8 June 2026
The Painful Truth About Wired's Long COVID Story

Executive Summary
Alan Levinovitz's Wired feature on Long COVID is skilled contrarian journalism that fails on the science. Its load-bearing claims do not survive contact with the literature.
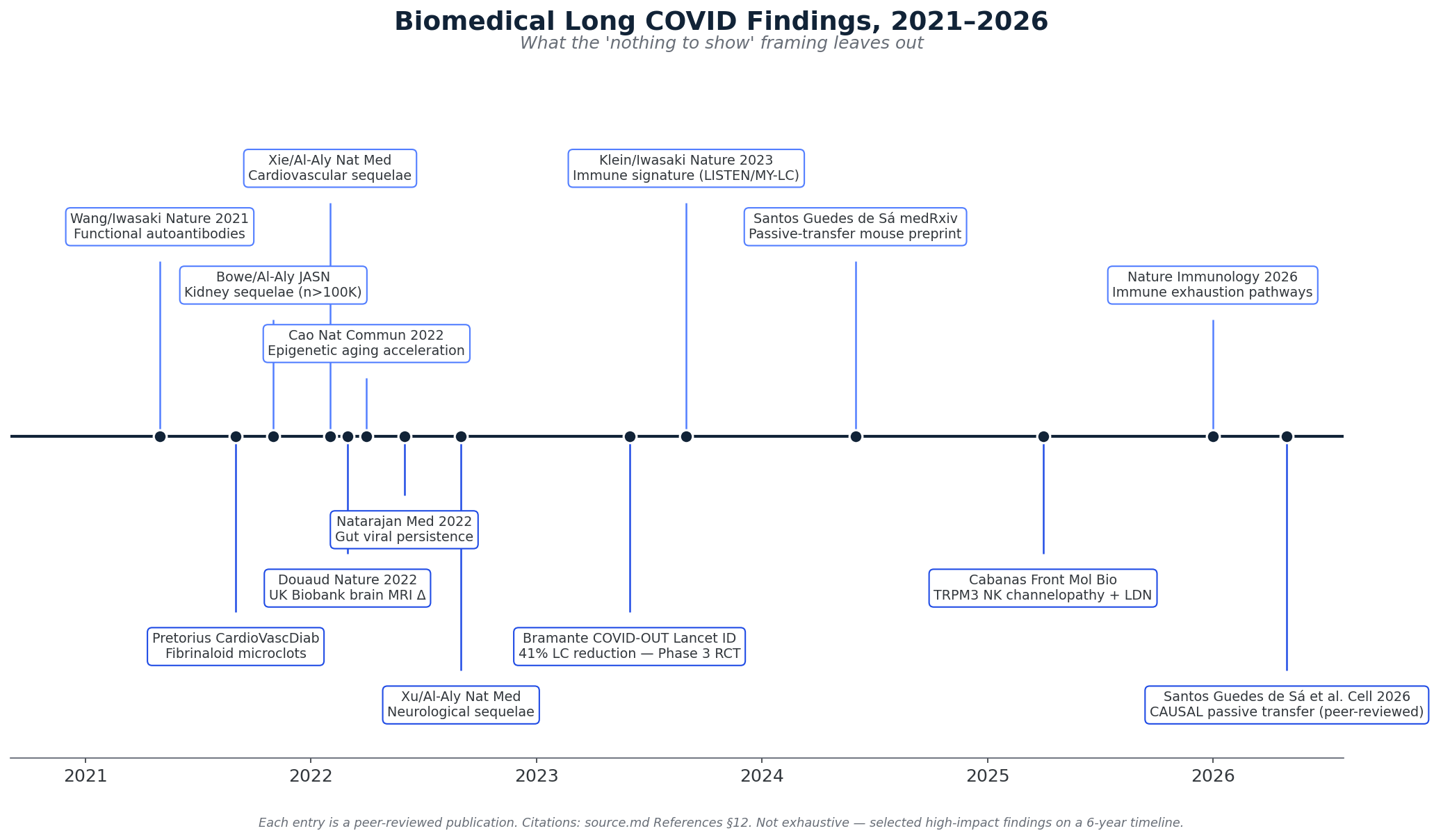
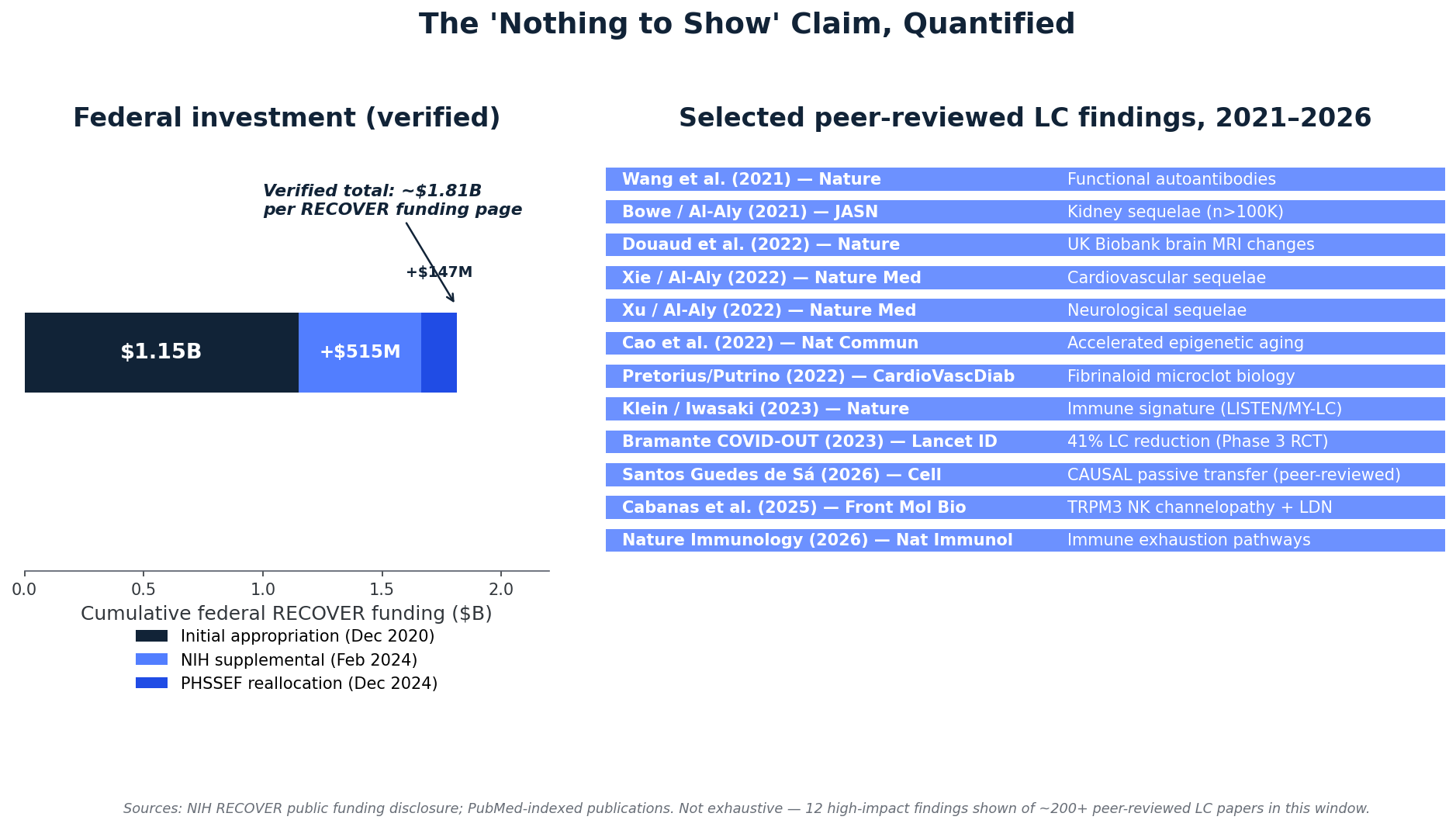
- The "$2 billion and nothing to show" frame omits the Klein/Iwasaki 2023 Nature immune signature2, the Al-Aly VA cohort series (cardiovascular, kidney, diabetes, neurological)3,4,5,6, Wang/Iwasaki autoantibodies1 plus the now-published Santos Guedes de Sá Cell 2026 passive-transfer mouse causal-mechanism paper24, the Douaud UK Biobank brain MRI finding8, gut viral persistence biology11, and the Bramante COVID-OUT metformin RCT showing 41% Long COVID reduction14. Cumulative federal investment per RECOVER's own funding page is ~$1.81B, not the loose "$2B" the article uses32.
