Legislative Strategy to Reform American Healthcare

Part III: From Analysis to Action
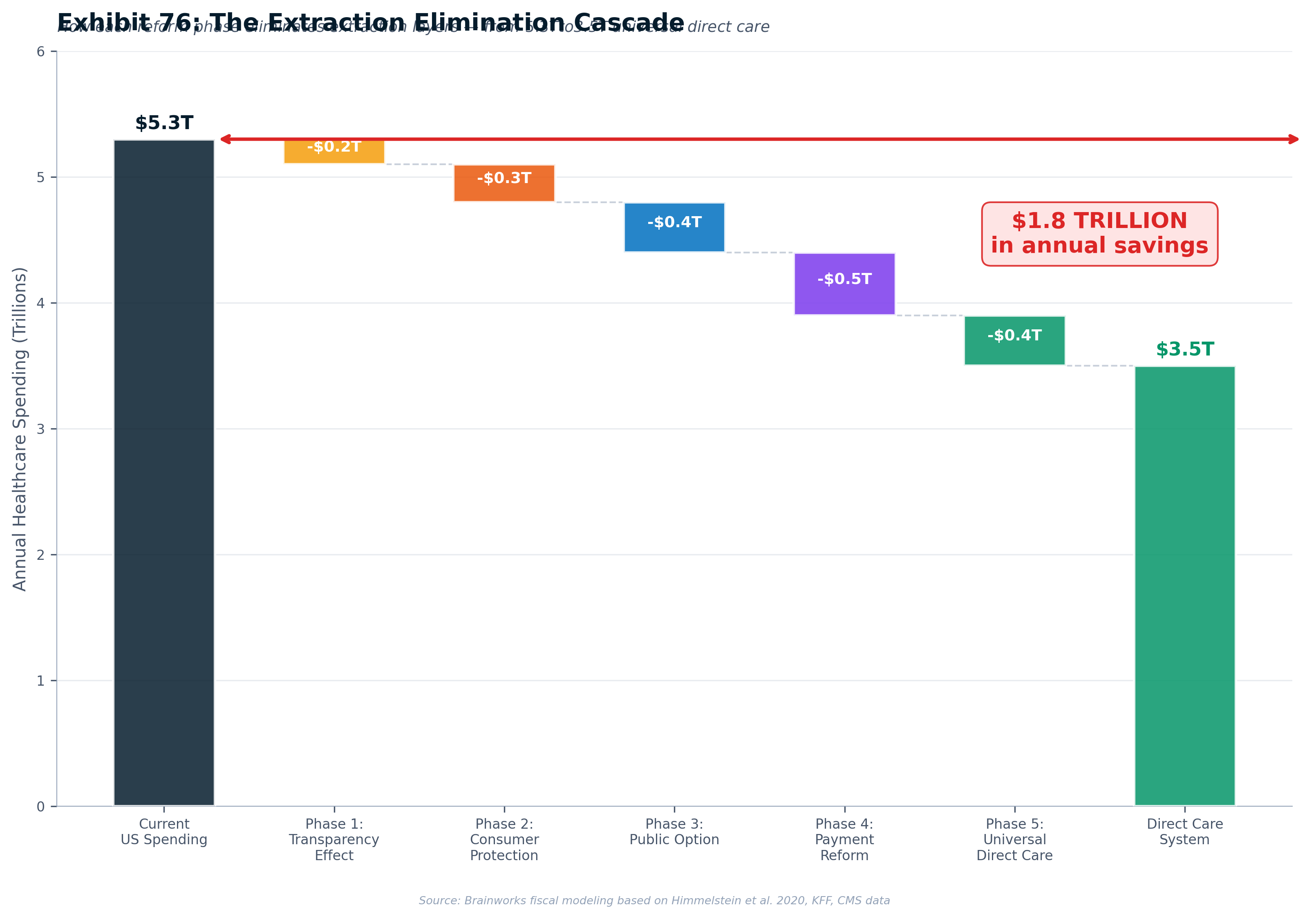
Volumes I and II of this report documented how $1.8+ trillion in annual healthcare spending is consumed by administrative waste, misaligned incentives, and corporate consolidation rather than reaching patients. This Part III answers the question those volumes demanded: what do we do about it?
The answer is a five-phase legislative strategy designed to reform America's healthcare cost crisis through state-level action — beginning with ten strategically selected states across the political spectrum, spreading through regional coalitions, and ultimately forcing federal reform through the sheer weight of demonstrated success. The strategy draws on every major lesson from healthcare reform history: Massachusetts Chapter 58's impossible coalition, Vermont's fatal financing divorce, CalCare's pulled floor vote, Colorado's ballot initiative catastrophe, and the New York Health Act's union paradox.
Critically, this is not a partisan agenda. Healthcare costs are America's single greatest competitive disadvantage — adding $15,000+ per worker in costs that German, Japanese, and Singaporean competitors simply do not bear. At 17.2% of GDP, American healthcare spending diverts $1.5–2 trillion annually from productive investment, suppresses entrepreneurship through "job lock," undermines military readiness (77% of young Americans are ineligible for service), and functions as a self-imposed trade barrier on every American export. Conservative, market-based reform models — from Indiana's HSA-based Healthy Indiana Plan to Singapore's MediSave system to Maryland's 47-year all-payer rate-setting track record — demonstrate that reform need not follow a single ideological template.
The phased approach — Transparency → Consumer Protection → Real Competition → Payment Reform → Universal Direct Care — ensures each step is independently valuable, politically achievable, and builds the institutional infrastructure and political constituency for the next. At full implementation, the Direct Care model is projected to deliver $30–60 billion in avoided annual cost growth in California and $10–20 billion in New York by reducing administrative overhead from 34% to under 5%, introducing real market competition, and redirecting waste to care. Note: These are avoided cost increases, not absolute spending reductions. Independent actuarial analysis (RAND/Milliman) is recommended before public use of any projection in this report.
Part III: Table of Contents
- New in v3.0
- Healthcare Costs as a National Competitiveness Crisis
- The Legislative Blueprint — A Five-Phase Strategy
- California — Leading the Transformation
- New York — Breaking the Senate Deadlock
- The National Map — Ten Reform-Ready States
- Lessons from the Battlefield — Why Reform Fails and How to Win
- Building the Movement — A Bipartisan Coalition
- The Campaign Timeline — From Research to Universal Care
- Conclusion — From Analysis to Action
- The Legal Fortress — ERISA, Constitutional Defense, and Litigation Strategy
- Implementation — Technology, Systems, and the HealthCare.gov Lesson
- Workforce Transition and Rural Health
- The AI-Personalized State Legislative Engine
- The Campaign Arsenal — Asset Inventory, Startup Guide, and AI-Accelerated Deployment
- Bridge to Part IV — Healthcare and AI Displacement
- Reference
- Bibliography
Chapter 16: Healthcare Costs as a National Competitiveness Crisis
Before examining the legislative strategy to reform American healthcare, it is essential to understand why reform is not merely a social policy objective but a national economic and security imperative. The data is unambiguous: America's healthcare cost crisis is the single largest self-imposed competitive disadvantage in the global economy.
The Employer Competitiveness Tax
Every American employer that provides health insurance pays a hidden tax that no competitor in Germany, Japan, Singapore, or China bears at anywhere near the same scale. In 2025, the average annual premium for employer-sponsored family coverage reached $25,572, with employers paying approximately 75% — or $19,179 per worker with family coverage. Single coverage averages $8,951, with employers covering ~$7,519. These costs are projected to rise 5.8–7.9% annually.
Compare this to America's major economic competitors:
| Country | Employer Health Cost/Worker | Mechanism |
|---|---|---|
| United States | $15,000–$16,000 | Employer-sponsored insurance premiums |
| France | ~$5,000–$6,000 | Social security contributions (~13% employer share) |
| Germany | ~$4,500–$5,500 | Payroll tax (~7.3% employer share) |
| Japan | ~$3,500–$4,500 | Social insurance (~5% employer share) |
| United Kingdom | ~$0 direct / ~$3,800 via tax | NHS funded through general taxation |
| South Korea | ~$2,500–$3,500 | National Health Insurance (~3.5% employer share) |
| Singapore | ~$1,500–$2,500 | MediSave (employer CPF contribution) |
| China | ~$1,000–$2,000 | Basic Medical Insurance (~6–10% employer) |
U.S. employers pay 3–10× more per worker for healthcare than competitors in every major economy. This is not a marginal difference — it is a structural competitive disadvantage embedded in the cost of every product and service produced in America.
The GM vs. Toyota Case: $1,525 Per Vehicle
The most powerful illustration of healthcare as competitive burden remains the General Motors case. Before its 2009 restructuring, GM spent $5.2 billion annually on health care, covering 1.1 million employees and retirees. Healthcare costs added approximately $1,525 per vehicle produced — more than GM spent on steel. Toyota's healthcare cost per vehicle in Japan? Approximately $150–200. Within two years of retirement, Toyota employees switched to Japan's national health plan at zero cost to the company.
GM CEO Rick Wagoner stated plainly: "The cost of health care in the U.S. is making American businesses extremely uncompetitive vs. our global counterparts." The $1,525 gap was equivalent to the cost of launching three additional new-model programs per year. This structural disadvantage contributed directly to GM's bankruptcy.
The Innovation Drain: $1.5–2 Trillion Diverted
The United States spends 17.2% of GDP on healthcare — nearly double the OECD average of 9.3% and roughly 50% more than the next-highest spender (Germany at 12.7%). In dollar terms, U.S. per capita health spending of $14,885 is almost $5,000 more than the next-highest country (Switzerland at ~$9,963) and roughly double the wealthy-country average.
The gap between U.S. spending (17.2%) and the average of peer nations (~10–12%) represents approximately $1.5–2 trillion annually — capital that in other countries flows to R&D, infrastructure, education, wages, and business investment. Every dollar consumed by administrative overhead, monopoly pricing, and misaligned incentives is a dollar not invested in the AI revolution, semiconductor manufacturing, clean energy, or any other domain of global competition.
The Administrative Overhead Crisis
A significant portion of America's healthcare cost excess is pure administrative waste. U.S. healthcare administrative costs per capita are $1,078 — approximately five times more than the average of other wealthy countries (~$200 per capita). The widely-cited Himmelstein et al. study estimated that $1.055 trillion (34.2% of total health expenditure) goes to administration — billing departments, prior authorizations, insurance interactions, and the 900+ private insurers each with different formularies, pre-authorization rules, and billing codes.
The average physician practice spends an estimated $110,000+ per year interacting with insurance companies. Physicians spend approximately two hours on administrative tasks for every one hour of patient care. Prior authorization processes alone cost the system an estimated $31 billion annually. This is not healthcare — it is bureaucracy masquerading as healthcare.
Real Wages Flat Since 1980: The Hidden Healthcare Tax on Workers
American workers have experienced stagnant real wage growth for over four decades — and healthcare costs are a primary culprit. When employers face 5–8% annual increases in health insurance premiums, those costs are absorbed by suppressing wage growth. The total compensation employers offer grows, but the growth is consumed by healthcare inflation rather than reaching workers' paychecks. In countries where healthcare costs are managed through national systems, employers can direct compensation growth to wages — giving workers in Germany, Japan, and Canada tangible annual raises that American workers do not receive.
Startup Suppression and "Job Lock"
The phenomenon of "job lock" — workers remaining in jobs primarily to maintain health insurance — represents a significant drag on labor market dynamism and entrepreneurship. Economist Brigitte Madrian's landmark study estimated that job lock reduces voluntary job mobility by 25%. A 2015 study found significantly higher business formation rates among workers who had just turned 65 (and gained Medicare eligibility) compared to those just under 65.
Denmark, which has universal healthcare, has higher levels of entrepreneurship than the United States. A 2020 study in Small Business Economics confirmed that universal healthcare programs positively influence entrepreneurial activities across countries. Every potential entrepreneur who stays in a corporate job because of healthcare coverage represents a lost startup, product, or innovation. Countries with universal systems effectively subsidize entrepreneurship by removing healthcare as a barrier to business formation.
Military Readiness: A National Security Emergency
America's population health crisis has become a national security emergency. The Department of Defense Military Health System budget for FY2026 is $63.9 billion — providing healthcare to 9.6 million beneficiaries through military treatment facilities and TRICARE.
But the deeper crisis is recruitment eligibility. 77% of young Americans (ages 17–24) would not qualify for military service without a waiver, according to the Pentagon's Qualified Military Available Study. The CDC confirms that 71% of young people would be unable to join the military if they wanted to. The top disqualification reasons — overweight/obesity (11%), drug and alcohol abuse (8%), and medical/physical health problems (7%) — are all upstream consequences of inadequate healthcare access, preventive care, nutrition, and mental health services.
Lieutenant General Mark Hertling stated: "The military has experienced increasing difficulty in recruiting soldiers as a result of physical inactivity, obesity, and malnutrition among our nation's youth. Not addressing these issues now will impact our future national security." No amount of defense spending can compensate for a population too unhealthy to serve.
Physician Burnout: The Brain Drain
The U.S. healthcare system's administrative complexity is driving a workforce crisis. Physician burnout rates remain at approximately 50%, with administrative burden consistently cited as a top driver. The AAMC projects a shortage of 37,800 to 124,000 physicians by 2034. Meanwhile, physicians in countries with simpler administrative systems (UK, Canada, Scandinavia) report lower burnout rates and spend significantly more time on direct patient care. The administrative burden of American healthcare is literally driving doctors out of medicine.
The Self-Imposed Trade Barrier
Every American export carries a healthcare surcharge. When a U.S. manufacturer ships goods overseas, the healthcare costs embedded in that product's labor are 3–10× higher than the healthcare costs embedded in the competing German, Japanese, or Chinese product. This functions as a self-imposed tariff on American competitiveness — one that no trade agreement can remedy because the source is domestic policy, not foreign barriers.