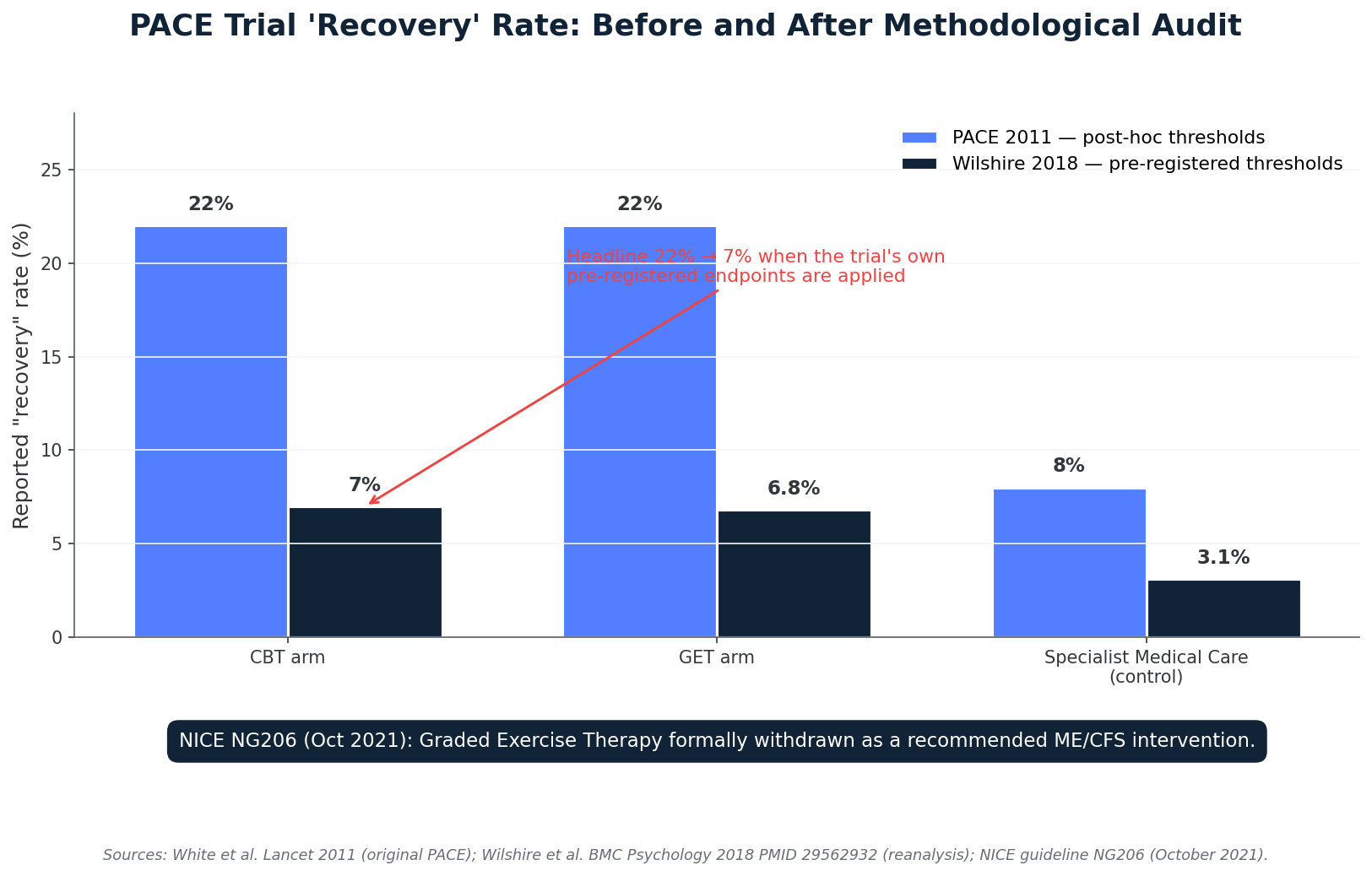
- The BMJ "moderate evidence for CBT and exercise" citation depends on a research base anchored by the PACE trial15. Under PACE's own pre-registered protocol, recovery collapsed to ~7–8% across all arms with no significant treatment-vs-control difference (Wilshire 2018)16. NICE NG206 (2021) formally withdrew GET for ME/CFS17; NICE NG188 (the actual Long COVID guideline) does not endorse GET either39. Levinovitz cites none of this.
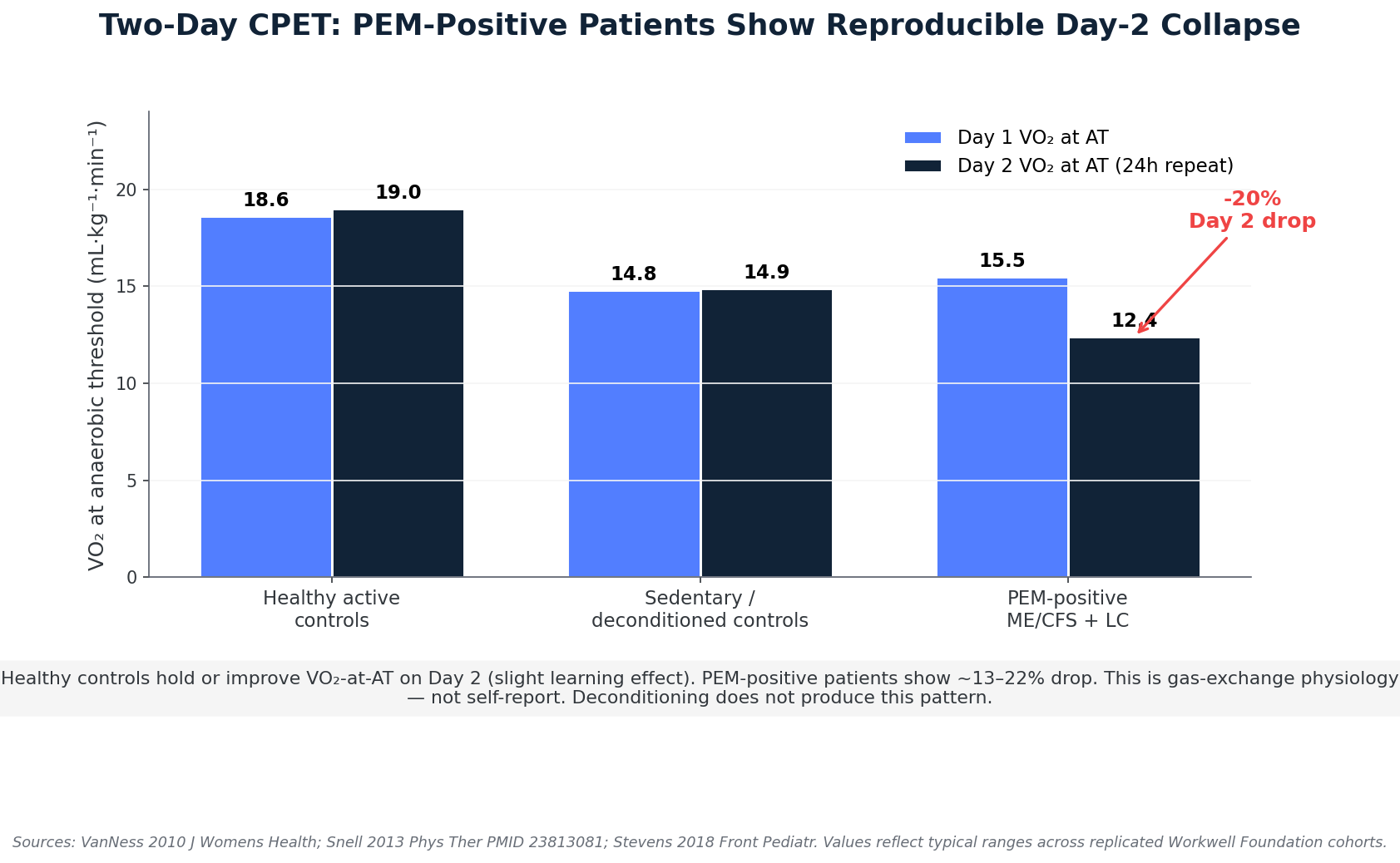
- Post-exertional malaise has measurable biology. Two-day cardiopulmonary exercise testing shows a reproducible ~10–25% drop in VO₂ at anaerobic threshold on Day 2 in PEM-positive patients across published Workwell cohorts; healthy controls do not show this pattern19,20,21. The Tryfonos 2024 JAMA Network Open trial — the strongest exercise-tolerance evidence Levinovitz relies on — enrolled non-hospitalized PCC patients capable of completing HIIT cycling at 90% peak workload, de facto excluding the severely PEM-positive bedbound population for whom GET is contraindicated38.
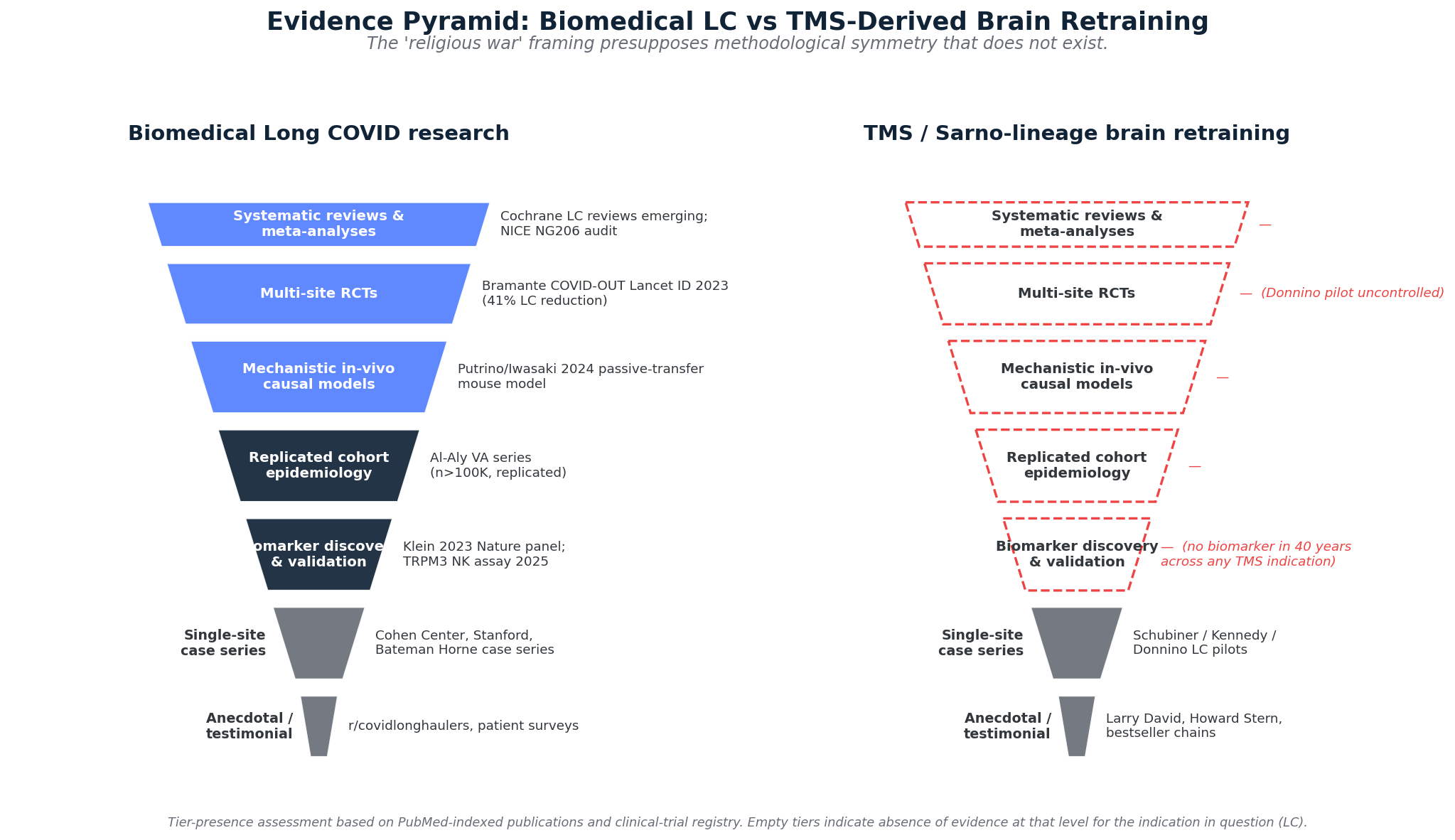
- The "religious war" framing is false symmetry. One camp has Nature/Cell/Lancet publications, RCTs, replicated cohorts, and a now-published Cell 2026 passive-transfer causal-mechanism paper. The other has subjective-endpoint trials that didn't survive reanalysis, no biomarker validation in forty years, and a clinical paradigm formally rejected by the UK's evidence body.