Small businesses face a disproportionate burden: they pay 8–18% more per employee for equivalent health coverage compared to large employers due to smaller risk pools. Only 56% of firms with 3–49 workers offer health insurance, versus 99% of firms with 200+ workers. The healthcare burden acts as a regressive tax on entrepreneurship, falling hardest on the smallest and newest firms — precisely the firms that create 65% of net new jobs.
Medical Debt: A Uniquely American Pathology
100 million Americans owe medical debt, totaling approximately $220 billion. An estimated 550,000 Americans file for bankruptcy annually due in part to medical bills — medical debt is the #1 cause of personal bankruptcy in the United States. This distinction is shared by no other developed nation. The concept of "medical bankruptcy" is essentially unknown in Canada, the UK, Germany, Japan, France, Australia, and most of the developed world.
National Competitiveness Scorecard
| Metric | United States | Germany | Japan | Singapore | China |
|---|---|---|---|---|---|
| Healthcare % of GDP | 17.2% | 12.7% | 10.7% | 4.1% | ~7% |
| Per capita spending | $14,885 | $8,540 | $5,250 | ~$3,000 | ~$900 |
| Employer cost/worker | $15,000+ | $4,500–$5,500 | $3,500–$4,500 | $1,500–$2,500 | $1,000–$2,000 |
| Admin cost per capita | $1,078 | ~$338 | ~$200 | Minimal | Minimal |
| Life expectancy | 77.5 yrs | 81.2 yrs | 84.6 yrs | 84.1 yrs | 78.6 yrs |
| Medical bankruptcies/yr | ~550,000 | ~0 | ~0 | ~0 | N/A |
| Universal coverage | No | Yes | Yes | Yes | Yes (basic) |
| Active labor market policy (% GDP) | ~0.1% | ~0.6% | ~0.3% | ~1.5% (SkillsFuture) | Growing |
Part III: Legislative Strategy to Reform American Healthcare
Chapter 17: The Legislative Blueprint — A Five-Phase Strategy
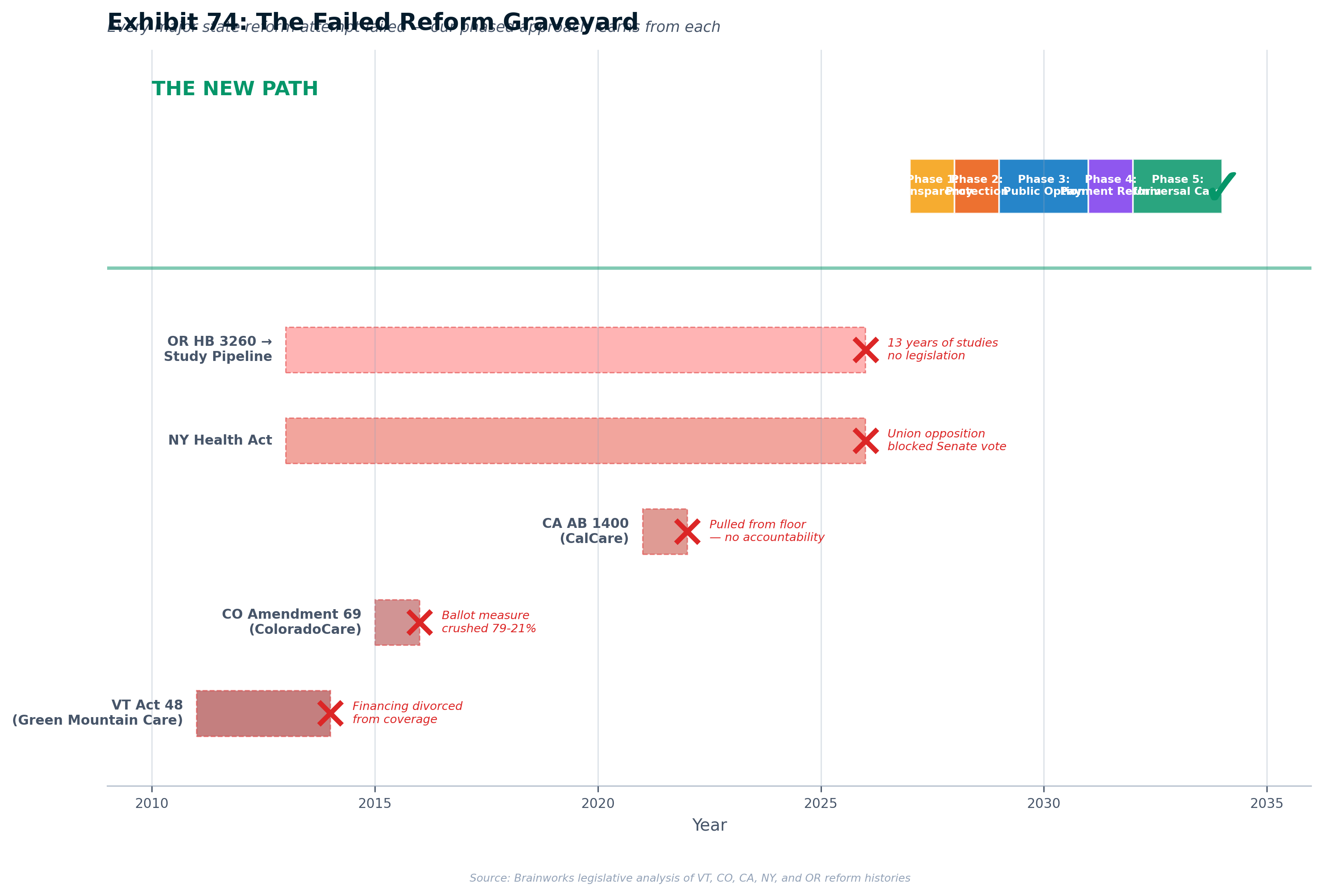
The historical record of state-level healthcare reform is unambiguous on one point: no state has ever succeeded by jumping directly to universal coverage in a single legislative act. Vermont passed single-payer and collapsed on financing. California introduced single-payer three times and couldn't secure a floor vote. Colorado put single-payer on the ballot and lost 79–21. New York has had majority cosponsors for single-payer for years and cannot get a Senate vote. Oregon has studied single-payer for thirteen years without producing legislation. [1]
The one state that succeeded — Massachusetts, in 2006 — did so through a phased approach that built the broadest possible coalition, integrated financing with coverage, and created political constituencies at each stage that made subsequent stages both more feasible and more politically defensible. [2]
This chapter presents the five-phase legislative strategy designed to apply the lessons of every major reform attempt — successful and failed — to the specific conditions of 2026–2038. The strategy is built on a fundamental insight drawn from the analysis in Volumes I and II: the goal is not simply to expand coverage, but to eliminate the waste, inefficiency, and misaligned incentives that divert $1.8 trillion annually from patient care.
Why Phased Legislation Succeeds Where Big-Bang Reform Fails
Single-payer proposals fail for structural reasons, not incidental ones. They present the full cost upfront without context, triggering sticker shock. They threaten every incumbent interest simultaneously — insurers, employers, unions, providers — creating a unified opposition coalition. They require federal waivers that may be politically impossible under hostile administrations. They demand a leap of faith from voters and legislators who cannot verify that the promised savings will materialize. And they provide no off-ramp if implementation encounters problems. [3]
The phased approach solves each of these problems. Each phase is independently valuable, politically achievable, and builds the infrastructure and constituency for the next. If the campaign stalls at Phase 3, the state still has price transparency, rate regulation, and a competitive public option — meaningful improvements benefiting millions. There is no "all or nothing" risk.
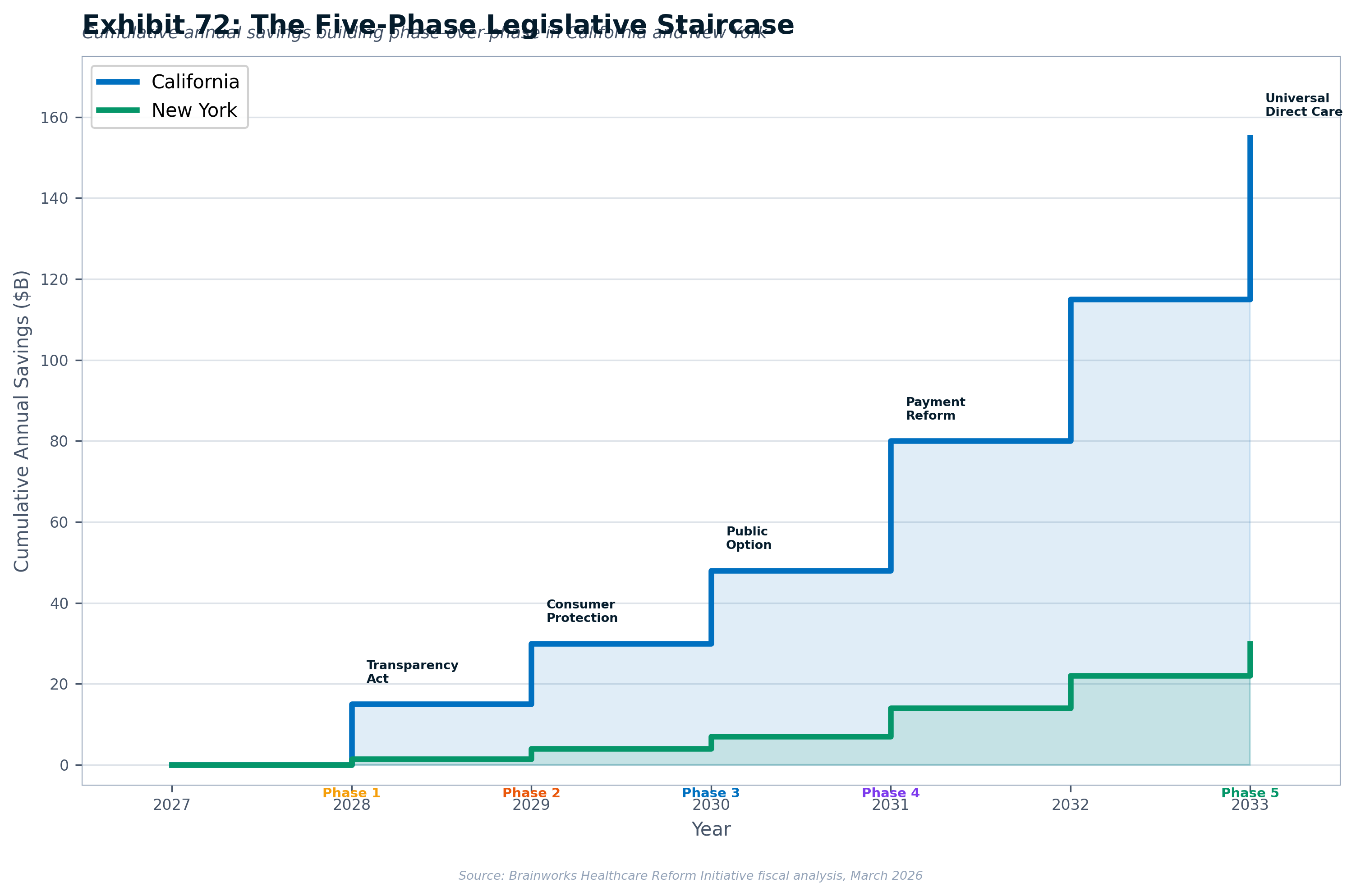
The Five Phases Explained
Phase 1: Transparency & Accountability (Year 1–2)
Mandates comprehensive healthcare price and financial transparency. Creates an all-payer claims database (APCD) and expands the state's health cost oversight authority. Publishes an annual "Healthcare Efficiency Index" showing what percentage of each healthcare entity's revenue reaches patient care versus administrative overhead. Builds the IT infrastructure for subsequent phases. No federal waivers required. Financing: modest assessment on health insurers (0.15% of premium revenue). Political feasibility: very high — opposing transparency is politically toxic across the entire political spectrum. [4]
Phase 2: Consumer Protection & Preventing Monopoly Abuse (Year 2–3)
Addresses the most visible system failures: prior authorization denials (80.7% appeal overturn rate proves systematic inappropriate denials), PBM manipulation (insulin prices inflated 1,200% through rebate walls), and insurance profiteering (raising MLR requirement to 90%). Implements all-payer rate setting for hospital services — Maryland has operated this model successfully since 1977 with documented cost savings. This is not government price-fixing; it is preventing monopoly pricing abuse in markets where consumers have no real choice. No federal waivers required. [5]
Phase 3: Introducing Real Competition (Year 3–5)
Creates a state-administered health plan available to all residents and employers — a public option that introduces genuine competition into insurance markets dominated by monopolies or near-monopolies. Provider reimbursement capped at 150% of Medicare (aggregate). Administrative cost target: under 5%, declining to 3%. Mandates hospital participation. Targets premiums 15–25% below comparable commercial plans. Launches Direct Primary Care (DPC) integration pilot. Minimal federal waivers required — plan operates as a Qualified Health Plan within the existing ACA framework. [6]
Phase 4: Payment Reform & System Modernization (Year 5–7 Optimistic / Year 7–10 Base Case)
Extends all-payer rate setting statewide to all services. Implements global hospital budgets (Maryland/Taiwan model). Integrates DPC as the primary care foundation. Mandates single claim form, single credentialing process, and 14-day clean claim payment — streamlining the administrative burden that consumes 34 cents of every healthcare dollar. Administrative cost reduction target: 50% within five years. Section 1115 Medicaid waiver required for Medicaid integration; Medicare integration requires additional federal authority. [7]
Phase 5: Universal Direct Care (Year 7–10 Optimistic / Year 10–15 Base Case)
Full universal enrollment — eliminating the free-rider problem that shifts costs from the uninsured to everyone else. Eliminates insurance intermediation for routine care (80% of claims). Maintains streamlined insurance function only for high-cost, unpredictable events. Administrative overhead target: 3%, consistent with Taiwan's NHI and Canadian provincial systems. Progressive payroll assessment replaces employer premiums. Comprehensive federal waivers required (Sections 1332, 1115, and Medicare). Five-year workforce transition program for displaced administrative workers. [8]
Dual Timeline: Optimistic vs. Base Case
Planning Timelines — Two Scenarios
| Phase | Optimistic (6–8 years) | Base Case (10–12 years) |
|---|---|---|
| Phase 1: Transparency | 2027 | 2027–2028 |
| Phase 2: Consumer Protection | 2028 | 2029–2030 |
| Phase 3: Real Competition | 2029 | 2030–2032 |
| Phase 4: Payment Reform | 2030–2031 | 2033–2035 |
| Phase 5: Universal Direct Care | 2032–2034 | 2036–2038 |
Recommendation: Use the base case (10–12 years) for planning, budgeting, and funder communications. The optimistic timeline is achievable only with cooperative federal conditions, a committed governor, and no major setbacks. Campaign materials should present both timelines with the base case as the default.
How Each Phase Builds the Political Foundation for the Next
The genius of the phased approach is its self-reinforcing political logic:
- Phase 1 creates data that demands Phase 2 — when voters see that the same MRI costs $500 from one insurer and $3,000 from another at the same facility, they demand rate regulation
- Phase 2 creates savings that fund Phase 3 — lower healthcare costs make the public option affordable and reduce employer resistance
- Phase 3 creates a constituency that demands Phase 4 — millions enrolled in the public option become its political defenders, just as Medicare recipients defend Medicare
- Phase 4 demonstrates administrative savings that justify Phase 5 — the streamlined system is visibly more efficient, and the "net savings" argument is proven in practice, not theory
- Phase 5 creates a permanent constituency — like Medicare, politically untouchable once implemented
The "Vermont Trap" and How to Avoid It
Vermont's Green Mountain Care (Act 48, 2011) is the most instructive failure in American healthcare reform history. Governor Shumlin signed single-payer into law — and then abandoned it in December 2014 when the financing plan arrived as sticker shock: an 11.5% payroll tax and progressive income tax up to 9.5%. The campaign had never established the "net cost" narrative. Voters heard "11.5% payroll tax" without hearing "but you'll no longer pay $15,000/year in premiums." [9]
The Vermont Lesson — An Absolute Rule
Never pass a coverage bill without a financing bill. They must move together or the financing will never survive on its own. Every phase in this strategy includes its own financing mechanism specified in the enabling legislation.
The phased approach avoids the Vermont Trap structurally. Each phase has its own financing mechanism. The financing scales with the scope — Phase 1 costs almost nothing, Phase 2 saves money, Phase 3 is self-financing through premiums, Phase 4 captures administrative savings, and Phase 5 redirects existing spending. At no point does the state face a single massive financing bill. [10]
Chapter 18: California — Leading the Transformation
California is at an inflection point for healthcare reform. The convergence of three forces — federal Medicaid cuts threatening up to 3.4 million Californians at risk of losing coverage under H.R. 1, the expiration of ACA enhanced premium subsidies (producing a 32% drop in new Covered California enrollments), and a wide-open 2026 gubernatorial race where nearly every Democratic candidate champions reform — creates an unprecedented window for transformational legislation. [11]
The Political Landscape and Opportunity Window
Democrats hold supermajorities in both chambers (approximately 62/80 Assembly seats, 32/40 Senate seats), providing the two-thirds majority needed for urgency statutes, tax increases, and constitutional amendments. Gavin Newsom is termed out. The next governor — almost certainly a Democrat — will have campaigned on healthcare transformation. [12]
Polling confirms the mandate: 86% of California Democrats support single-payer; nearly two-thirds of all California voters want transformational — not incremental — health reform. [13]
The Office of Health Care Affordability (OHCA), established in 2022, provides existing regulatory infrastructure. OHCA has set 3% healthcare cost growth spending targets, conducted its first Cost and Market Impact Review, and seen its authority expanded by AB 1415 and SB 351 (both signed by Newsom in 2025). This is the institutional foundation upon which Phase 1 builds. [14]
The Five California Bills
| Phase | Bill | Target Year | Core Mechanism | Federal Waiver |
|---|---|---|---|---|
| Phase 1 | CA Healthcare Transparency & Accountability Act | 2027 | Price transparency, APCD, OHCA expansion, Efficiency Index | None |
| Phase 2 | CA Healthcare Consumer Protection Act | 2028–2029 | Prior auth reform, PBM regulation, MLR increase to 90%, anti-consolidation | None |
| Phase 3 | CA Healthcare Competition Act | 2029–2031 | State-administered health plan, 150% Medicare rates, DPC pilot | Minimal |
| Phase 4 | CA Healthcare Payment Reform Act | 2031–2034 | Statewide all-payer rate setting, global hospital budgets, admin simplification | Section 1115 |
| Phase 5 | CA Universal Direct Care Act | 2033–2037 | Universal enrollment, 3% admin target, elimination of waste intermediaries | Comprehensive |
Revised Savings Projections
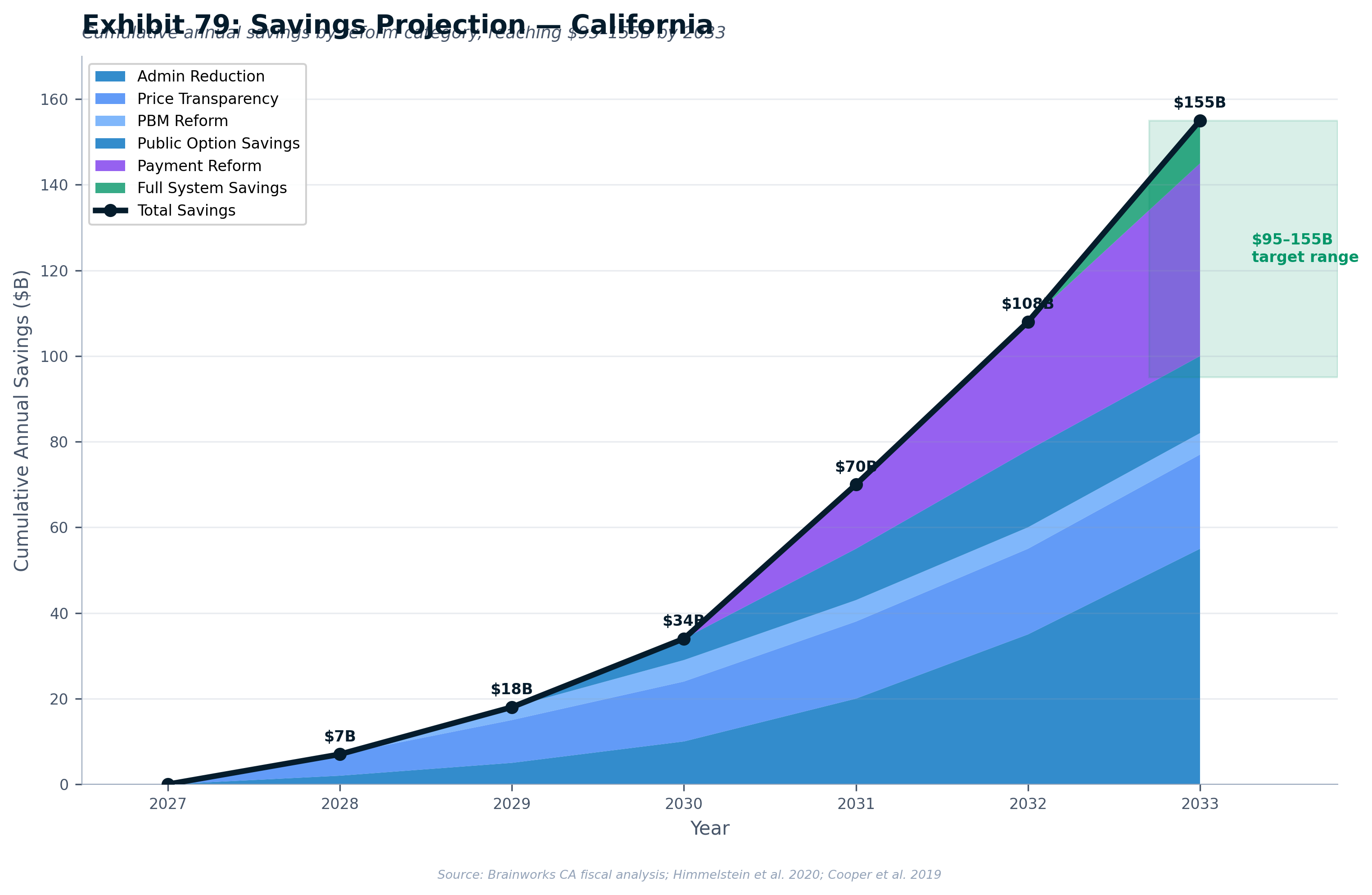
| Savings Category (Phase 5) | Low Estimate | Mid Estimate | High Estimate | Type |
|---|---|---|---|---|
| Administrative simplification | $15B | $22B | $30B | Avoided cost growth |
| Negotiated drug prices | $5B | $8B | $12B | Absolute reduction |
| Insurance overhead elimination | $8B | $10B | $12B | Absolute reduction |
| Provider billing simplification | $5B | $7B | $10B | Avoided cost growth |
| Uncompensated care elimination | $3B | $4B | $5B | Absolute reduction |
| Population health improvement | $2B | $3B | $5B | Avoided cost growth (5–10 year lag) |
| Total Phase 5 Annual | $30B | $45B | $60B | Mixed |
Chapter 19: New York — Breaking the Senate Deadlock
The New York Health Act is the most paradoxical case in American healthcare reform: a bill with majority cosponsorship in both chambers that has never received a Senate floor vote. First introduced in 1991 by Assemblyman Richard Gottfried, it has passed the Assembly at least four times (2015–2018). [19]
The Public-Sector Union Problem — and How to Solve It
The silent obstacle to the NY Health Act is public-sector union concern. CSEA, DC 37 (AFSCME), and the UFT have expressed concern that universal healthcare could reduce the value of employer-provided health insurance — their primary recruitment and retention tool. Union-negotiated health benefits are the centerpiece of collective bargaining. [20]
The solution has four components, codified in the Phase 2 bill's Title IV — the "Workers' Shield":
Title IV: The Workers' Shield — Four Components
1. Benefit Guarantee Plus Enhancement: Statutory language guaranteeing that no public employee receives benefits inferior to their current plan. Plus immediate enhancements: elimination of all copays for preventive care, dental/vision upgrades, prescription caps.
2. Governance Roles: No fewer than 3 seats on any governing board reserved for public-sector union designees. Unions become builders of the new system, not defenders of the old one.
3. Wage Bargaining Enhancement: Upon implementation, the value of healthcare benefits previously bargained converts to equivalent wage increases.