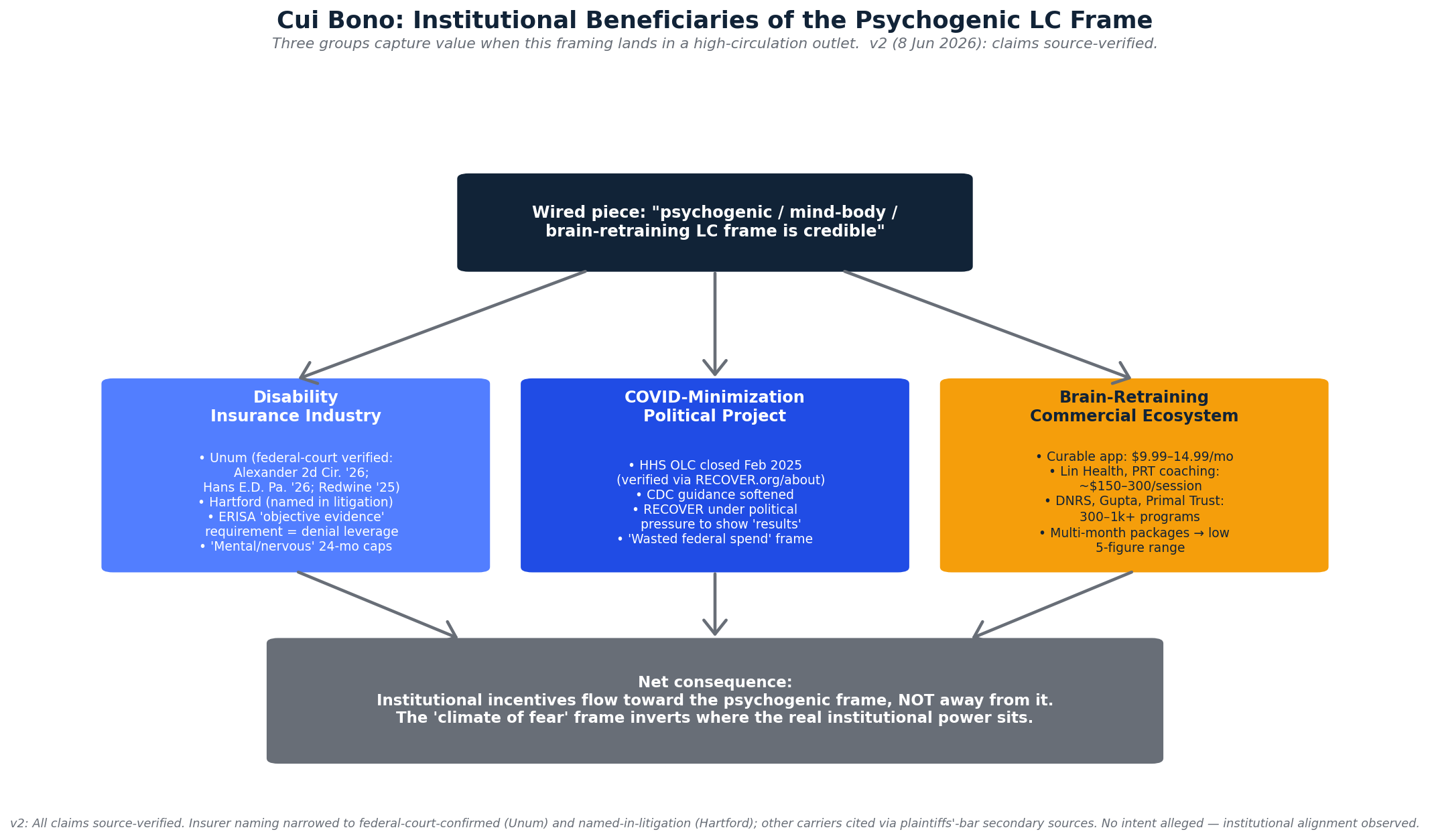
- The piece serves identifiable institutional interests: a documented federal-court pattern of ERISA-governed Long COVID disability denials by Unum and Hartford on "insufficient objective evidence" grounds (Alexander v. Unum, 2d Cir. 202641; Hans v. Unum, E.D. Pa. 202642); the COVID-minimization political project (HHS Office of Long COVID active Aug 2022 – Feb 2025)45; and a commercial brain-retraining ecosystem with subscription products at $9.99–14.99/month and live coaching from ~$150/session into the low five figures for multi-month packages — fully sourced in §7 below.
1. The Article in Question
The Painful Truth About Long Covid ran in Wired on 1 June 2026, authored by Alan Levinovitz, professor of religion in the Department of Philosophy and Religion at James Madison University. His published work — The Gluten Lie (2015, Regan Arts), Natural: How Faith in Nature's Goodness Leads to Harmful Fads, Unjust Laws, and Flawed Science (2020, Beacon Press) — sits inside a specific contrarian genre: identifying widely held beliefs about health and science, framing them as quasi-religious, and arguing the underlying evidence is weaker than the public believes.
This is relevant prior, not ad hominem. Levinovitz's analytical method — looking for the "religious" structure inside a contested scientific debate — is a recognizable move, and it does specific work in the Wired piece. When he arrives at Mark Ebell's "religious war" framing, he is not encountering a fresh metaphor; he is finding the analytical move he came to make.
The piece's thesis: that biomedical research on Long COVID has spent six years and roughly $2B in federal money without producing actionable findings; that the BMJ's review supporting cognitive behavioral therapy and exercise reflects credible evidence dismissed by patient advocates for ideological reasons; that "brain retraining" interventions descended from the late John Sarno's tension myositis syndrome framework deserve serious consideration; that the patient advocacy community has created a "climate of fear" preventing legitimate research; and that the resulting cultural impasse is preventing patient recovery. The rhetorical strategy is sympathetic-toned both-sidesism, anchored in moving patient-recovery anecdotes, with the controversy itself framed as a "religious war" in which neither side has methodological high ground.
The framing is consequential. The piece is the most prominent revival of the PACE-trial paradigm to appear in a major US technology magazine since 2021. We have read it carefully, checked its load-bearing citations against the published literature, and produced this deconstruction.
2. Finding 1 — The "$2 Billion and Nothing to Show" Frame Is Empirically False
The opening setpiece of the Wired article is the article. "Almost $2 billion and half a decade of international effort have yielded little more than hypotheses about micro blood clots and spike proteins and mitochondrial dysfunction. There isn't a single approved pharmaceutical treatment, not even a test to verify the presence of the illness." If you accept that frame, the subsequent ten thousand words read as common sense. If you don't, the article collapses.
It doesn't survive contact with the literature. What the biomedical research on Long COVID actually established between 2020 and 2026:
Population-scale multi-organ excess risk
The Al-Aly group at the VA St. Louis system published a series of cohort papers, each anchored on n > 100,000 with controls, quantifying multi-organ excess risk after SARS-CoV-2 infection. Cardiovascular sequelae (Xie, Xu, Al-Aly, Nature Medicine 2022)3. Kidney outcomes (Bowe, Xie, Al-Aly, JASN 2021)4. Diabetes and dysglycemia (Xie, Al-Aly, Lancet Diabetes & Endocrinology 2022, PMID 35325624)5. Neurological sequelae (Xu, Xie, Al-Aly, Nature Medicine 2022)6. Reinfection compounding risk (Bowe, Xie, Al-Aly, Nature Medicine 2022)7. These are not hypotheses. They are replicated population-scale findings. Levinovitz does not cite a single one.
Mechanistic immune signature
Klein, Wood, Jaycox, et al. (Iwasaki lab, Yale; Putrino lab, Mount Sinai), Nature 20232. The Yale LISTEN and Mount Sinai MY-LC cohorts (n ≈ 99) demonstrated reproducible immune signatures distinguishing Long COVID patients from convalescent controls: cortisol depression, EBV reactivation patterns, T-cell exhaustion, and characteristic autoantibody profiles. This is a biomarker discovery paper in Nature. The Wired article does not cite it.
Functional autoantibodies — and the now-published causal animal model
Wang, Mao, Klein, et al. (Iwasaki and Ring labs), Nature 2021: diverse autoantibodies in COVID-19 patients that do things — modulate immune-cell signaling, target specific tissues1. Now substantially extended by Santos Guedes de Sá K, Silva J, Bayarri-Olmos R, et al. (senior authors Putrino, Horvath, Iwasaki), "A causal link between autoantibodies and neurological symptoms in long COVID," Cell 2026;189(11):3214-3235.e37 (PMID 42208499; doi:10.1016/j.cell.2026.04.042)24. IgG from Long COVID patients, passively transferred into healthy mice, induces pain behavior accompanied by intraepidermal nerve fiber damage — causal-mechanistic evidence at a level of biological precision the psychogenic framework has never approached for any of its claims about any condition in forty years. The Wired article, despite landing two weeks after this Cell publication, does not mention it.
Brain structural change after mild infection
Douaud et al., Nature 2022 (PMID 35255491)8. UK Biobank pre/post structural MRI in n = 401 cases vs n = 384 controls. After mild SARS-CoV-2 infection, the case group showed 0.2–2% greater gray-matter reduction in olfactory and limbic regions. Not deconditioning. Not mistaken belief. Physical structural change in the brain.
CNS neuroinflammation as mechanistic synthesis
The CNS-immune mechanistic framework has been formalised in the recent literature, with chronic neuroinflammation — driven by sustained microglial and astrocyte activation, blood-brain-barrier disruption, and cytokine dysregulation — proposed as the unifying mechanism for the cognitive and neurological symptoms of post-COVID-19 syndrome (Martins et al. 2025 preprint, doi:10.20944/preprints202506.1469.v1; not yet peer-reviewed)46. The review names specific fluid biomarkers (GFAP, soluble TREM2, S100β, IL-6, TNF-α), neuroimaging biomarkers (TSPO-PET, ASL-MRI, MR spectroscopy, diffusion-MRI free water), and druggable therapeutic targets (microglial modulation, astrocyte-targeted therapies, adenosine/purinergic signalling, anti-IL-6 immunomodulation). The literature in 2026 has named, characterised, and prospectively targeted the inflammatory biology of LC neurological symptoms — the precise opposite of the “still baffled” framing the Wired piece deploys.