4. Workforce Transition Authority: Five-year employment guarantee for displaced workers, retraining programs, priority hiring in the new system, pension credit continuity. [22]
The H.R. 1 Crisis as Catalyst
The federal healthcare assault creates a unique window. H.R. 1 cut $7.5 billion in federal health funding to New York, placing approximately 450,000 New Yorkers at risk of losing Essential Plan coverage. The narrative writes itself: "If the federal government won't protect New York's healthcare, New York must protect itself." [23]
The Five New York Bills
| Phase | Bill | Target Year | Core Mechanism |
|---|---|---|---|
| Phase 1 | NY Healthcare Transparency Act | 2027 | Healthcare Efficiency Dashboard, hospital/insurer/PBM disclosure |
| Phase 2 | NY Healthcare Consumer & Worker Protection Act | 2027–2028 | Prior auth reform, PBM regulation, Title IV union provisions |
| Phase 3 | NY Public Health Option Act ("NY HealthChoice") | 2028–2030 | State public option, Essential Plan expansion, DPC pilot |
| Phase 4 | NY Healthcare Payment Reform Act | 2029–2033 | Statewide all-payer rate setting, global budgets, admin simplification |
| Phase 5 | NY Universal Direct Care Act | 2030–2036 | Universal enrollment, single admin system, 5% admin target |
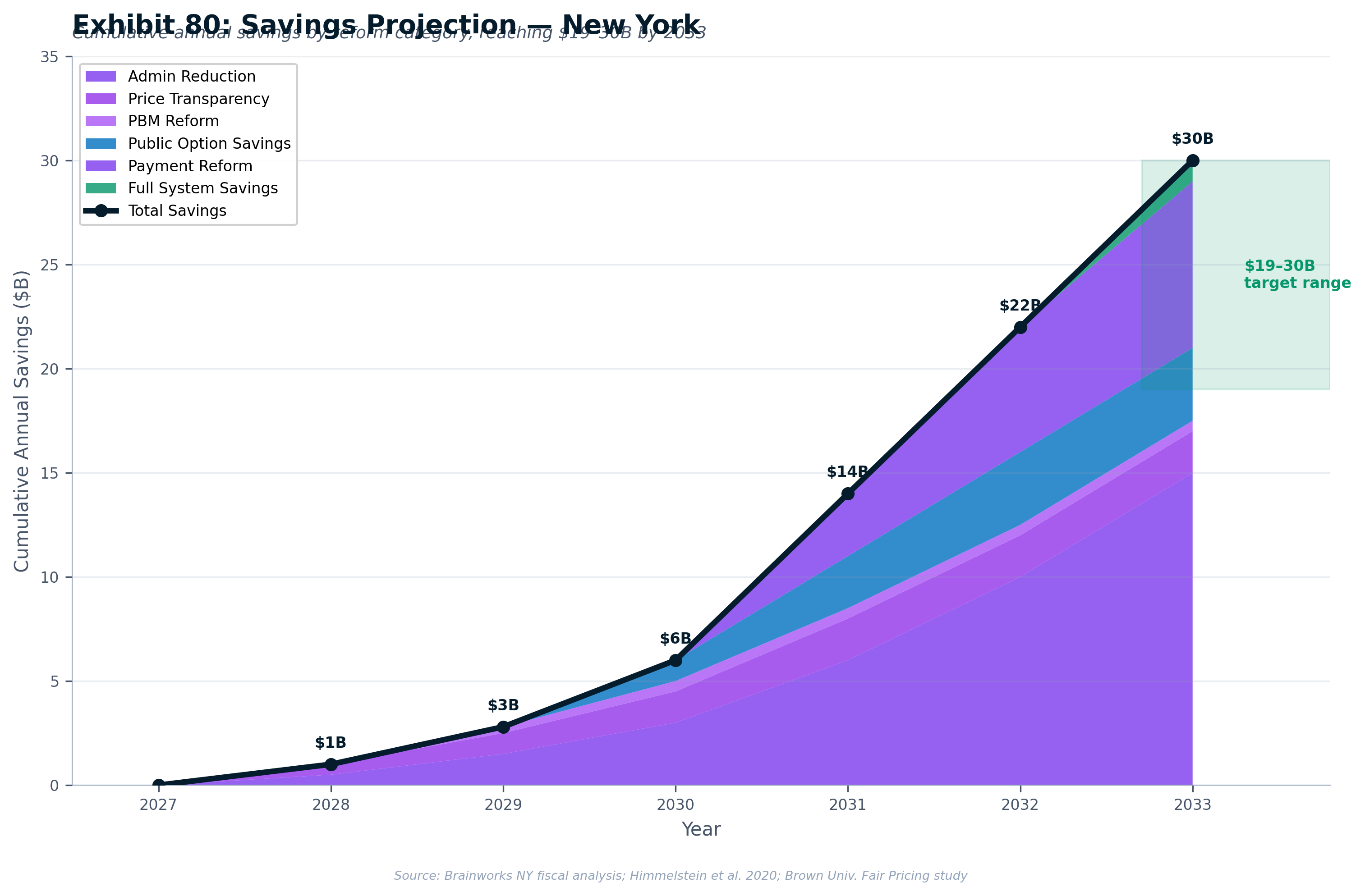
Revised Savings Projections — New York
| Savings Category (Phase 5) | Low | Mid | High | Type |
|---|---|---|---|---|
| Administrative savings | $5B | $7B | $10B | Avoided cost growth |
| Rate rationalization | $3B | $4B | $5B | Avoided cost growth |
| DPC-driven prevention | $1B | $2B | $3B | Avoided cost growth (lagged) |
| Pharmaceutical purchasing | $1B | $1.5B | $2B | Absolute reduction |
| Total Phase 5 Annual | $10B | $15B | $20B | Mixed |
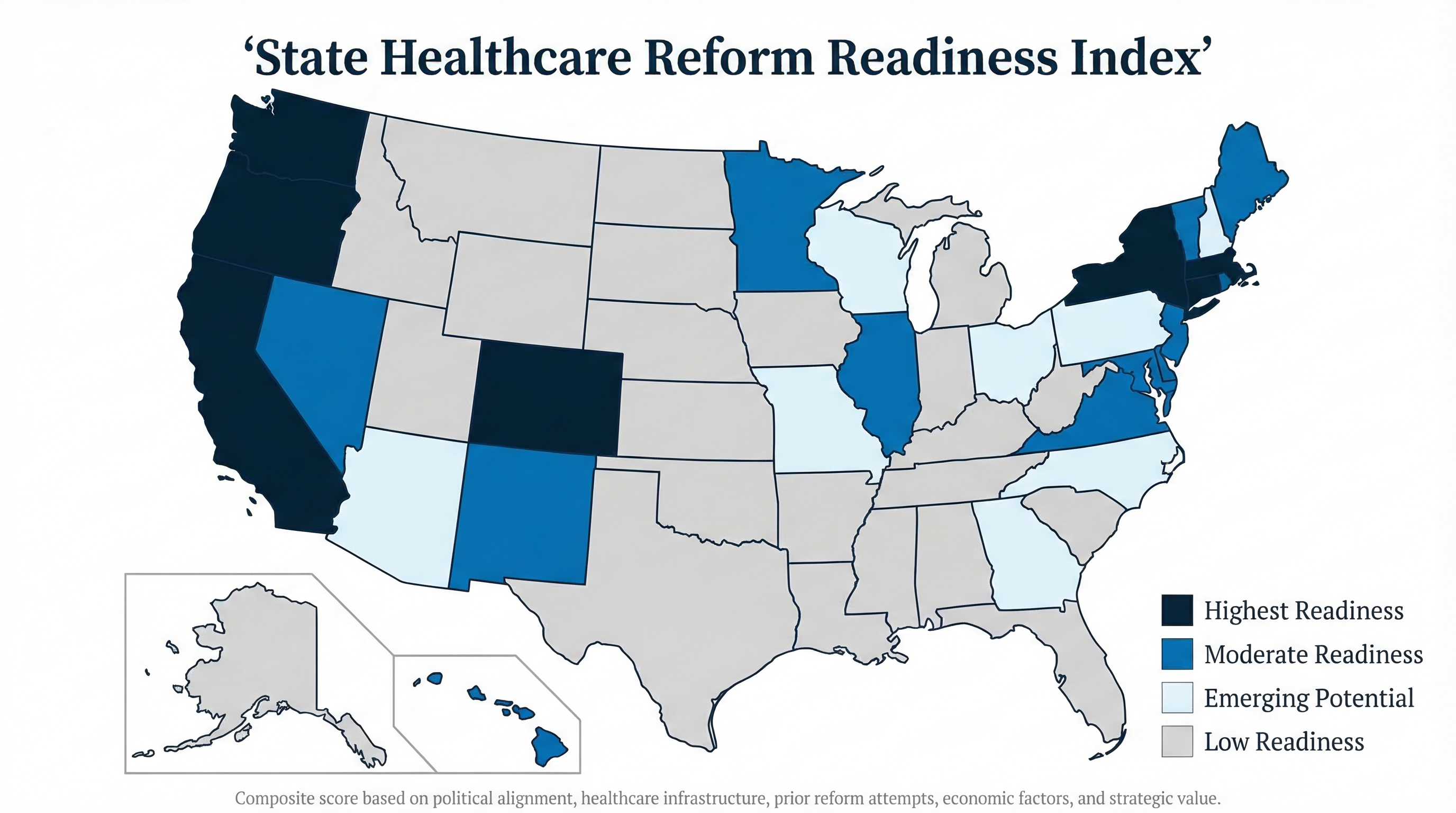
Chapter 20: The National Map — Ten Reform-Ready States
California and New York are the flagships — but a strategy that works only in deep-blue states is not a national strategy. Healthcare costs burden every American employer, every American worker, and every American community — regardless of political affiliation. This chapter profiles the ten most reform-ready states across the political spectrum, demonstrating that healthcare reform can be advanced in red, blue, and purple states with the right framing and coalition approach. [26]
1. Massachusetts — The Gold Standard (Reform Likelihood: 80%)
Proposed Bill: "Massachusetts Healthcare & AI Opportunity Act"
Why now: Governor Maura Healey has made healthcare a priority issue, launching an AI Hub initiative and deploying a ChatGPT-powered assistant to 40,000 state workers. The state's Chapter 58 (2006) legacy — the model for the ACA — creates path-dependent institutional support. Democratic supermajority in both chambers. Sweeping healthcare market oversight bill signed in 2025.
Framing: "Building on Chapter 58 — extending Massachusetts healthcare leadership into the AI age." This state responds to evidence-based, innovation-forward messaging that combines healthcare universality with economic competitiveness.
Coalition: Massachusetts AFL-CIO, SEIU Local 509, Massachusetts Nurses Association, Healey administration, Harvard/MIT academic network, biotech industry (workforce stability).
AI-personalized approach: Massachusetts values institutional credibility and evidence. Messaging emphasizes data, research backing, and builds on the state's identity as a healthcare policy innovator. Power words: "leadership," "evidence-based," "innovation," "responsibility."
2. Washington — The Public Option Pioneer (Reform Likelihood: 75%)
Proposed Bill: "Washington AI Transition & Healthcare Security Act"
Why now: Cascade Care public option fully implemented statewide in 2025 — the most advanced public option in America. New Governor Bob Ferguson has healthcare as a priority issue. Democratic supermajority. Strong labor union infrastructure (SEIU, Amazon worker organizing).
Framing: "Extending Cascade Care's success to protect workers in the AI age." Washington responds to progressive-pragmatic framing that links healthcare security to economic transition.
Coalition: Washington State Labor Council, SEIU Local 775, nurses unions, tech worker organizing groups, Ferguson administration.
AI-personalized approach: Heavy tech sector presence (Amazon, Microsoft) makes AI displacement visceral and personal. Frame healthcare continuity as the bridge that makes AI transition manageable. Power words: "security," "transition," "community," "leadership."
3. California — The Scale Leader (Reform Likelihood: 75%)
Proposed Bill: "California AI Opportunity Act"
Why now: Democratic supermajority, 2026 open gubernatorial race, existing OHCA infrastructure, AB 1900 (CalCare) with 20 co-authors and 270+ organizational endorsements. Federal H.R. 1 threatening 3.4 million Californians.
Framing: "Healthcare justice and efficiency — California leads." The state responds to equity + innovation framing that combines social justice language with pragmatic economic arguments.
Coalition: CNA/NNU (100,000+ nurses), Health Access California, SEIU California State Council, PNHP California, California Pan-Ethnic Health Network, small business allies.
AI-personalized approach: Largest tech sector in the nation means AI displacement is already happening. Frame healthcare reform as enabling responsible AI transition. Power words: "equity," "innovation," "accountability," "opportunity."
4. Colorado — The Innovation Lab (Reform Likelihood: 70%)
Proposed Bill: "Colorado Responsible AI Transition Act"
Why now: Governor Polis (tech entrepreneur) signed the nation's most comprehensive AI regulation (SB 24-205) in 2024. Colorado Option public option saving $493M+ in premiums. SB25-045 mandated healthcare study, report due December 2026. Democratic supermajority.
Framing: "Responsible innovation — protecting workers while leading in AI." Colorado responds to pragmatic, innovation-forward framing that positions regulation as enabling sustainable growth.
Coalition: Colorado AFL-CIO, SEIU Colorado, Colorado Nurses Association, Polis administration, tech companies (Google, Microsoft), Colorado Healthcare Institute.
AI-personalized approach: Polis's tech background means AI framing resonates. Build on SB 205 success — position worker protection as completing the AI regulation framework. Power words: "responsible," "innovation," "sustainable," "Colorado-led."
5. New York — Breaking the Deadlock (Reform Likelihood: 55%)
Proposed Bill: "New York Fair AI Transition Act"
Why now: NY Health Act has 39+ Senate sponsors and 90+ Assembly sponsors. H.R. 1 cut $7.5 billion in federal health funding. Workers' Shield strategy addresses union opposition. Democratic trifecta (though narrower than CA/WA).
Framing: "Healthcare is a human right — and workers in the AI age deserve security." New York responds to rights-based language coupled with economic security arguments.
Coalition: Campaign for New York Health, 1199 SEIU (400K members), NY State Nurses Association, progressive legislators, community organizations.
AI-personalized approach: Financial services concentration (Manhattan) makes AI displacement a Wall Street story as well as a Main Street story. Frame transition support as preventing social instability. Power words: "security," "rights," "fairness," "New York values."
6. Oregon — The Governance Pioneer (Reform Likelihood: 65%)
Proposed Bill: "Oregon Healthcare Modernization Act"
Why now: Oregon's Universal Health Care Governance Board is delivering its plan in September 2026 — the most advanced structural preparation in the nation. Score: 91 on reform readiness index. Democratic trifecta.
Framing: "Completing Oregon's healthcare promise." Oregon responds to communitarian, sustainability-focused framing that emphasizes community health and practical solutions.
Coalition: CNA/NNU Oregon chapter, Oregon Health Equity Alliance, rural health advocates, environmental justice organizations.
AI-personalized approach: Smaller tech scene but Portland startup culture means innovation resonates. Rural healthcare crisis in eastern Oregon creates bipartisan opening. Power words: "community," "sustainability," "practical," "Oregon values."
7. Ohio — The Pragmatic Heartland (Reform Likelihood: 55%)
Proposed Bill: "Save Our Hospitals Act" / "Ohio Workforce Resilience Act"
Why now: Governor DeWine is a pragmatic conservative who expanded Medicaid under Kasich's framework and maintains it. 31 Ohio hospitals have closed or significantly reduced services. Strong labor union tradition (UAW, USW). Post-industrial workforce concerns create unique political space.
Framing: "Saving our hospitals, protecting our workers — Ohio common sense." Ohio responds to communitarian, populist framing that emphasizes tangible local impacts — jobs, hospitals, community survival. Avoid: "disruption," "transformation," "innovation economy," "coastal."
Coalition: Ohio Hospital Association, UAW, AFSCME, community hospital administrators, Ohio Farm Bureau, rural municipal governments, faith communities (rural church networks), small-town mayors.
AI-personalized approach: Ohio's manufacturing heritage means framing AI transition as the next industrial adaptation — "Ohio workers have adapted before, from steam to electricity to digital. They'll adapt to AI too, but they need support." Emphasize concrete, local impacts over abstract policy. Power words: "community," "our hospitals," "Ohio workers," "practical," "common sense."
8. Arizona — The Choice State (Reform Likelihood: 50%)
Proposed Bill: "Arizona Healthcare Choice Act" / "Arizona Healthcare & Workforce Opportunity Act"
Why now: Split government (Governor Hobbs D, Republican legislature) creates negotiation dynamic. Medicaid expansion via Proposition 204 (2014) remains popular (65%+ approval). H.R. 1 federal cuts threaten 500K+ Arizonans. Growing tech sector (Apple, Intel, TSMC). Large retiree population with intense healthcare interests. Tribal nation sovereignty concerns create unique coalition opportunities.
Framing: "Real choice in healthcare — breaking insurance monopolies, not expanding government." Arizona responds to liberty-focused, anti-monopoly framing. The argument is that Arizonans don't have real healthcare choice today — one insurance company often controls an entire county. Avoid: "mandate," "federal," "California model," "regulation."
Coalition: Arizona Hospital Association, Arizona Chamber of Commerce, tribal nations, retiree communities (Sun City, Green Valley), Arizona Farm Bureau, small business associations, Latino business associations, ASU/U of A (AI research).
AI-personalized approach: Semiconductor investments (Intel, TSMC) make AI/automation workforce concerns tangible. Frame transition support as Arizona preparing for its economic future. "Arizona is ready — let's make sure Arizonans are ready too." Power words: "choice," "freedom," "independence," "Arizona solutions," "competition."
9. Georgia — The New South Rising (Reform Likelihood: 45%)
Proposed Bill: "Georgia Healthcare Freedom Act" / "Peach State Innovation Act"
Why now: Unprecedented bipartisan opening — four Republican legislators signed onto a Medicaid expansion bill in January 2025. Rural hospital crisis acute: 60% of Georgia's rural hospitals on brink of failure. Governor Kemp is pragmatic (pursuing "Georgia Pathways" waiver alternative). Atlanta's tech ecosystem growing rapidly. HBCUs (Morehouse, Spelman, Clark Atlanta) provide coalition anchor.
Framing: "Georgia-grown solutions for Georgia families — not waiting for Washington." Georgia responds to business-friendly, innovation-forward framing that bridges the state's diverse constituencies — economic freedom (business community), personal freedom (suburban moderates), and freedom from discrimination (Black communities). Avoid: "liberal," "mandate," "redistribution," "Northern model."
Coalition: Metro Atlanta Chamber of Commerce, Georgia Hospital Association, HBCUs, faith communities (Black churches in Atlanta + rural white churches in South Georgia), Georgia Farm Bureau, Georgia Tech, the four Republican expansion bill co-sponsors, Georgia Retail Association.
AI-personalized approach: Atlanta's emergence as a tech hub (Google, Microsoft, Amazon) creates AI workforce concerns. Frame workforce development as ensuring AI benefits reach all Georgians — "from Atlanta to Albany, from Savannah to Dalton." Link to HBCU workforce training. Power words: "Georgia-grown," "business-friendly," "freedom," "opportunity," "New South."
10. Texas — The Long Game (Reform Likelihood: 20–35%)
Proposed Bill: "Free Market Healthcare Competition Act" / "Texas Rural Healthcare Security Program"
Why now: Texas has the highest uninsured rate in the nation (16.7%, ~2.5 million Texans) and 450,000 uninsured children. 14+ hospital closures since 2015 with 60+ vulnerable facilities. A 24-member bipartisan group proposed Medicaid expansion in May 2025 (shot down by leadership). Texas Hospital Association and rural providers increasingly vocal. Healthcare costs add a massive burden to the state's $1.5 trillion economy.
Framing: "Free market competition — breaking the healthcare monopolies that are shutting down Texas hospitals and driving up costs for Texas businesses." Texas political culture demands maximum liberty and market language. The argument: the current system is not a free market — it's dominated by out-of-state corporate monopolies. Reform restores real competition. Avoid: "regulation," "government program," "mandate," "universal," "European model."
Coalition: Texas Hospital Association, Texas Farm Bureau, NFIB Texas chapter, rural hospital administrators, faith communities, veterans' organizations, Texas Medical Association (physician autonomy from insurance bureaucracy).
AI-personalized approach: Texas's exploding tech sector (Austin, Dallas, Houston, San Antonio) creates AI workforce concerns, but frame through market lens: "Texas should lead the AI revolution — Texas workers deserve the training to stay competitive." Emphasize employer-led transition with state incentives, not mandates. Power words: "freedom," "choice," "competition," "Texas-led," "protecting Texans," "local control."
The long game: Texas is unlikely to pass comprehensive reform under current leadership. But the rural hospital crisis is accelerating, business community pressure is rising, and the post-Abbott era (2027 election) may create new openings. Every rural hospital closure makes the case for reform stronger.
Reform-Ready States: Summary Rankings
| Rank | State | Political Control | Likelihood | Key Advantage |
|---|---|---|---|---|
| 1 | Massachusetts | Dem Supermajority | 80% | Chapter 58 legacy + Healey leadership + AI Hub |
| 2 | Washington | Dem Supermajority | 75% | Cascade Care public option operational |
| 3 | California | Dem Supermajority | 75% | Scale + OHCA infrastructure + gubernatorial race |
| 4 | Colorado | Dem Supermajority | 70% | AI Act precedent + Colorado Option success |
| 5 | Oregon | Dem Trifecta | 65% | Governance Board plan Sep 2026 |
| 6 | New York | Dem Trifecta | 55% | 90+ Assembly sponsors + H.R. 1 crisis catalyst |
| 7 | Ohio | GOP Supermajority | 55% | DeWine pragmatism + rural hospital crisis |
| 8 | Arizona | Split | 50% | Popular Medicaid expansion + bipartisan openings |
| 9 | Georgia | GOP Supermajority | 45% | Bipartisan expansion bill + rural crisis |
| 10 | Texas | GOP Supermajority | 20–35% | Rural crisis + business pressure + long game |
Chapter 21: Lessons from the Battlefield — Why Reform Fails and How to Win
Five major state-level single-payer reform efforts have failed in the United States. One — Massachusetts Chapter 58 — succeeded spectacularly. And internationally, several conservative, market-based models have achieved universal or near-universal coverage. Each offers distinct, actionable lessons. [32]
Massachusetts Chapter 58: The Gold Standard
On April 12, 2006, Republican Governor Mitt Romney signed the most ambitious state-level healthcare reform in American history. Within four years, the uninsured population dropped from approximately 602,000 to 356,000 — during the Great Recession. A 2011 poll found three-to-one public approval five years after passage. Massachusetts succeeded through the impossible coalition (Heritage Foundation + Ted Kennedy), the ballot initiative as a weapon, revenue neutrality, and phased implementation. [33]
The Graveyard: Vermont, CalCare, ColoradoCare, Oregon
Conservative and Market-Based Reform Models That Work
Healthcare reform need not follow a single ideological template. Several of the most successful models globally and domestically have been championed by conservative policymakers and institutions:
Indiana's Healthy Indiana Plan (HIP 2.0) — The HSA-Based Approach
Championed by then-Governor Mike Pence, HIP 2.0 covers adults up to 138% of the Federal Poverty Level through POWER Accounts — health savings account-style structures requiring monthly contributions of $1–$27 based on income. The plan features two tiers: HIP Plus (for those making contributions, with enhanced benefits including dental and vision) and HIP Basic (reduced benefits with copayments). HIP demonstrates that conservative principles — personal responsibility, consumer choice, market mechanisms — can be integrated into public health coverage. A deeply red state expanded coverage to hundreds of thousands using conservative mechanisms.
Utah's Intermountain Health — Value-Based Care
Intermountain Health, operating 33 hospitals and 385+ clinics, pioneered value-based care — rewarding providers for health outcomes rather than service volume. Telehealth patients achieved similar clinical outcomes at costs of $1,016 vs. $1,556–$1,896 for controls. The model is market-driven, not government-imposed — and demonstrates that competition on quality and outcomes naturally reduces costs. If the entire U.S. system achieved Intermountain-level efficiency, employer costs could fall 20–30%.
Singapore's MediSave/MediShield — HSA + Catastrophic
Singapore achieves universal coverage through three pillars: MediSave (mandatory individual healthcare savings accounts funded through payroll deductions), MediShield Life (universal catastrophic insurance), and MediFund (safety net for low-income citizens). Singapore spends just 4.1% of GDP on healthcare while achieving life expectancy of 84.1 years (vs. 77.5 in the U.S.) and zero medical bankruptcies. The Heritage Foundation, AEI, and other conservative institutions have repeatedly cited Singapore as a model. The key insight: separate routine care (individual savings) from catastrophic protection (universal insurance).
Switzerland — Private Mandate with Regulated Competition
Switzerland achieves >99.5% coverage through private, not-for-profit insurance companies operating under a government mandate with regulated competition. Every resident must purchase basic health insurance. Insurers compete on premiums but must accept all applicants. Healthcare spending cannot exceed 8% of an individual's income. The model was originally inspired by Alain Enthoven's "managed competition" — the same concept that influenced the Heritage Foundation's original 1989 healthcare proposals. No government-run insurance; instead, genuine market competition within a regulatory framework.
Maryland's All-Payer Rate Setting — 47 Years of Proven Results
Maryland has operated all-payer hospital rate setting since 1977 — the longest-running experiment in regulated healthcare pricing in America. Under this system, all payers (Medicare, Medicaid, commercial insurers) pay the same rate for the same service at the same hospital. The result: Maryland's hospital cost growth has been consistently below the national average, rural hospitals have remained open, and the system has survived under governors of both parties for nearly half a century. If rate setting were a radical idea, it would not have survived 47 years in a politically competitive state.
The 10 Rules for Successful State Healthcare Reform
The 10 Rules — Synthesized from Every Success and Failure
- Never separate coverage from financing. They must pass together. Vermont is the proof.
- Win the framing war before the legislative battle. Establish the "total cost" narrative months or years before the bill is introduced.
- Build the broadest possible coalition. Nurses + progressive activists is necessary but not sufficient. You need business allies, provider organizations, faith communities, fiscal conservatives, and rural advocates.
- Phase the approach. No state has succeeded by jumping to universal coverage in one leap.
- Use the ballot initiative as a weapon, not the vehicle. Collect signatures to create the legislative deadline, but pursue reform through the legislative process.
- Force the vote. Never pull a bill. Even a losing recorded vote creates accountability.
- Lock in the governor. Executive commitment must be secured before the campaign invests.
- Solve the union problem proactively. Address public-sector union concerns from day one.
- Build cost containment into the original design. Massachusetts's biggest failure was the six-year gap before cost controls.
- Plan for the morning after. The coalition that passes the bill must survive to defend implementation. [35]
The Opposition Playbook — and How to Counter It
Chapter 22: Building the Movement — A Bipartisan Coalition
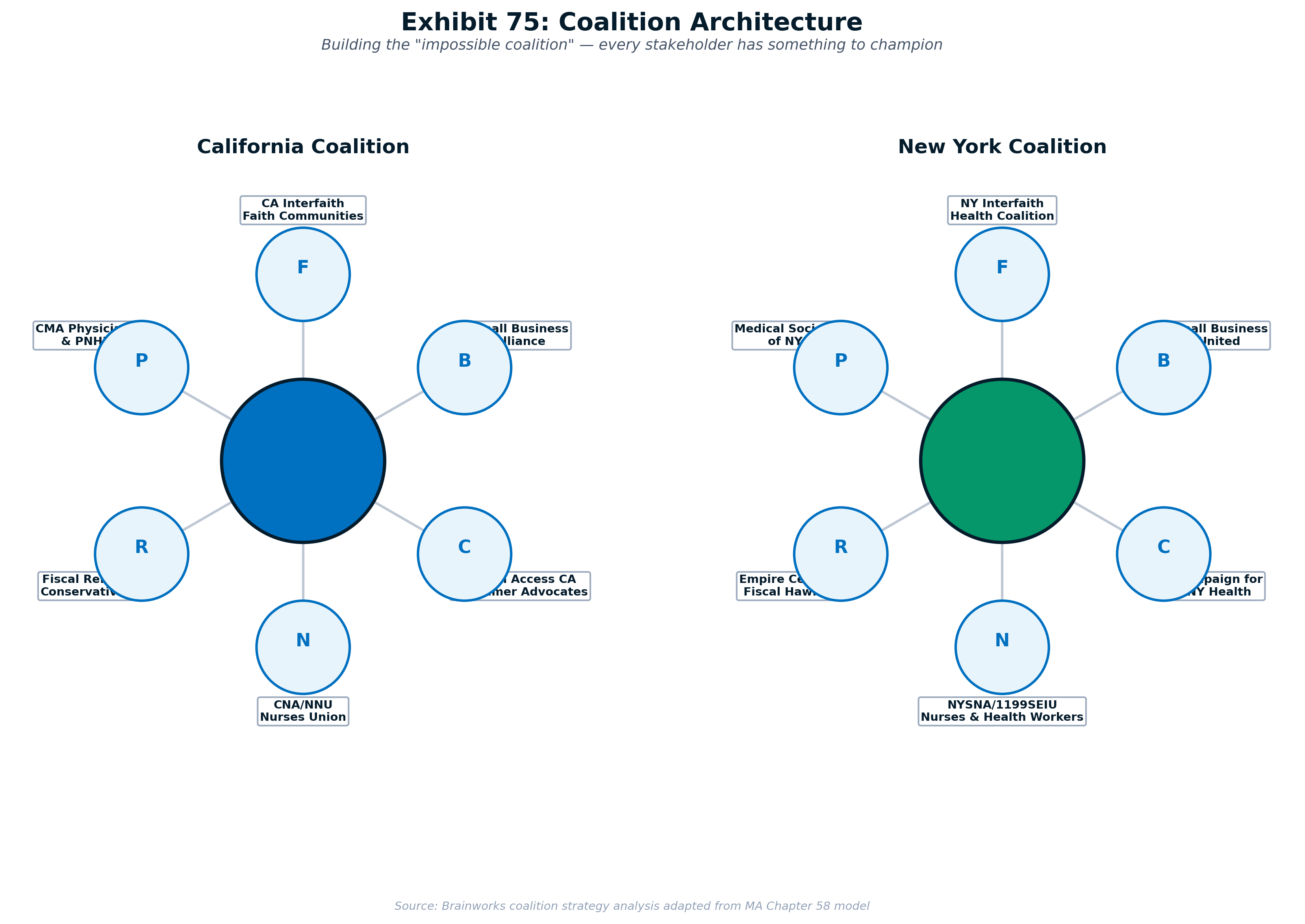
Massachusetts Chapter 58 succeeded because an extraordinary coalition — spanning Heritage Foundation intellectual origins to Ted Kennedy's progressive vision — invested in rigorous research, strategic advocacy, and relentless organizing. This chapter builds a coalition architecture that is explicitly bipartisan, reflecting the reality that healthcare costs burden Americans regardless of political affiliation. [37]
Coalition Architecture and Governance
The Bipartisan Coalition: Seven Pillars
Pillar 1: Progressive Healthcare Advocates
California Nurses Association/NNU, Health Access California, SEIU, PNHP, Campaign for New York Health, state-level single-payer advocacy organizations. These are the movement's core — the organizations that have been fighting for reform for decades.