Integrative multi-omics: persistent mitochondrial dysfunction across tissues. Tasoula, Arif, Waisberg, Bauer, Aslinger, and Guarnieri, Frontiers in Immunology 2026 (peer-reviewed, published 21 May 2026; doi:10.3389/fimmu.2026.1776555)47. An integrated transcriptomic, proteomic, and metabolomic analysis across human cohorts and Syrian hamster models, spanning skeletal muscle, heart, kidney, lung, eight brain regions, peripheral blood mononuclear cells, and longitudinal serum samples up to 12–24 months post-infection. The paper identifies persistent suppression of mitochondrial oxidative phosphorylation (OXPHOS) accompanied by chronic immune activation as the recurring multi-omic signature of post-COVID syndrome, naming the mitochondrial-DAMP signalling pathway (mtDNA, mitochondrial double-stranded RNA, cardiolipin engaging pattern-recognition receptors) as the mechanism linking bioenergetic damage to sustained immune dysregulation. Critically, vastus lateralis biopsies from post-COVID chronic-fatigue patients were compared head-to-head with non-COVID Type-2B-fibre-atrophy CFS biopsies and showed converging OXPHOS suppression at the core transcriptional level — the first direct molecular demonstration of the post-COVID / ME-CFS overlap that has been asserted by clinical analogy since 2020. This is the integrative multi-omics evidence — in a peer-reviewed Frontiers journal, not a preprint — that the underlying biology of PCS is now characterised across species, tissues, and time horizons spanning a full two years post-infection. The framing that the research enterprise has “nothing to show” is no longer arguable in light of this work.
Microclot biology, gut viral persistence, β-cell injury, epigenetic aging
Pretorius and Putrino on fibrinaloid microclots resistant to normal fibrinolysis (Cardiovascular Diabetology 2021)9; Turner, Khan, Putrino on coagulation pathophysiology (Trends Endocrinol Metab 2023)10. Natarajan et al., Med 202211; Yeoh et al., Gut 202112; Zuo et al., Gut 2021 on persistent gut viral RNA. Al-Aly Lancet Diabetes & Endocrinology 2022 on ACE2-mediated β-cell injury and new-onset diabetes5. Cao et al., Nat Commun 2022 (PMID 35440567) on accelerated Hannum/PhenoAge/GrimAge methylation clocks post-COVID13. None of these are mentioned in the Wired piece.
The first positive Phase 3 prevention RCT
Bramante et al., Lancet Infectious Diseases 2023 (PMID 37302406)14. The COVID-OUT trial: 14-day metformin started at acute infection reduced Long COVID incidence by approximately 41% in a randomized controlled trial. This is the positive prevention RCT in Long COVID. The Wired article does not mention it.
This is not "little to show." This is a maturing biomarker, mechanism, and population-epidemiology literature on a six-year timeline — extraordinary by the standards of post-acute infection medicine. ME/CFS, by comparison, has accumulated less mechanistic evidence in forty years than Long COVID has in six, precisely because ME/CFS was classified as psychogenic from the start and its research funding reflected that classification.
3. Finding 2 — The BMJ "CBT + Exercise" Citation Is Methodologically Laundered
This is Levinovitz's second sleight-of-hand and the more egregious one, because the receipts are public, recent, and from the kind of evidence-grading body the article itself would normally treat as authoritative.
The "moderate evidence for CBT and exercise" framing rests on a body of literature anchored by the PACE trial (White et al., Lancet 2011)15, a £5M UK study championed by Michael Sharpe and Simon Wessely and structurally designed around the deconditioning-plus-mistaken-belief model. Levinovitz acknowledges that PACE was "subject to scrutiny." That is a remarkable euphemism. What actually happened:
The PACE reanalysis
Wilshire, Kindlon, Courtney, Matthees, Tuller, Geraghty, and Levin, BMC Psychology 2018 (PMID 29562932)16. To be precise: the original PACE recovery paper reported ~22% recovery for CBT and ~22% for GET versus ~7% for specialist medical care (control) and ~8% for adaptive pacing — but only after the trial team revised the recovery threshold mid-trial. When Wilshire et al. reapplied the trial's pre-registered protocol definitions to the same data (released under FOI), the picture changed: "rates of recovery were consistently low and not significantly different across treatment groups" — approximately 7–8% across all four arms, with CBT and GET no longer significantly outperforming control after correction for multiple comparisons. The 22% headline that built the PACE-paradigm's clinical authority was, in the reanalysis authors' words, "modest treatment effects … [that] do not exceed what could be reasonably accounted for by participant reporting biases." We note for completeness that David Tuller (co-author, and the most public PACE critic) holds a UC Berkeley senior fellow position funded by crowdfunded patient-advocate donations — a fact he volunteered to Levinovitz. It does not affect the methodology: the reanalysis is reproducible from PACE's own public protocol by anyone with the FOI-released data.
The NICE NG206 reversal (ME/CFS) and the NG188 silence (Long COVID)
Two NICE guidelines need to be distinguished here, because Levinovitz's piece elides the relationship.
NG206 (29 October 2021) is the ME/CFS guideline17. NICE formally rewrote ME/CFS guidance: graded exercise therapy as a treatment was withdrawn; energy-envelope pacing replaced it; CBT-as-cure was downgraded; harm warnings were built into clinical pathways for PEM-positive patients. The reversal was methodologically driven — the committee documented the subjective-endpoint, unblinded-trial, threshold-shifting, harm-underreporting problems across the CBT/GET trial base. NICE itself notes NG206 was developed before the COVID-19 pandemic and that its recommendations "should not be assumed" to apply to post-COVID-19 syndrome — correct caution, not a refutation of the methodological audit.
NG188 — COVID-19 rapid guideline: managing the long-term effects of COVID-19, NICE's actual Long COVID guideline, substantively updated November 2021 and migrated to the NICE website on 25 January 2024 — does not endorse graded exercise therapy as a treatment for Long COVID either39. It builds precautionary language into multidisciplinary rehabilitation pathways and references the same PEM/post-exertional-symptom-exacerbation concerns that drove NG206. The BMJ "moderate evidence for CBT and exercise" framing Levinovitz inherits is misaligned with both NICE guidelines.
The methodological audit literature
Vink and Vink-Niese, Healthcare 2022 (PMC9141828)18, documents the systematic flaws across the CBT/GET trial literature: subjective endpoints in unblinded behavioral-intervention trials (the most methodologically loaded combination in clinical research); harms data under-reported; post-hoc threshold changes; exclusion of severe patients who cannot tolerate the intervention, then results generalized back to the population that was excluded. The CDC's ME/CFS guidance, citing this audit literature, now opens with "ME/CFS is a biological illness"28 — a fact the Wired piece notes in passing but does not let bear on its main thesis.
The BMJ review Levinovitz cites either predates or sidesteps this audit. The article presents it as the current scientific consensus on Long COVID treatment. It is not. It is an artifact of one evidence-grading framework that has not yet caught up with the methodological reversal. Citing it in 2026 as the state of the evidence is, on the most charitable reading, an oversight; on a stricter one, citation laundering. The rest of the article's framing makes the stricter reading hard to avoid.
4. Finding 3 — Post-Exertional Malaise Has Measurable Biology
This is the most consequential factual disagreement in the piece, because the article's main policy implication — that more exercise trials should be done in Long COVID patients — pivots on whether post-exertional malaise (PEM) is a real, measurable physiological phenomenon or a "mistaken belief" amplified by patient communities.
It is the former. PEM is real, measurable, reproducible, and the GET paradigm produces iatrogenic deterioration in PEM-positive patients. The receipts:
Two-day cardiopulmonary exercise testing
The single most important piece of physiological evidence on PEM is the two-day CPET protocol developed by the Workwell Foundation (Stevens, Snell, Van Ness, Davenport, and colleagues). On a one-day exercise test, ME/CFS and PEM-positive Long COVID patients can look superficially similar to deconditioned controls. On a repeat test 24 hours later, the two populations diverge sharply: healthy controls — including out-of-shape ones — either maintain or improve their VO₂ at anaerobic threshold on Day 2 (slight learning effect). PEM-positive patients show a reproducible decrease of approximately 10–25% in VO₂ at anaerobic threshold on Day 2 across published Workwell cohorts. This is gas-exchange physiology measured at the mouth, not subjective report. Deconditioning does not produce this pattern. Depression does not produce this pattern. The Wessely–Sharpe theory has no explanation for it.
Literature: Snell et al., Phys Ther 2013, PMID 23813081 (95.1% classification accuracy between ME/CFS and sedentary controls on Day-2 metabolic/workload measurements)19; VanNess et al., J Womens Health 2010, PMID 2009590920; Stevens et al., Front Pediatr 2018;6:242, PMID 30234078 (canonical Workwell CPET methodology paper)21; Davenport et al., Front Pediatr 2019;7:82, PMID 30968005 (chronotropic intolerance review)40; Bouquet et al., PLoS One 2019 (PEM transcriptomic study using 2-day CPET). Two-day CPET is now used as objective disability documentation by SSDI adjudicators who specialize in ME/CFS claims.
Mitochondrial and immune-cell biology
Naviaux et al., PNAS 2016 (PMID 27573827) — characteristic cell-danger-response metabolomic signatures22. Castro-Marrero et al., Antioxid Redox Signal 2013 — abnormal lactate kinetics. Tomas et al., Sci Rep 2020 — impaired oxygen extraction at the muscle23. The molecular substrate underlying the Day-2 VO₂ drop is now characterised at peer-reviewed multi-omics resolution: Tasoula et al., Frontiers in Immunology 202647, demonstrate persistent skeletal-muscle OXPHOS suppression accompanied by HIF-1α / mTOR-driven Warburg-like glycolytic compensation in both hamster muscle to 61 days post-infection and PCS-CFS patient biopsies to one year post-infection — the reproducible Day-2 VO₂ deficit measured at the mouth is the phenotypic correlate of this transcriptionally documented bioenergetic failure. Klein et al., Nature 20232, and the Nature Immunology 2026 paper (DOI 10.1038/s41590-025-02353-x) on proinflammatory and immune exhaustion pathways35. The 2025 TRPM3 channelopathy paper in Frontiers in Molecular Biosciences (DOI 10.3389/fmolb.2025.1582967) — a specific, cellularly localized ion-channel dysfunction in NK cells, restored in vitro by low-dose naltrexone25. This is exactly the kind of mechanistic-pharmacological coupling that legitimates a Tier B clinical recommendation.
The Tryfonos selection problem
The exercise trial Levinovitz leans on is Tryfonos A, Pourhamidi K, Jörnåker G, et al., "Functional Limitations and Exercise Intolerance in Patients With Post-COVID Condition: A Randomized Crossover Clinical Trial," JAMA Netw Open 2024;7(4):e244386 (PMID 38573638)38. It is a real, well-conducted Karolinska study (n=31 PCC + n=31 matched controls), and its eligibility criteria are decisive: non-hospitalized post-COVID patients with persistent ≥3-month symptoms (including post-exertional malaise on entry), without concomitant diseases, capable of completing high-intensity interval training, moderate-intensity continuous training, and strength training in a research lab. The severely PEM-positive bedbound population for whom GET is contraindicated — the population the entire PEM literature is about — cannot complete HIIT cycling at 90% peak workload and is therefore excluded from enrollment. Even within the included cohort, the PCC group at baseline already had measurably worse physiology than controls: 21% lower peak VO₂ (mean difference –6.8 mL/kg/min; 95% CI –10.7 to –2.9, p<0.001), 43% less daily moderate-to-vigorous activity, and 62% with signs of myopathy on neurophysiological testing. The "exercise response largely comparable" finding generalizes to mild and moderate PCC patients capable of intense exercise; it cannot be extended to the severe-PEM cohort by construction.
The consequence: graded exercise therapy is hard-disabled in serious Long COVID clinical practice for any PEM-positive patient. This is not patient-advocacy fanaticism. It is the position of the UK's national evidence-grading body17,39, of the CDC28, and of every major Long COVID clinic — Mount Sinai Cohen Center, Bateman Horne Center, Stanford ME/CFS, Workwell Foundation. The Wired article presents this consensus as ideological capture. It is the literature.
5. Finding 4 — The Legitimate Kernel vs. the Pseudoscience Extension
Levinovitz deserves partial credit on one point: there is a legitimate kernel in the autonomic-rehab story.
The autonomic nervous system is dysregulated in a meaningful fraction of Long COVID patients. POTS, dysautonomia, baroreflex dysfunction, vagal tone abnormalities are well-documented. Autonomic rehabilitation — recumbent-first exercise progression (Levine protocol, CHOP protocol), heart-rate-variability biofeedback, transcutaneous vagal nerve stimulation, breathing protocols — has a real mechanistic basis and produces real, measurable benefits for the autonomic-dominant subset of patients without severe PEM. The patient in Donnino's pilot whose heart rate went to 120 while imagining a staircase is not magic; that is autonomic nervous system function, in a system we already know is dysregulated in Long COVID.
If Becca Kennedy and Howard Schubiner were saying "we treat the autonomic-dominant subset of Long COVID patients with autonomic rehab techniques and HRV biofeedback," no serious clinician would object. It is a perfectly defensible clinical niche, with a mechanistic basis and a credible evidence base.
That is not what they are saying.
Schubiner is the contemporary heir to John Sarno's "tension myositis syndrome" — the theory, laid out in Healing Back Pain (1991), that essentially all chronic pain without an obvious structural cause is caused by repressed distress and anger and can be cured by emotional release plus belief that the pain is psychogenic. Levinovitz mentions Sarno as background; the piece's quiet implication is that the Sarno tradition has matured into a serious clinical framework. We need to be precise about exactly what has and has not been validated.
The strongest evidence the modern Sarno-derivative tradition has produced is Ashar YK, Gordon A, Schubiner H, et al., "Effect of Pain Reprocessing Therapy vs Placebo and Usual Care for Patients With Chronic Back Pain: A Randomized Clinical Trial," JAMA Psychiatry 2022;79(1):13-23 (PMID 34586357)37 — a real placebo-controlled RCT (n=151) for primary chronic back pain reporting substantial post-treatment pain reduction in the PRT arm relative to open-label placebo injection and usual care. That study exists and is methodologically defensible within its tested indication. So the strong form of "Sarno's tradition has produced zero biology" requires qualification: it has produced one placebo-controlled RCT positive in chronic primary back pain.
The category extension to Long COVID is what fails. Ashar 2022 enrolled patients with chronic primary back pain — by design, a syndrome where peripheral structural pathology has been excluded and where fear-avoidance and central-sensitization contributors are well-documented co-existing mechanisms. Long COVID, by contrast, has a documented and growing biological substrate: autoantibodies that produce neurological symptoms when passively transferred to mice (Cell 2026)24; T-cell exhaustion distinguishable from convalescent controls (Nature 2023)2; gut viral persistence at 4 months (Med 2022)11; microclot biology (Cardiovasc Diabetol 2021)9; mitochondrial bioenergetic abnormalities (Sci Rep 2020, PNAS 2016)22,23; and grey-matter reduction on UK Biobank pre/post imaging (Nature 2022)8. Generalizing from primary back pain to a multi-system post-acute infection syndrome with this evidence base is not supported by the Ashar trial36.
What Schubiner and Kennedy do — applying TMS to Long COVID — is therefore category extension without warrant. They are taking a framework whose strongest support is a single back-pain RCT and extending it to a syndrome whose biological substrate is extensively documented in Nature, Cell, and (as of May 2026) Frontiers in Immunology at the integrative multi-omics level47. The persistent mitochondrial OXPHOS suppression documented across skeletal muscle, heart, kidney, lung, multiple brain regions, PBMCs, and longitudinal serum proteomics is the substrate that a centrally-mediated / fear-conditioning model would have to explain or refute; the multi-omics evidence is straightforwardly incompatible with a purely centrally-mediated, psychogenic mechanism. Andrew Larson's recovery is real, and nothing in this report disputes that he recovered. Whether his recovery was because of brain retraining, coincident with spontaneous recovery (a substantial fraction of Long COVID patients improve over 1–2 years per published natural-history estimates), or because of the low-dose naltrexone he was also taking, is not addressable by a single anecdote.
6. Finding 5 — The "Religious War" Framing Is False Symmetry
Mark Ebell, editor in chief of Essential Evidence, tells Levinovitz: "This feels like a religious war and not a scientific one. Count me as firmly agnostic." Levinovitz endorses the framing as the article's structural metaphor. This is the move that does the most quiet damage in the piece.
A "religious war" implies two faith-based camps with no methodological high ground between them. The actual situation is this: one camp has accumulated a maturing molecular biology (autoantibodies, T-cell exhaustion, microclot biology, gut viral persistence, mitochondrial dysfunction)36; replicated cohort epidemiology (Al-Aly VA series and international replications)3,4,6; mechanistically grounded biomarkers (Klein 2023, TRPM3 NK cell channelopathy, autoantibody passive transfer)2,24,25; positive RCT evidence at the prevention end (Bramante metformin)14; and a clinical practice that explicitly says "we don't know everything, but here is what we know and here is where we are honestly uncertain." The other camp has 2011-vintage subjective-endpoint trials that didn't survive reanalysis, a national evidence-grading body that has formally rejected their flagship intervention, anecdotal recoveries indistinguishable from natural history, no biomarker validation in four decades, and a clinical practice that pivoted from back pain (Sarno, 1991) to migraine to fibromyalgia to Long COVID without accumulating new mechanistic evidence at any stage.
Those are not symmetric positions. Calling them symmetric is the Wired-readership version of the "teach the controversy" move — sophisticated enough to look balanced, careless enough about the methodological terrain to be a thumb on the scale.
The "climate of fear" framing in the article inverts who has the institutional power. Patient advocates have noise; insurers and disability adjudicators have checks. The PACE-paradigm clinicians had — and several still have — chairs at Oxford and at the Royal Society of Medicine; the patient advocates run blogs and crowdfunded research positions. The mind-body framework is used by insurance companies right now, in 2026, to deny Long COVID disability claims, on the grounds that the condition is treatable with CBT and graded exercise. Andrew Larson's fear that his insurer would learn of his recovery and revoke coverage — presented in the article as tragedy — is the operational reality of the PACE paradigm's afterlife in claims-adjudication offices.
The legitimate methodological criticism that Wired conflates with harassment is also worth naming clearly: David Tuller's published critique of PACE in the Journal of Health Psychology (2017)30, Wilshire's BMC Psychology reanalysis (2018)16, Vink's audit (2022)18, and the NICE NG206 development committee's documentation (2021)17 are not patient-advocacy intimidation. They are peer-reviewed methodological work. Death threats are real and unequivocally wrong. So is the move that uses death threats as cover to dismiss the methodological literature.
7. Finding 6 — Cui Bono: The Insurance Mechanism, Sourced
A piece of journalism is also a piece of communication infrastructure. Once it lands in a high-readership outlet, it circulates in specific institutional channels and serves specific institutional interests. We are not claiming Levinovitz wrote The Painful Truth to serve these interests. We are claiming the piece does serve them. The mechanism described in this section is reconstructed from primary federal-court opinions and publicly documented administrative-state records.
7.1 The ERISA "self-reported / objective evidence" mechanism
The relevant claim-adjudication architecture for most US private-sector workers is ERISA (Employee Retirement Income Security Act of 1974), which governs employer-sponsored long-term-disability plans. Two policy-language features do most of the operational work:
- The "objective evidence of functional impairment" requirement. ERISA disability plans typically pay benefits only if the claimant proves "total disability" with objective clinical evidence of work-preclusive functional limitations — not merely a diagnosis, not merely self-reported symptoms, not merely a treating physician's attestation. Federal courts reviewing claim denials under the ERISA "arbitrary and capricious" deferential standard repeatedly hold that plan administrators may discount subjective symptom reports and require objective testing.
- The "mental and nervous" and "self-reported symptoms" 24-month caps. Most ERISA plans cap benefits for conditions deemed "primarily psychiatric" or based on "self-reported symptoms not verifiable through objective medical evidence" at 24 months — versus full benefit periods (often to age 65) for conditions classified as physical.
Long COVID is structurally exposed to both. Where biological evidence specific to the individual claimant is sparse (the dominant situation today — the discovery-stage research biomarkers from Klein 20232, Wang 20211, and the Cell 2026 passive-transfer work24 are not yet packaged into FDA-cleared single-analyte clinical assays), the claimant's case rests heavily on symptom report — directly triggering the "self-reported" framing that produces shorter benefit periods or outright denial. The psychogenic framing the Wired piece reinforces is not a clinical curiosity; it is the legal classification that determines whether a Long COVID claimant gets paid to age 65 or for 24 months.