Pillar 2: Business Community
National Federation of Independent Business (NFIB) — representing small businesses whose #1 complaint is healthcare costs. Local and state chambers of commerce — increasingly vocal about healthcare as a competitive burden. National Association of Manufacturers (NAM) — manufacturers bear disproportionate healthcare costs that foreign competitors do not. Small businesses paying $20,000+ per employee for health insurance are natural allies who don't know it yet.
Pillar 3: Conservative Reformers
Arnold Ventures — Houston-based philanthropy (John and Laura Arnold) funding evidence-based healthcare reform, including drug pricing transparency, Medicare sustainability, and market correction approaches. Niskanen Center — libertarian-leaning think tank advocating universal catastrophic coverage as a market-compatible path to universal access. American Enterprise Institute (AEI) — published extensively on reference pricing, Medicare Advantage competition models, and site-neutral payment. Committee for Responsible Federal Budget — fiscal conservatives who recognize that healthcare spending growth is the single largest threat to long-term fiscal sustainability.
Pillar 4: Faith Communities
National Association of Evangelicals — "For I was sick and you looked after me" (Matthew 25:36). Faith-based healthcare advocacy has deep roots in both progressive and conservative traditions. Catholic Health Association — the largest group of nonprofit healthcare providers in the nation, operating 1 in 6 hospital beds in America. State-level interfaith coalitions — the Connecticut SustiNet model's Interfaith Fellowship for Universal Health Care provides a template.
Pillar 5: Veterans and Military
American Legion and Veterans of Foreign Wars (VFW) — veterans understand both the value of government-provided healthcare (VA, TRICARE) and its inefficiencies. The 77% youth ineligibility rate for military service connects healthcare reform directly to national security. Council for a Strong America — nonpartisan organization of military leaders, law enforcement, business executives, and educators advocating for investments in youth.
Pillar 6: Rural and Agricultural
American Farm Bureau Federation and state Farm Bureaus — rural communities face the most acute healthcare access crisis, and agricultural employers face the same cost burdens as other businesses. 432 rural hospitals nationwide remain vulnerable to closure. When a hospital closes, it takes the local economy with it — businesses leave, young families leave, the tax base collapses.
Pillar 7: Healthcare Providers
State medical associations (frame as "administrative liberation" — physicians spend 30%+ of practice time on insurance paperwork), nurses' unions, hospital associations (particularly rural hospitals), community health centers, and the growing physician burnout advocacy movement.
Fundraising: The Tiered Budget Model
Budget Reality Check
A serious multi-state reform campaign requires $50–80M over its full duration, though initial phases require substantially less. The budget is structured in two tiers to match fundraising reality.
Tier 1: Phases 1–2 ($5–10M over 3–4 years)
| Year | Phase | Budget | Focus |
|---|---|---|---|
| Year 1 | Foundation | $1.5–2.5M | Coalition building, research, PAC formation |
| Year 2 | Phase 1 Push | $2–3M | Bill introduction, committee hearings, organizing |
| Year 3 | Phase 2 Push | $2.5–4M | Consumer protection bills, expanded media |
| Tier 1 Total | $5–10M | Achievable with existing networks | |
Counter-Messaging Framework
Bipartisan Counter-Messaging
| Opposition Claim | Bipartisan Counter-Message |
|---|---|
| "Government takeover of healthcare" | "This is anti-monopoly — breaking up the insurance bureaucracy that acts like a shadow government over your doctor. Real markets require real competition." |
| "You'll lose your doctor" | "Under the current system, you lose your doctor every time you change jobs or your employer switches plans. This gives you choice." |
| "It costs too much" | "We already spend $4.5 trillion — nearly double what other countries spend for better outcomes. This reduces waste and improves efficiency." |
| "Socialist medicine" | "Singapore achieves universal coverage through individual savings accounts and private providers. Indiana uses HSAs. Switzerland uses private insurers. Market-based reform isn't socialism — it's smart policy." |
| "Insurance job losses" | "The bill includes the most generous workforce transition in American history — and creates more care jobs than admin jobs lost." |
Chapter 23: The Campaign Timeline — From Research to Universal Care
The campaign timeline presents two scenarios: an optimistic case (6–8 years, 2026–2034) and a base case (10–12 years, 2026–2038) recommended for planning. [43]
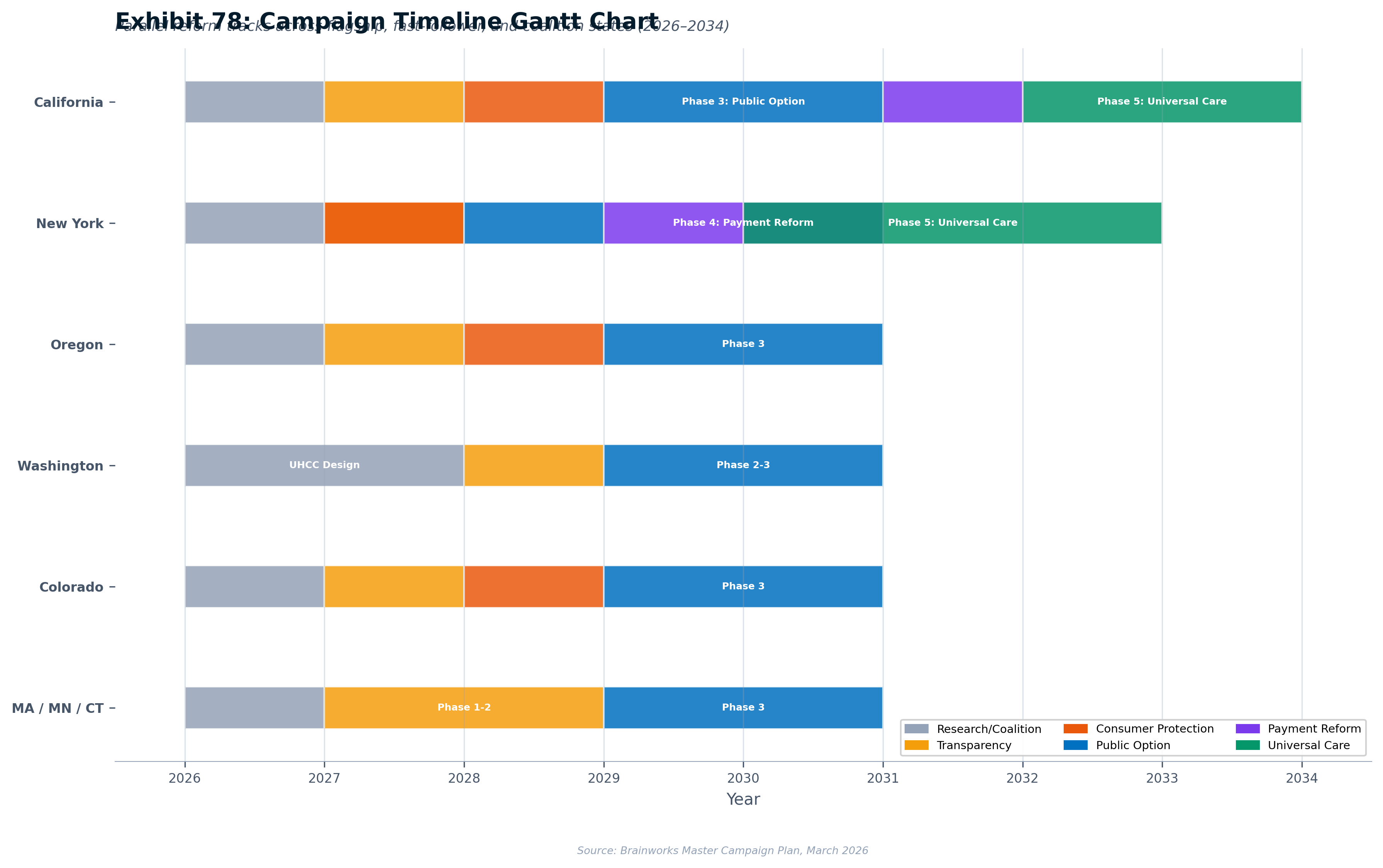
Base Case Timeline: 2026–2038
| Year | California Track | New York Track | Expansion States |
|---|---|---|---|
| 2026–2028 | Foundation; Phase 1 passage (2027) | Phase 1 passage (2027); union engagement | Study completion; initial legislation (OR/WA/CO) |
| 2029–2030 | Phase 2 passage; APCD operational | Phase 2 passage; Workers' Shield enacted | Phase 1 implementation; OH/AZ engagement |
| 2031–2032 | Phase 3 passage; public option enrollment | Phase 3 passage; Essential Plan expansion | Phase 2 expansion; GA coalition building |
| 2033–2035 | Phase 4 passage; all-payer rate setting | Phase 4 passage; global budgets | Phase 3; TX rural program pilot |
| 2036–2038 | Phase 5 — Universal Direct Care | Phase 5; full implementation | Critical mass; federal legislation |
The Cascade Effect
Each state victory makes the next easier through five channels: demonstration effect, workforce migration, interstate compacts, political contagion, and federal gravity. This is precisely how marriage equality, marijuana legalization, and Canadian universal healthcare all succeeded — state by state, with localized approaches that generated data and momentum for subsequent states. [44]
Chapter 24: Conclusion — From Analysis to Action
This report has now completed a three-part arc. Volume I proved that the American healthcare system's inefficiency and waste kills. Volume II traced the cash flows to show precisely how $1.8 trillion is consumed by administrative overhead, monopoly pricing, and misaligned incentives. Part III provides the plan to reform it — through bipartisan, phased, state-by-state action that draws on conservative and progressive models alike. [47]
The $1.8 Trillion Opportunity
Redirecting even a fraction of healthcare waste to actual patient care and productive economic investment would:
- Restore American competitiveness — eliminating the $15,000+/worker healthcare tax that no competitor bears
- Provide universal comprehensive coverage to every American at lower total cost
- Eliminate the $1.4 trillion employer healthcare burden, freeing businesses to invest in wages, hiring, and growth
- End the 100 million Americans carrying medical debt and 550,000 annual medical bankruptcies
- Unleash entrepreneurship by ending "job lock" — universal coverage countries have higher startup rates
- Strengthen military readiness by improving population health upstream of the 77% ineligibility crisis
- Restore the physician-patient relationship by eliminating the administrative burden driving 50%+ physician burnout [48]
A Call to Action
For Legislators: Phase 1 — transparency — is nearly impossible to vote against, regardless of party. Start there.
For Business Leaders: Healthcare costs are your single largest competitive disadvantage. You spend $15,000+ per worker that your German, Japanese, and Singaporean competitors do not. Join the coalition.
For Conservative Reformers: Market-based models exist. Indiana, Singapore, Switzerland, and Maryland prove that universal coverage can be achieved through HSAs, private insurers, and regulated competition — not government takeover.
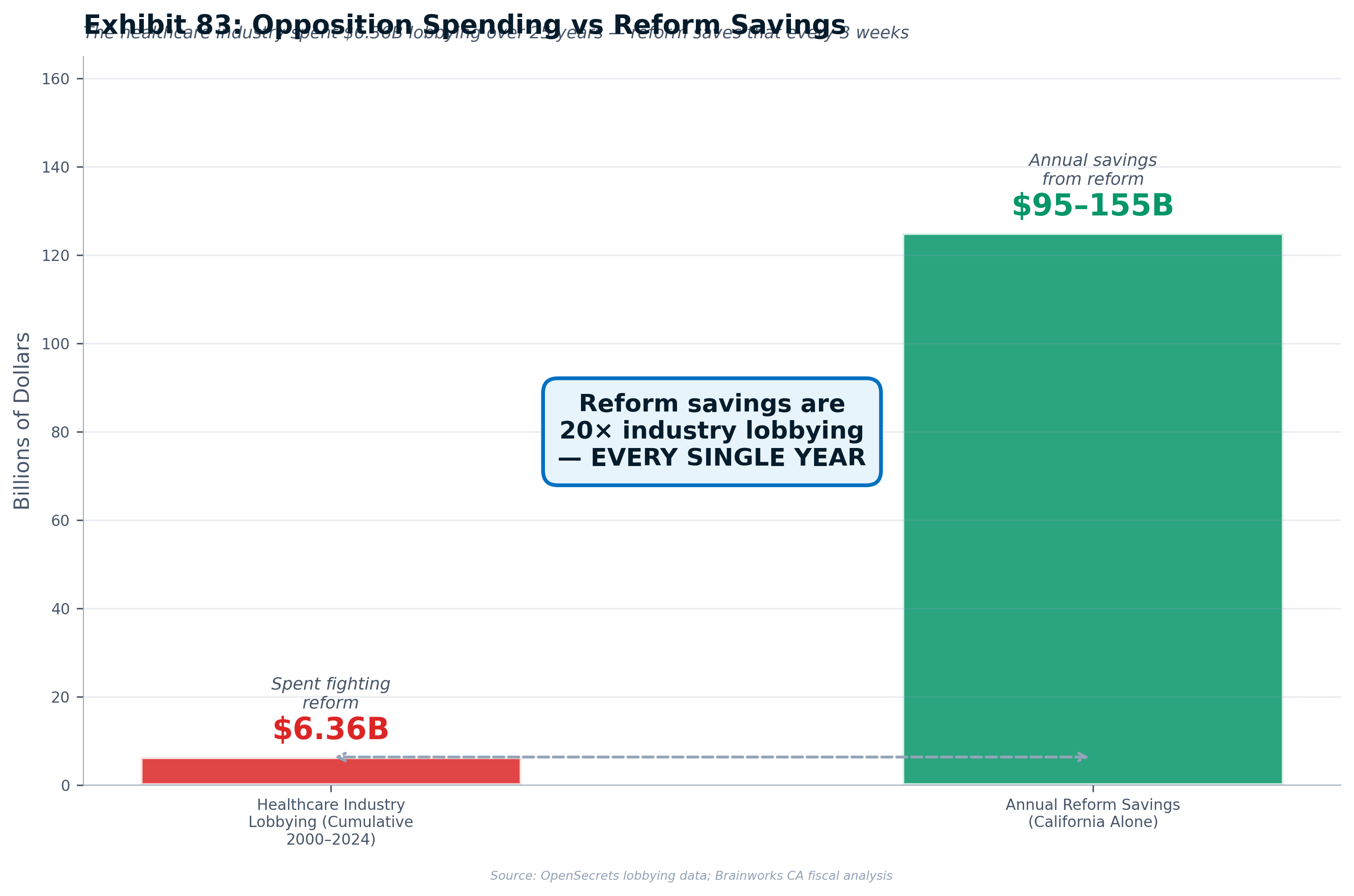
For Donors: This is a $50–80 million, 10–12 year investment that unlocks $40–80 billion in annual avoided cost growth. The opposition spends $100 million annually to protect the status quo. Your investment in reform is the highest-leverage philanthropic opportunity in American healthcare.
For Citizens: You are the constituency that makes reform politically possible. Call your legislator. Share your healthcare story. Vote for candidates who commit to reform.
What American Healthcare Could Look Like by 2040
Every resident is covered from birth, regardless of employment. You choose your doctor — any doctor. Your primary care physician knows you by name because their panel is 600 patients, not 2,500. There are no prior authorizations, no surprise bills, no medical debt. Administrative costs are 3% of total spending, not 34%. The same procedure costs the same amount at every hospital. Drug prices are negotiated at international benchmark rates.
This is not a fantasy. It is what every other wealthy nation has already achieved. It is what Massachusetts proved at the state level. It is what Canada built province by province. And it is what the five-phase strategy in this report is designed to deliver.
The healthcare cost crisis was not created in a day. It will not be resolved in a day. But it can be resolved — phase by phase, state by state, year by year — until the system serves patients, employers, and communities instead of enriching intermediaries.
From analysis to action. From waste to care.
The work begins now.
Chapter 25: The Legal Fortress — ERISA, Constitutional Defense, and Litigation Strategy
Every ambitious state healthcare reform will face legal challenge. This chapter maps the legal terrain and builds the litigation defense strategy — starting with ERISA, the single largest legal obstacle to state-level universal healthcare. [49]
ERISA Preemption: Why It's the #1 Obstacle
ERISA preempts state laws that "relate to" employee benefit plans, shielding self-insured employer health plans — which cover approximately 61% of all covered workers — from state insurance regulation. However, the Supreme Court has imposed limits: in Travelers (1995), the Court held ERISA does not reach laws of "general applicability" that only indirectly affect costs. In Rutledge (2020), the Court upheld state PBM regulation. [51]
Phase-by-Phase ERISA Exposure
| Phase | ERISA Risk | Key Vulnerability | Mitigation |
|---|---|---|---|
| Phase 1: Transparency | LOW | APCD data collection | Collect from TPAs, not plans directly |
| Phase 2: Consumer Protection | LOW-MOD | Prior auth doesn't reach self-insured | Rutledge supports PBM regulation |
| Phase 3: Real Competition | LOW | Voluntary plan — no ERISA mandate | Market competition, not regulation |
| Phase 4: Payment Reform | MODERATE | Rate setting indirectly affects self-insured | Travelers: regulates providers, not plans |
| Phase 5: Universal Coverage | MAXIMUM | Payroll assessment relates to employer plans | Tax-and-credit structure; federal waiver |
Three Strategic Scenarios
Scenario A (20–30% probability): Federal waiver legislation passes, explicitly waiving ERISA preemption. Scenario B (15–25%): Litigation narrows ERISA preemption using "generally applicable tax" structure. Scenario C (50–60%): Most likely — ERISA preemption remains. Phase 5 achieves functional universality at 85–90% coverage through the state system. The remaining 10–15% retain employer coverage while the public option is so efficient that employers voluntarily migrate.
The Honest Assessment
Full universality requires federal action. Our state strategy achieves 85–90% without it. The 85–90% coverage achieved through the state system — combined with the documented gap — becomes the most powerful argument for federal ERISA reform. Design for Scenario C; work toward Scenario A.
Chapter 26: Implementation — Technology, Systems, and the HealthCare.gov Lesson
Implementation failure is the silent killer of healthcare reform. HealthCare.gov's catastrophic 2013 launch nearly destroyed the ACA. This chapter applies those lessons. [57]
Core Principle
No big-bang launches. Every system deploys in phases, is load-tested before public launch, and has manual fallback procedures. Build IT before coverage.
HealthCare.gov Lessons Applied
| HealthCare.gov Failure | Our Mitigation |
|---|---|
| No single accountable leader | Single Chief Health Information Officer |
| Big-bang launch | Phased rollout: large payers first, then mid-size, then small |
| Tested for 200 users; 250,000 tried | Load testing at 5x projected peak |
| No manual fallback | Manual fallback for all critical paths |
| Multiple prime contractors blamed each other | Single prime contractor with performance bonds |
Chapter 27: Workforce Transition and Rural Health
The two most potent opposition attacks against healthcare reform are "job killer" and "abandons rural communities." This chapter provides detailed plans that neutralize both — and convert them into campaign strengths. [63]
Part A: The Workforce Transition
Healthcare reform will restructure the healthcare labor market. This is a managed transition from bureaucratic jobs to care jobs. The insurance intermediation system employs approximately 530,000 workers nationally in roles that exist solely to process administrative complexity. The phased approach means workforce impacts are gradual — no single phase eliminates a large number of jobs.
The Direct Care Workforce Transition Act — $3–5 Billion
| Program | Details | Est. Cost |
|---|---|---|
| Salary Continuation | 24 months at 80% of previous salary (capped $100K/yr) | $1.5–2.5B |
| Retraining Programs | Healthcare IT, Clinical Support, Public Health Admin, Entrepreneurship | $0.7–1.2B |
| Early Retirement | Workers 55+: 36 months at 70%, full health coverage until Medicare | $0.5–0.8B |
| Priority Hiring | 50%+ of new public system positions from displaced workers | $50–100M |
| Total | Over 8–12 year transition period | $3.0–5.1B |
Cost-benefit context: The $3–5B transition cost is less than one month of the estimated $30–60B in annual savings from Phase 5.
Part B: Rural Health Strategy
Each phase specifically helps rural communities: Phase 1 reveals the access gap quantitatively, Phase 2 reform benefits rural providers lacking staff to fight denials, Phase 3 mandates hospital participation, Phase 4 global budgets stabilize rural hospital finances (the Maryland model has kept rural hospitals open for decades), and Phase 5 universal coverage eliminates uncompensated care — the #1 financial burden driving rural hospital closures.
Messaging: The Core Frame
"We're replacing bureaucratic jobs with care jobs." The current system employs ten administrators for every physician. Our reform invests in people who take care of you, not people who deny your claims.
Chapter 28: The AI-Personalized State Legislative Engine
The healthcare reform campaign outlined in this report — phased legislation across ten states over 2026–2038 — faces a fundamental strategic dilemma. The problems are national, but the political systems that must address them are radically local. A strategy that resonates in Austin will fall flat in Ann Arbor. Language that mobilizes coalitions in Atlanta will alienate potential allies in Phoenix. This chapter presents the AI-Personalized State Legislative Engine — the technology that makes a fifty-state campaign possible with a small team. [69]
The Strategic Dilemma: Unified vs. Localized Messaging
There are two fundamental approaches to advancing reform across multiple states:
Strategy A: Unified Compromise Language. A single, carefully crafted bipartisan framing deployed identically everywhere. Advantages: consistent national brand, simple media management, easier coalition coordination. Disadvantages: lowest-common-denominator messaging that inspires no one, fails to activate state-specific emotional triggers, ignores vast political culture differences, and is vulnerable to localized opposition.
Strategy B: AI-Hyper-Personalized State Engine. An AI-powered system generating state-specific legislative language, bill names, coalition strategies, lobbying kits, testimony templates, and counter-messaging — all customized to each state's unique political culture. Advantages: maximum political resonance, activates state-specific coalitions, responsive to opposition. Disadvantages: operational complexity, coordination risk.
Historical Evidence: Localization Wins
The historical record strongly favors localized approaches:
- The ACA (unified — struggled): Consistent national messaging couldn't adapt to local political cultures. The ACA was successfully rebranded by opponents in conservative states as "Obamacare — a government takeover." Yet Medicaid expansion succeeded precisely where it was localized — Montana called it "HELP," Louisiana framed it as fiscal responsibility, Virginia framed it as bringing tax dollars home.
- Marriage equality (localized — succeeded): In Iowa, the campaign emphasized "Iowa values — fairness, treating neighbors right." In New Hampshire, "live free or die" libertarian principles. In Maryland, civil rights legacy. In Maine, family and personal freedom. Different spokespeople, different ads, different coalitions in every state. Result: 27% support in 1996 to Supreme Court victory in 2015.
- Marijuana legalization (localized — succeeded): Colorado emphasized tax revenue. Washington emphasized ending wasteful incarceration. Oregon emphasized regulation and safety. From zero legal states in 2011 to 24 recreational states by 2026.
- Gun control (unified — mostly failed): Despite 60–90% polling support for specific measures, the unified "common-sense gun safety" approach has failed to make inroads in competitive or conservative states.
The Hybrid Conclusion
Strategy A for the Roof — Strategy B for the Foundation
Strategy A (Unified) for: Federal legislative coordination, national media, national coalition partners (AARP, AMA), donor communications, umbrella brand identity.
Strategy B (State Engine) for: State-specific bill drafting and naming, state-level coalition building, lobbying kits and testimony templates, opposition monitoring and counter-messaging, campaign management in each state.
The relationship is architectural: Strategy A is the roof — visible, providing identity. Strategy B is the foundation — customized to the terrain of each state, doing the structural work. A roof without walls is a kite. Walls without a roof is a ruin. You need both.
AI State Engine Architecture
The Engine has five layers:
| Layer | Function | Content |
|---|---|---|
| 1. Master Template Library | Policy core | Parameterized model legislation, lobbying kits, testimony templates, media kits, opposition rebuttals at 3 ambition tiers |
| 2. State Intelligence Database | Political intelligence | Political landscape, key actors (50–100 profiles/state), cultural values mapping, healthcare/AI data, opposition mapping |
| 3. AI Adaptation Layer | Content generation | Combines templates + intelligence to produce fully customized state-specific outputs |
| 4. Human Review Gate | Quality control | Two-stage review: state coordinator validates politics, local partner validates authenticity |
| 5. Feedback Loop | Learning system | Tracks outcomes, polling, media, opposition — feeds back to improve future outputs |
State Customization Parameters
Political Culture Vectors
Each state receives scores on four continuous dimensions: Liberty ↔ Community (0–100), Individual ↔ Collective (0–100), Market ↔ Government (0–100), and Tradition ↔ Progress (0–100). These scores calibrate the rhetorical orientation of all generated content.
Framing Archetypes
Each state is assigned a primary and secondary archetype: Fiscal Conservative ("This saves taxpayer money"), Social Justice ("This addresses inequality"), Populist ("The little guy is getting screwed"), Libertarian ("Protect individual choice"), Communitarian ("Our communities are suffering"), or Pragmatic ("Look at the data — it works").
Linguistic Parameters
Each state maintains taboo word lists (words the AI must never use) and power word lists (words the AI prioritizes), plus rhetorical style guides covering formality, data density, emotional intensity, and humor tolerance.
The Content Generation Pipeline: 10 Stages
| Stage | Output | Cycle Time |
|---|---|---|
| 1. Bill Name & Branding | 5–7 candidates → 3 finalists for human review | 2 hours + 24–48 hr review |
| 2. Executive Summary | 1–2 page state-specific summary | 3 hours + 24–48 hr review |
| 3. Full Bill Language | Complete bill text for legislative counsel | 8 hours + 3–5 day legal review |
| 4. Lobbying Kit | Fact sheets, policy briefs, legislator leave-behinds, talking points, FAQ | 6 hours + 48–72 hr review |
| 5. Media Kit | Press releases, op-eds, social media package, spokesperson talking points | 8 hours + 48–72 hr review |
| 6. Opposition Rebuttal | Rebuttals, rapid response templates, counter-advertising scripts | 6 hours + 48–72 hr review |
| 7. Coalition Pitches | Customized recruitment for business, labor, faith, veterans, rural, healthcare providers | 8 hours + 48–72 hr review |
| 8. Campaign Timeline | Phase-by-phase timeline with state legislative calendar | 4 hours + 24–48 hr review |
| 9. Budget & Fundraising | Campaign budget, funding sources, grassroots plan | 4 hours + 48–72 hr review |
| 10. Counter-Advertising | TV, radio, digital, print scripts tuned to state culture | 8 hours + 72–96 hr review |
| Complete State Kit | All 10 stages | 5–7 business days |
Total turnaround: 5–7 business days for a complete, state-specific campaign kit. Traditional methods require 4–7 weeks and dedicated staff per state. The AI Engine makes a 10-state simultaneous campaign possible with a small team.