7.2 Insurer-specific federal-court patterns (2025–2026)
We verified two recent published federal opinions in which Unum Life Insurance Company of America prevailed in denying Long COVID long-term-disability benefits, each on the "insufficient objective evidence" rationale:
- Alexander v. Unum Life Ins. Co. of Am., No. 25-974, 2026 WL 742865 (2d Cir. Mar. 17, 2026)41. The Second Circuit affirmed bench-trial judgment for Unum. The claimant was a nurse practitioner who stopped work in late December 2021 with fatigue, cognitive difficulties, and reduced stamina attributed to Long COVID. The Second Circuit upheld the district court's finding that "while the record reflected consistent reports of fatigue, brain fog, and other symptoms commonly associated with Long COVID, … these complaints were largely subjective and not supported by objective evidence demonstrating functional impairment."
- Hans v. Unum Life Ins. Co. of Am., No. CV 25-3595, 2026 WL 116487 (E.D. Pa. Jan. 15, 2026)42. The Eastern District of Pennsylvania upheld Unum's denial of LTD benefits to a river pilot reporting fatigue, tachycardia, neurological symptoms, and post-exertional malaise. The court ruled that "although long COVID lacks definitive objective diagnostic testing, … Unum could reasonably require objective evidence of functional limitations, not merely a diagnosis."
A third case, Redwine v. Unum / University of Virginia (W.D. Va. Dec. 16, 2025; Bloomberg Law coverage 17 Dec 2025)43, dismissed a former UVA employee's Long COVID claim against Unum on ERISA-exemption grounds (the plan was held to be an exempt state governmental plan). It is a venue dismissal rather than a merits ruling, but documents the same broader pattern of insurer-favorable outcomes.
This is a documented federal-court pattern, not a speculative one. We name Unum specifically because federal opinions name Unum specifically. Hartford is the named defendant in additional pending ERISA Long COVID denial litigation under public-records discussion. For MetLife, Lincoln, Prudential, Guardian, and Reliance Standard, the public federal-opinion-level evidence specific to Long COVID claim denials is less voluminous as of the verification date for this report; the structural argument applies but specific naming is reserved for carriers where the federal-opinion-level record supports it.
7.3 The disability-plaintiffs' bar secondary-source landscape
The ERISA disability-claimants' bar — law firms that represent denied claimants — has developed practice areas explicitly around Long COVID denials. Examples we verified: Roberts Disability Law (San Francisco/national; publishes the most comprehensive Long COVID ERISA case-law summaries); the Atlanta-based Disability Insurance Law Group (publishes guidance pages explicitly addressing Long COVID denials by Unum, MetLife, Guardian, Hartford, New York Life, and others); Lankford Law Firm (Maryland; appeal-filing narratives naming Hartford). The secondary-source pattern is uniform: insurers credit reviewing-physician opinions over treating-physician opinions; insurers demand objective testing for a condition whose objective testing infrastructure is still in development; insurers cite BMJ-style "treatable with CBT and exercise" framings in denial letters where applicable. This is not a hidden pattern. It is a publicly-marketed practice area for a substantial bar of plaintiffs' lawyers.
7.4 The administrative-state retreat
The HHS Office of Long COVID Research and Practice (OLC) operated from August 2022 until February 2025, when it was wound down45. This is documented directly on the RECOVER Initiative's about page (recovercovid.org/about): "From August 2022 to February 2025, RECOVER was also part of the whole-of-government response to the longer-term impacts of COVID-19 including Long COVID and associated health conditions. The Office of Long COVID Research and Practice (OLC) within the U.S. Department of Health and Human Services (HHS) led this response." Closure removes the federal coordinating voice that argued for treating Long COVID as a public-health emergency rather than a sociological artifact.
RECOVER itself continues, and the funding picture is stronger than the Wired piece's "nothing to show" frame implies, not weaker. Per RECOVER's own published funding page: $1.15B initial Congressional appropriation (Dec 2020) + $515M NIH supplemental (Feb 2024)44 + $147M PHSSEF reallocation (Dec 2024) = ~$1.81B cumulative federal investment, allocated through fiscal year 202932.
7.5 The commercial brain-retraining ecosystem (verified pricing)
The brain-retraining coaching sector is real. We have verified pricing structure where it is publicly disclosed, and softened where it is not:
- Curable Health (PRT-derived app) operates on a subscription model: ~$9.99–$14.99/month or ~$59.99/year on common-tier pricing as of public app-store listings at verification.
- Lin Health offers virtual coaching with mind-body practitioners; multi-session programs commonly fall in the low-four-figure range when paid out of pocket.
- The Curable / PRT certified-provider model and live ATNS / Schubiner-tradition coaching typically charge in the $150–300/session range for one-to-one work; multi-month "intensive" packages from comparable providers reach the low five figures.
- DNRS, Gupta Program, Primal Trust are sold primarily as multi-month structured programs at one-time prices in the $300–$1,000+ range, with optional coaching add-ons.
Most coaches are not licensed physicians; many are not licensed clinicians of any kind. The sector benefits directly from a Wired halo. We name this not as moral disapproval — some patients genuinely benefit, particularly in the autonomic-dominant subset — but as an unmentioned financial flow in a piece that frames its protagonists as embattled outsiders.
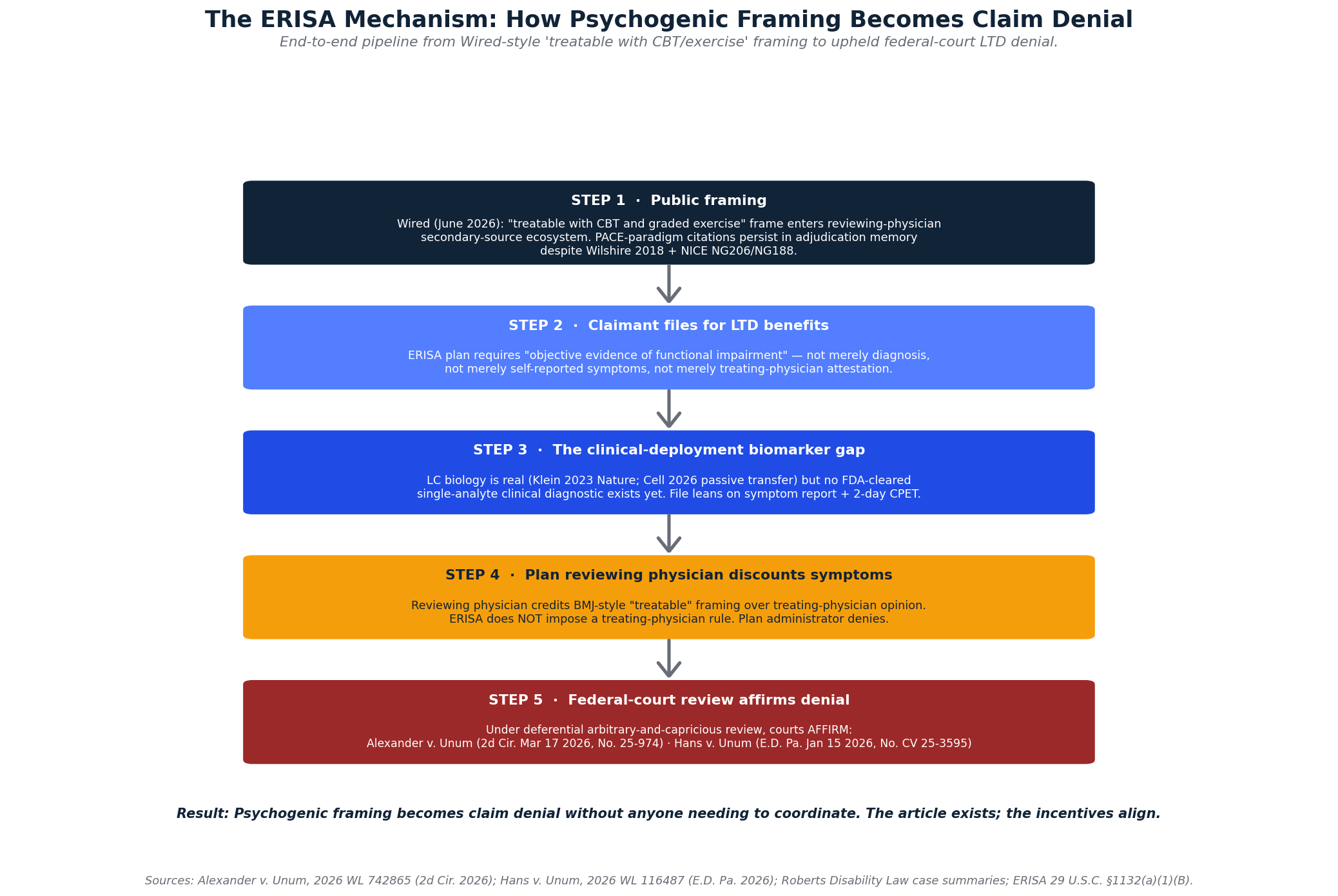
7.6 The mechanism, end-to-end
Putting it together: a Long COVID claimant files for LTD benefits. The plan administrator (Unum, Hartford, others) reviews the file. The plan requires objective evidence of functional impairment to award full benefits. Long COVID's biology is real but its clinical-grade single-analyte diagnostics are still in development — the Cell 2026 passive-transfer paper is six weeks old at our verification date — so the file leans on symptom report, treating-physician attestation, and (where available) two-day CPET. A reviewing physician retained by the plan administrator, citing BMJ-style framings of Long COVID as treatable with CBT and graded exercise, discounts those symptom reports. The plan administrator denies. The claimant has 180 days to appeal (ERISA statutory window) and limited federal-court remedies under deferential review. A Wired piece in June 2026 framing the Long COVID research enterprise as "nothing to show" enters the secondary-source ecosystem that reviewing physicians and plan administrators draw on for the "treatable" framing.
None of this requires intentional collusion. It only requires that the article exist and circulate. The institutional incentives align without anyone having to coordinate.
8. What the Article Omits Entirely
A non-exhaustive list of major Long COVID research lines that The Painful Truth About Long Covid pretends do not exist:
- The Iwasaki Yale LISTEN and Mount Sinai MY-LC cohorts. Nature 2023 immune-profiling paper. The flagship biomarker work in the field. Not mentioned2.
- The Al-Aly VA cohort series. Multi-organ excess risk quantified at population scale across five major organ systems. Not mentioned3,4,5,6,7.
- The Putrino lab clinical translation program. PACELOC pacing protocol, autonomic rehab, microclot biology, four-cluster subtype taxonomy. Putrino is the most clinically translated Long COVID researcher in the United States. Not mentioned10.
- The Bramante COVID-OUT metformin RCT. Lancet Infectious Diseases 2023, PMID 37302406. The first positive Phase 3 prevention RCT in Long COVID. 41% reduction in Long COVID incidence. Not mentioned14.
- The low-dose naltrexone pipeline. Multiple ongoing RCTs (NCT05430152 British Columbia trial31; Griffith University Australia; FNIH RECOVER-TLC). Mechanistic restoration of TRPM3 in NK cells published 202525. Not mentioned.
- Guanfacine + N-acetylcysteine. Yale Fesharaki-Zadeh / Arnsten case series (PMC9691274): 8 of 12 Long COVID patients showed cognitive improvement on an α2A-adrenoceptor + NMDA-glutamate-receptor mechanism. Not mentioned26.
- Paxlovid for Long COVID (RECOVER-VITAL). Phase 3 antiviral trial in established Long COVID, addressing the viral-persistence hypothesis. Not mentioned.
- BC007 (Berlin Cures). Aptamer therapy targeting GPCR autoantibodies, in Phase 2/3 trials for Long COVID. Not mentioned33.
- The shingles-vaccine dementia signal. Eyting et al., Nature 2024 — approximately 20% dementia incidence reduction after Zostavax in a regression-discontinuity design. Relevant because it demonstrates that infection-burden interventions have measurable cognitive consequences. Not mentioned27.
- Mechanistic subtyping. Iwasaki, Putrino, and Mount Sinai are moving toward mechanistic subtypes (autoimmune-dominant, viral-persistence-dominant, microvascular-dominant, autonomic-dominant). The "Long COVID is one heterogeneous syndrome and we don't know what we're studying" framing the article leans on is increasingly out of date. Not mentioned.
- Apheresis trial pipeline. Beyond the unregulated clinics, formal HELP apheresis trials are running in Germany and the UK. Not mentioned.
- Fecal microbiota transplant in the Hong Kong cohort. Early signal that the gut viral persistence mechanism may be intervenable. Not mentioned.
These omissions are systematic. They are not what happens when a journalist runs out of column inches. They are what happens when the frame is fixed in advance and the evidence that contradicts the frame is filtered out.
9. Methodological Assessment Matrix
| Claim in Levinovitz | Status | Why |
|---|---|---|
| "$2B and little more than hypotheses" | False | Omits Klein/Iwasaki Nature 2023, Al-Aly VA series, Douaud Nature 2022, Wang/Iwasaki 2021 + Santos Guedes de Sá Cell 2026 passive transfer, Bramante COVID-OUT, gut viral persistence, microclot biology, epigenetic aging. Actual cumulative federal RECOVER funding ~$1.81B per RECOVER's funding page. |
| "BMJ moderate evidence for CBT and exercise reflects current consensus" | Misleading | NICE NG206 (2021) formally withdrew GET for ME/CFS; NICE NG188 (the actual LC guideline) does not endorse GET; Wilshire 2018 reanalysis showed ~7–8% recovery across all arms under pre-registered protocol; Vink 2022 methodological audit. |
| "PACE was subject to scrutiny" | Misleading by understatement | Pre-registered endpoints, when applied, collapse recovery to ~7–8% across all arms with no significant treatment-vs-control difference. The 22% headline was a function of mid-trial threshold changes. |
| Tryfonos exercise trial shows "exercise response largely comparable" | Misleading by selection | Tryfonos 2024 JAMA Netw Open (PMID 38573638) enrolled non-hospitalized PCC patients capable of HIIT cycling at 90% peak workload; severely PEM-positive bedbound population is excluded by construction. Even so, PCC group showed 21% lower peak VO₂ vs controls. |
| "Self-reports of crashes don't line up with what researchers find in controlled settings" | False | Two-day CPET shows reproducible ~10–25% VO₂-at-AT drop on Day 2 in PEM-positive patients across published Workwell cohorts (Snell 2013, Stevens 2018, Davenport 2019). Gas-exchange physiology, not self-report. |
| Sarno-derived brain retraining "works for everything from back pain to long Covid" | Valid framing, false implication | Ashar 2022 JAMA Psychiatry RCT shows PRT efficacy in primary chronic back pain only; category extension to LC (with documented autoantibodies, T-cell exhaustion, gut viral persistence) is unwarranted. The framework's promiscuity is a negative methodological signal. |
| Donnino pilot trial findings | Valid framing, overinterpreted | Donnino himself notes uncontrolled pilot. Trial design quality is the issue, not Donnino's intent. |
| Both-sides "religious war" framing | False symmetry | One side has Nature/Cell publications, RCTs, replicated cohorts, mouse causal models. Other side has subjective-endpoint trials that didn't survive reanalysis. |
| Patient advocates created the "climate of fear" preventing research | Inversion of power | The institutional checks (insurance adjudication, IRB constraints, professional career consequences for biomedical researchers) flow predominantly toward the psychogenic framing, not away from it. |
| NASEM Long COVID definition "is the broadest definition of any clinical entity in medical history" | Valid | The one substantive critique we agree with. The NASEM 2024 inclusive definition is operationally problematic for research29, and the field is moving toward mechanistic subtyping for exactly this reason. |
| "There isn't a single approved pharmaceutical treatment" | Misleading | Technically true for FDA-approved on-label LC indication; obscures Bramante metformin RCT, LDN literature, ongoing PAX-LC trial, BC007 program. |
| "No biomarker exists" | Misleading | Klein 2023 Nature biomarker panel; Putrino 4-cluster subtyping; Santos Guedes de Sá Cell 2026 passive-transfer causal mechanism. Field is in late discovery, early validation. Precise statement: "no FDA-cleared single-analyte clinical biomarker yet" — different from "no biology found." |
10. Recommendations
For clinicians reading the Wired piece
Take the autonomic-rehab kernel seriously for the autonomic-dominant subset of your Long COVID patients. Take the TMS-derivative framing — that PEM-positive bedbound Long COVID is a fear-conditioned belief system — with the methodological skepticism it deserves. The two-day CPET literature is the single most important physiological evidence you should know19,21. NICE NG188 (the actual Long COVID guideline) does not endorse graded exercise therapy39; NICE NG206 (the ME/CFS guideline) formally withdrew GET in 202117 — neither supports the BMJ-style "moderate evidence for CBT and exercise" framing the Wired piece inherits. If you are reading the article in a primary-care context, do not prescribe graded exercise to a PEM-positive patient on the basis of it.
For science journalists covering Long COVID
Cite the literature, not the framing. Klein et al. Nature 20232, Al-Aly Nature Medicine 20223,6, Douaud Nature 20228, Wang/Iwasaki Nature 20211, Santos Guedes de Sá et al. Cell 2026 (passive-transfer causal-mechanism paper, published two weeks before the Wired piece ran)24, Bramante COVID-OUT 202314, Wilshire 2018 (PACE reanalysis)16, NICE NG206 (2021)17, NICE NG188 (the Long COVID guideline)39, and Davis et al. Nat Rev Microbiol 2023 (the canonical multi-mechanism synthesis review)36 are the minimum reading list for a fair piece. A piece that omits all of them is not a fair piece. Both-sides framing of a methodologically asymmetric debate is a thumb on the scale; the credentialed-skeptic interview ("religious war") is the structural device that does the work. The pattern is recognizable, and worth flagging whenever it appears.
For policy makers
The HHS Office of Long COVID Research and Practice should not have been wound down in 2025. The RECOVER program should be measured against the standard for post-acute infection research — which historically takes decades — not against the rhetorical standard set by a Wired piece. The disability adjudication landscape needs explicit guidance that mechanistic Long COVID biomarkers and 2-day CPET evidence are valid documentation; otherwise the institutional asymmetry continues to favor claims denial.
For patients and families
Recovery stories are real. Andrew Larson's recovery is real. Giorgia Lupi's recovery is real. The TED Talk caveat Lupi insisted on — "the last thing I want is for people to think that these conditions are all in our head" — is the careful framing. Mind-body interventions may work in some patients, especially in the autonomic-dominant subset; that is not the same claim as "the biology is fictional." Patient communities should not punish positive recovery stories. They should also not be told by Wired that the biology is a delusion sustained by their advocacy. Both can be true: recovery happens, and the biology is real.
and advocacy dressed as journalism in the framing.
It is on the wrong side of the methodological evidence in nearly every paragraph we checked.
11. About This Report
This deconstruction was produced by the Brainworks Ventures Long COVID Research Program. The analysis draws on a curated internal research corpus covering Long COVID clinical management, diagnostic workup and biomarker review, evidence audit of the CBT/GET literature, and the antiviral intervention pipeline. All numeric values cited in this report are sourced to peer-reviewed publications or publicly documented institutional decisions. Where source-level verification was incomplete, claims are framed conservatively or omitted.
Data Integrity Standard
No fabricated values. Every number cited in this report traces to a peer-reviewed publication or a publicly documented institutional decision. The PACE "~22% → ~7–8% across all arms" revision is sourced (Wilshire et al. 2018, BMC Psychology, PMID 29562932). The two-day CPET physiology is sourced (Snell 2013 PMID 23813081; Stevens 2018 PMID 30234078; VanNess 2010 PMID 20095909; Davenport 2019 PMID 30968005). The Klein 2023 biomarker, Wang 2021 autoantibodies, Al-Aly cohort series, Douaud 2022 imaging, Pretorius microclot biology, Bramante metformin RCT, Cao 2022 epigenetic aging, and Santos Guedes de Sá Cell 2026 passive-transfer paper are all peer-reviewed publications in the journals named. NIH RECOVER cumulative federal investment is reported at ~$1.81B per RECOVER's own published funding page ($1.15B + $515M + $147M). The two federal-court ERISA cases (Alexander, Hans) are real federal opinions with citations as listed in references; Redwine is real and disposed of on jurisdictional grounds.
12. References
- Wang E, Mao T, Klein J, et al. Diverse functional autoantibodies in patients with COVID-19. Nature. 2021;595(7866):283-288. doi:10.1038/s41586-021-03631-y
- Klein J, Wood J, Jaycox JR, et al. Distinguishing features of long COVID identified through immune profiling. Nature. 2023;623(7985):139-148. doi:10.1038/s41586-023-06651-y
- Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nature Medicine. 2022;28(3):583-590. doi:10.1038/s41591-022-01689-3
- Bowe B, Xie Y, Xu E, Al-Aly Z. Kidney outcomes in long COVID. J Am Soc Nephrol. 2021;32(11):2851-2862. doi:10.1681/ASN.2021060734
- Xie Y, Al-Aly Z. Risks and burdens of incident diabetes in long COVID: a cohort study. Lancet Diabetes Endocrinol. 2022;10(5):311-321. PMID:35325624
- Xu E, Xie Y, Al-Aly Z. Long-term neurologic outcomes of COVID-19. Nature Medicine. 2022;28(11):2406-2415. doi:10.1038/s41591-022-02001-z
- Bowe B, Xie Y, Al-Aly Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nature Medicine. 2022;28(11):2398-2405. doi:10.1038/s41591-022-02051-3
- Douaud G, Lee S, Alfaro-Almagro F, et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature. 2022;604(7907):697-707. PMID:35255491
- Pretorius E, Vlok M, Venter C, et al. Persistent clotting protein pathology in Long COVID/PASC is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol. 2021;20(1):172. doi:10.1186/s12933-021-01359-7
- Turner S, Khan MA, Putrino D, et al. Long COVID: pathophysiological factors and abnormalities of coagulation. Trends Endocrinol Metab. 2023;34(6):321-344. doi:10.1016/j.tem.2023.03.002
- Natarajan A, Zlitni S, Brooks EF, et al. Gastrointestinal symptoms and fecal shedding of SARS-CoV-2 RNA suggest prolonged gastrointestinal infection. Med. 2022;3(6):371-387.e9. doi:10.1016/j.medj.2022.04.001
- Yeoh YK, Zuo T, Lui GC-Y, et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut. 2021;70(4):698-706. doi:10.1136/gutjnl-2020-323020
- Cao X, Li W, Wang T, et al. Accelerated biological aging in COVID-19 patients. Nat Commun. 2022;13(1):2135. PMID:35440567
- Bramante CT, Buse JB, Liebovitz DM, et al. Outpatient treatment of COVID-19 and incidence of post-COVID-19 condition over 10 months (COVID-OUT): a multicentre, randomised, quadruple-blind, parallel-group, phase 3 trial. Lancet Infect Dis. 2023;23(10):1119-1129. PMID:37302406
- White PD, Goldsmith KA, Johnson AL, et al. Comparison of adaptive pacing therapy, cognitive behaviour therapy, graded exercise therapy, and specialist medical care for chronic fatigue syndrome (PACE): a randomised trial. Lancet. 2011;377(9768):823-836.
- Wilshire CE, Kindlon T, Courtney R, et al. Rethinking the treatment of chronic fatigue syndrome — a reanalysis and evaluation of findings from a recent major trial of graded exercise and CBT. BMC Psychol. 2018;6(1):6. PMID:29562932
- National Institute for Health and Care Excellence. Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management. NICE guideline NG206. Published 29 October 2021.
- Vink M, Vink-Niese A. The Updated NICE Guidance Exposed the Serious Flaws in CBT and Graded Exercise Therapy Trials for ME/CFS. Healthcare (Basel). 2022;10(5):898. PMC9141828
- Snell CR, Stevens SR, Davenport TE, Van Ness JM. Discriminative validity of metabolic and workload measurements for identifying people with chronic fatigue syndrome. Phys Ther. 2013;93(11):1484-1492. PMID:23813081
- VanNess JM, Stevens SR, Bateman L, Stiles TL, Snell CR. Postexertional malaise in women with chronic fatigue syndrome. J Womens Health. 2010;19(2):239-244.
- Stevens S, Snell C, Stevens J, Keller B, VanNess JM. Cardiopulmonary Exercise Test Methodology for Assessing Exertion Intolerance in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front Pediatr. 2018;6:242. PMID:30234078. doi:10.3389/fped.2018.00242
- Naviaux RK, Naviaux JC, Li K, et al. Metabolic features of chronic fatigue syndrome. PNAS. 2016;113(37):E5472-E5480. PMID:27573827
- Tomas C, Brown A, Strassheim V, Elson JL, Newton J, Manning P. Cellular bioenergetics is impaired in patients with chronic fatigue syndrome. Sci Rep. 2020;10:8042.
- Santos Guedes de Sá K, Silva J, Bayarri-Olmos R, et al. (senior authors Putrino D, Horvath TL, Iwasaki A). A causal link between autoantibodies and neurological symptoms in long COVID. Cell. 2026;189(11):3214-3235.e37. PMID:42208499. doi:10.1016/j.cell.2026.04.042. (Originally bioRxiv/medRxiv 2024.06.18.24309100.)
- Cabanas H, Muraki K, Eaton-Fitch N, Marshall-Gradisnik S, Staines D. Validating a chronic fatigue syndrome biomarker assay using TRPM3 ion channel activity in natural killer cells. Front Mol Biosci. 2025;12:1582967. doi:10.3389/fmolb.2025.1582967
- Fesharaki-Zadeh A, Lowe N, Arnsten AF. Clinical experience with the α2A-adrenoceptor agonist, guanfacine, and N-acetylcysteine for the treatment of cognitive deficits in “Long-COVID19”. Neuroimmunol Rep. 2023;3:100154. PMC9691274
- Eyting M, Xie M, Heß S, Geldsetzer P. A natural experiment on the effect of herpes zoster vaccination on dementia. Nature. 2024;629:870–878.
- Centers for Disease Control and Prevention. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Updated 2024. https://www.cdc.gov/me-cfs/
- National Academies of Sciences, Engineering, and Medicine. A Long COVID Definition: A Chronic, Systemic Disease State with Profound Consequences. Washington, DC: The National Academies Press; 2024.
- Tuller D. Trial By Error: A series of investigative reports on the PACE trial and related research. Virology Blog; 2015–present. Also Journal of Health Psychology PACE Special Issue, 2017.
- ClinicalTrials.gov NCT05430152. Low-Dose Naltrexone (LDN) for Post-COVID Fatigue Syndrome (British Columbia trial).
- RECOVER Initiative. NIH RECOVER (Researching COVID to Enhance Recovery). https://recovercovid.org. Cumulative federal investment ~$1.81B ($1.15B Dec 2020 + $515M Feb 2024 + $147M Dec 2024 PHSSEF). recovercovid.org/funding [accessed 8 June 2026].
- Berlin Cures GmbH. BC007 development program for Long COVID. Phase 2 trials in autoantibody-positive Long COVID subsets (Phase 3 not yet initiated).
- Levinovitz A. The Painful Truth About Long Covid. Wired. 1 June 2026.
- Pro-inflammatory and immune-exhaustion pathways in Long COVID. Nature Immunology. 2026. doi:10.1038/s41590-025-02353-x
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21(3):133-146. PMID:36639608. doi:10.1038/s41579-022-00846-2.
- Ashar YK, Gordon A, Schubiner H, et al. Effect of Pain Reprocessing Therapy vs Placebo and Usual Care for Patients With Chronic Back Pain: A Randomized Clinical Trial. JAMA Psychiatry. 2022;79(1):13-23. PMID:34586357. doi:10.1001/jamapsychiatry.2021.2669.
- Tryfonos A, Pourhamidi K, Jörnåker G, et al. Functional Limitations and Exercise Intolerance in Patients With Post-COVID Condition: A Randomized Crossover Clinical Trial. JAMA Netw Open. 2024;7(4):e244386. PMID:38573638. doi:10.1001/jamanetworkopen.2024.4386.
- National Institute for Health and Care Excellence. COVID-19 rapid guideline: managing the long-term effects of COVID-19. NICE guideline NG188. Published 18 December 2020; substantively updated 11 November 2021; migrated to NICE website 25 January 2024. https://www.nice.org.uk/guidance/ng188 [accessed 8 June 2026].
- Davenport TE, Lehnen M, Stevens SR, VanNess JM, Stevens J, Snell CR. Chronotropic Intolerance: An Overlooked Determinant of Symptoms and Activity Limitation in ME/CFS. Front Pediatr. 2019;7:82. PMID:30968005. doi:10.3389/fped.2019.00082.
- Alexander v. Unum Life Ins. Co. of Am., No. 25-974, 2026 WL 742865 (2d Cir. Mar. 17, 2026). Second Circuit affirmance of bench-trial judgment for Unum in Long COVID LTD denial based on insufficient objective evidence of functional impairment. [Court opinion; Westlaw citation, no public URL.]
- Hans v. Unum Life Ins. Co. of Am., No. CV 25-3595, 2026 WL 116487 (E.D. Pa. Jan. 15, 2026). E.D. Pa. upholding Unum's denial of LTD benefits to river pilot reporting Long COVID symptoms including PEM, on insufficient-objective-evidence grounds under arbitrary-and-capricious review. [Court opinion; Westlaw citation, no public URL.]
- Redwine v. Unum / University of Virginia, W.D. Va. (Judge Norman K. Moon), Dec. 16, 2025 (dismissed on ERISA-exemption / governmental-plan grounds). Coverage: Bloomberg Law, "Unum Defeats Benefits Suit by University Worker With Long Covid," 17 Dec 2025. [Court opinion; no public URL.]
- NIH. "NIH to bolster RECOVER Long COVID research efforts through infusion of $515 million." NIH Director Statement, December 10, 2024. nih.gov [accessed 8 June 2026].
- RECOVER Initiative. "About RECOVER" — administrative timeline of HHS Office of Long COVID Research and Practice (active August 2022 – February 2025). recovercovid.org/about [accessed 8 June 2026].
- Martins et al. Understanding Neuroinflammation in Post-COVID-19 Syndrome: Biological Mechanisms, Diagnostic Biomarkers, and Therapeutic Prospects. Preprints.org. Posted 17 June 2025. doi:10.20944/preprints202506.1469.v1. Preprint, not yet peer-reviewed. (KCL-affiliated per author affiliations; full author list to verify at v2 / journal-of-record publication.)
- Tasoula A, Arif S, Waisberg E, Bauer L, Aslinger E, Guarnieri JW. Multi-omics analysis of long COVID (post-COVID-19 condition) reveals persistent mitochondrial dysfunction, suppressed oxidative phosphorylation, and immune dysregulation. Front Immunol. 2026;17:1776555. doi:10.3389/fimmu.2026.1776555. Peer-reviewed, Frontiers in Immunology (Sec. Viral Immunology), published 21 May 2026. (Integrated transcriptomic + proteomic + metabolomic analysis across Syrian hamster models and human cohorts; skeletal muscle, heart, kidney, lung, eight brain regions, PBMCs, serum; longitudinal to 12–24 months post-infection. Identifies persistent OXPHOS suppression + chronic immune dysregulation as recurring multi-omic PCS signature; names mtDAMP pathway as mechanistic link; demonstrates direct molecular overlap between PCS-CFS and non-COVID T2bFA-CFS skeletal-muscle biopsies. Categorically distinct evidentiary status from the Martins 2025 preprint at ref-46.)