Five Contrasting State Examples: Same Policy, Different Packaging
The following examples demonstrate how the same healthcare reform goal — introducing real competition to insurance markets dominated by monopolies — receives completely different political packaging in five states:
🤠 Texas: "Free Market Healthcare Competition Act"
Culture vector: Maximum liberty, maximum individual, maximum market. Archetype: Libertarian/Fiscal Conservative.
Framing: "Texas hospitals are being bought up by out-of-state corporate chains that eliminate competition and raise prices. Texas taxpayers are subsidizing $47 billion in annual healthcare waste. This bill restores real free market competition."
Coalition targets: Texas Farm Bureau, NFIB Texas, faith communities, veterans' organizations, rural hospital administrators, Texas Medical Association.
Taboo words: "regulation," "government program," "mandate," "universal," "European model."
Power words: "freedom," "choice," "competition," "Texas-led," "protecting Texans."
| Opposition Attack | Texas Counter-Response |
|---|---|
| "DC telling Texas how to run healthcare" | "This is Texas protecting Texans from out-of-state insurance monopolies that are shutting down our rural hospitals" |
| "Government takeover" | "This is anti-government — it breaks up the insurance bureaucracy that acts like a shadow government over your doctor" |
| "Too expensive" | "Texans are already paying $47 billion a year in healthcare waste. This saves money" |
🌴 California: "Healthcare Justice & Efficiency Act"
Culture vector: High community, moderate collective, maximum progress. Archetype: Social Justice/Pragmatic.
Framing: "California's communities of color face healthcare outcomes that would be unacceptable in any other wealthy state. Insurance bureaucracies consume $62 billion annually. California can lead the nation in showing that equitable healthcare is also efficient healthcare."
Coalition targets: CNA, SEIU-UHW, tech progressives, environmental justice, immigrant rights, community health centers.
Taboo words: "deregulation," "market-only solutions," "colorblind," "trickle-down."
Power words: "equity," "justice," "community," "innovation," "accountability."
🏭 Ohio: "Save Our Hospitals Act"
Culture vector: High community, moderate balance across dimensions. Archetype: Communitarian/Populist.
Framing: "31 Ohio hospitals have closed or cut services. When a hospital closes, the nearest ER might be 45 minutes away — for a heart attack, that's the difference between life and death. Meanwhile, insurance executives are taking home eight-figure bonuses."
Coalition targets: Ohio Hospital Association, UAW, AFSCME, community colleges, rural municipal governments, faith communities, small-town mayors.
Taboo words: "coastal," "progressive," "disruption," "transformation," "global competition."
Power words: "community," "our hospitals," "Ohio workers," "practical," "common sense."
🍑 Georgia: "Georgia Healthcare Freedom Act"
Culture vector: Moderate across all dimensions with enormous internal diversity. Archetype: Pragmatic/Fiscal Conservative.
Framing: "Georgia is #1 for business — but healthcare costs are making it harder to compete. Insurance bureaucracy costs Georgia businesses $22 billion annually. Meanwhile, rural Georgia hospitals are closing and communities are dying."
Coalition targets: Metro Atlanta Chamber, Georgia Hospital Association, HBCUs, faith communities, Georgia Farm Bureau, Georgia Tech, bipartisan legislative sponsors.
Taboo words: "liberal," "mandate," "redistribution," "Northern model."
Power words: "Georgia-grown," "business-friendly," "innovation," "freedom," "opportunity."
🌵 Arizona: "Arizona Healthcare Choice Act"
Culture vector: High liberty, high individual, moderate market. Archetype: Libertarian/Pragmatic.
Framing: "Arizonans don't have real healthcare choice today. In most counties, one insurance company controls the entire market. That's not a free market — that's a monopoly wearing a free-market costume. This bill breaks up monopolies, expands real choice, and puts Arizonans back in control."
Coalition targets: Libertarian organizations, small business associations, tribal nations, retiree communities, Arizona Farm Bureau, ASU/U of A.
Taboo words: "mandate," "federal," "California model," "regulation," "government program."
Power words: "choice," "freedom," "independence," "Arizona solutions," "competition."
Operational Model: Sub-Linear Scaling
| Phase | States Active | Core Team | State Coordinators | Total |
|---|---|---|---|---|
| Phase 1 (Pilot) | 2 | 5 | 1 | 6 |
| Phase 2 (Expand) | 10 | 5 | 3 | 8 |
| Phase 3 (Scale) | 20 | 5 | 6 | 11 |
| Phase 4 (National) | 35 | 5 | 10 + 1 deputy | 16 |
| Phase 5 (Full) | 50 | 5 | 15 + 3 deputies | 23 |
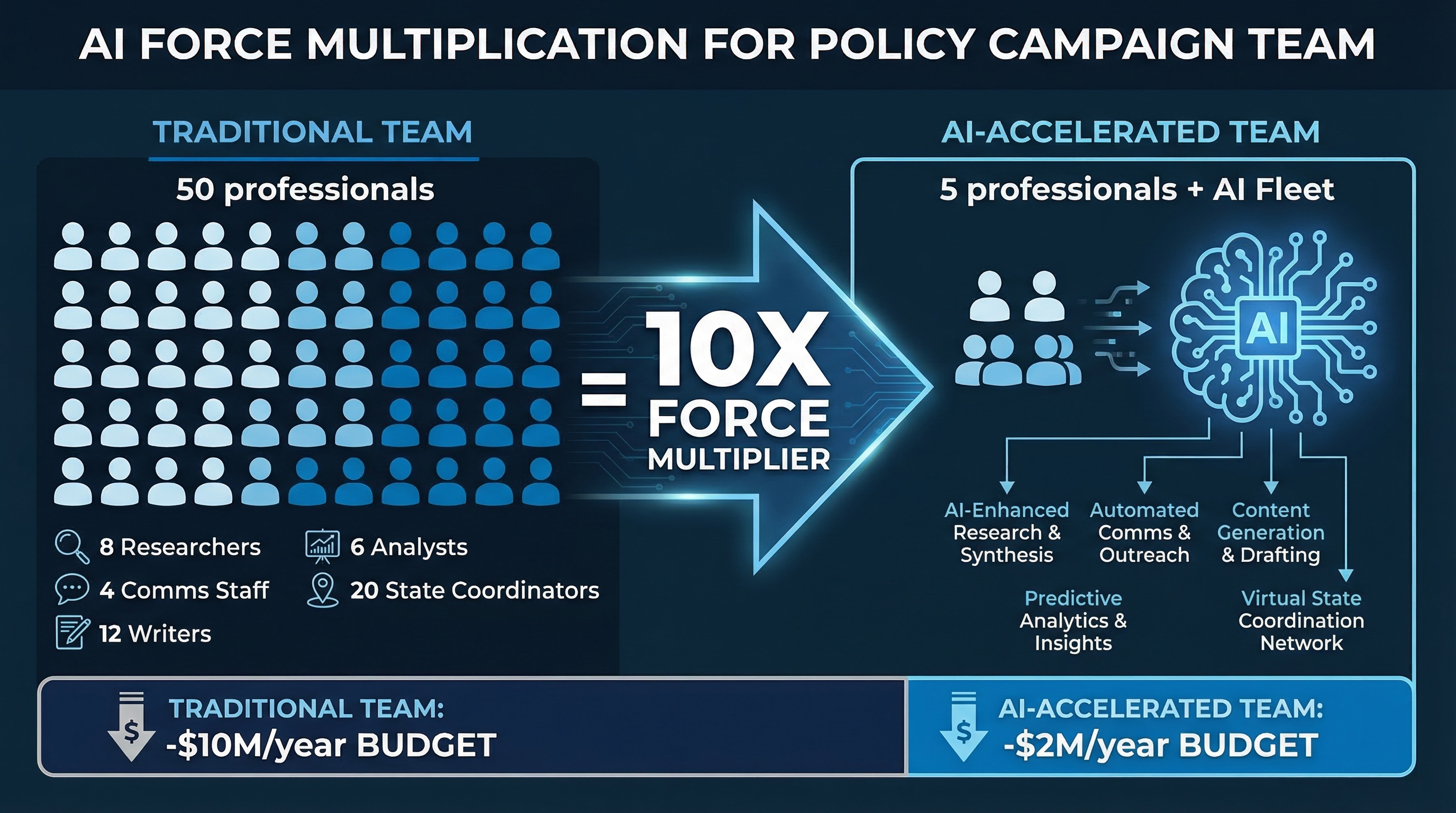
The AI handles content production that would normally require dozens of additional staff. Doubling the number of states does not double the team — it adds state coordinators (the irreducibly human role) while the AI scales content production at marginal cost.
What AI Cannot Replace
- Relationships: Building trust with legislators, coalition partners, and community leaders requires human connection
- Political judgment: Knowing when to push, when to compromise, when to walk away
- Public testimony: A nurse testifying about losing a patient to a prior authorization denial moves legislators. AI produces the draft; humans deliver the moment
- Coalition management: Navigating competing priorities and institutional politics is fundamentally human work
- Ethical oversight: Every AI-produced output must be reviewed for accuracy, tone, and alignment with campaign values
Chapter 29: The Campaign Arsenal — Asset Inventory, Startup Guide, and AI-Accelerated Deployment
This chapter catalogs every asset produced, provides a startup sequence, and outlines the operational model.
Complete Asset Inventory
Volume I–II: 16 chapters | ~33,700 words | 79 exhibits — The Healthcare Cost Crisis analyzed across insurance intermediation, pharmaceutical pricing, hospital financial engineering, private equity consolidation, administrative complexity, and vertical integration.
Part III: 14 chapters | ~50,000+ words — Five-phase legislative strategy, ten state profiles, bipartisan coalition architecture, AI State Engine specification, legal fortress, implementation plan, workforce transition.
Research Documents: 8 reports totaling ~38,500 words — Massachusetts case study, failed attempts analysis, international models, state political landscapes.
Strategy Drafts: 10 documents totaling ~80,000+ words — State legislative sequences, model bills, campaign plans, fundraising strategy, legal defense.
Lobbying Kit: ~15,600 words — Fact sheets, talking points, testimony templates, media kit, opposition rebuttals.
v3.0 Additions: Competitiveness crisis chapter, AI State Engine specification, 10-state expanded profiles, conservative reform models, bipartisan coalition expansion, Part IV bridge.
Startup Guide — Week by Week
| Timeline | Key Tasks | Deliverables |
|---|---|---|
| Weeks 1–2 | Read foundational materials; assemble core team; establish legal entity; secure $300–500K seed | Strategy memo, job descriptions, filed articles |
| Weeks 3–4 | Anchor organization outreach; legislator mapping; opposition research; media landscape scan | Signed LOIs, legislator contact list, opposition memo |
| Month 2 | Phase 1 bill drafting; coalition MOUs signed; lobbying kit production; donor cultivation | Bill text, 8–10 signed MOUs, complete lobbying kit |
| Months 3–4 | Phase 1 bill introduction; committee testimony planning; grassroots launch; media campaign | Bills introduced, witness lists, 3–5 op-eds placed |
| Months 5–8 | Committee hearings, amendments, markup; sustained media; grassroots pressure | Committee passage by month 8 |
| Months 9–12 | Floor debate prep; message discipline; governor confirmation | Floor passage — Phase 1 bill signed into law |
AI-Accelerated Content Production
| Content Type | Traditional Time | AI-Accelerated | Multiplier |
|---|---|---|---|
| State lobbying kit | 4–7 weeks | 5–7 days | 5–7× |
| Legislative testimony | 2–3 days | 2–4 hours | 8–12× |
| Opposition rapid response | 24–48 hours | 2–4 hours | 8–12× |
| Grant proposal | 2–4 weeks | 3–5 days | 4–6× |
| Daily media briefing | 2–3 hours/day | 15 min review | 8–12× |
| State policy comparison | 1–2 weeks | 1–2 days | 5–10× |
Chapter 30: Bridge to Part IV — Healthcare and AI Displacement
Healthcare costs and AI-driven workforce displacement are not separate crises. They are two faces of the same national competitiveness emergency — and they compound each other in ways that make addressing either one alone insufficient.
How Healthcare Costs Make AI Displacement Worse
In the United States, unlike every other wealthy nation, health insurance is tied to employment. When a worker is displaced by AI automation, they don't just lose their income — they lose their healthcare. This means:
- The human cost of displacement is doubled: A displaced worker in Germany loses income but retains healthcare. A displaced worker in America loses both — and faces potential medical bankruptcy on top of unemployment.
- "Job lock" prevents proactive transition: Workers who might voluntarily retrain for AI-era careers stay in vulnerable jobs because they can't afford to lose insurance during the transition.
- COBRA is a fiction: The option to continue employer coverage at full cost ($25,000+/year for a family) is financially impossible for most displaced workers.
- The safety net is weakest where displacement is greatest: States with the highest AI exposure (tech hubs in Texas, Georgia, Arizona) often have the weakest healthcare safety nets — non-expansion Medicaid, high uninsured rates, limited public options.
How AI Displacement Makes Healthcare Costs Worse
- Rising uninsured population: As AI displaces workers, more Americans lose employer-sponsored coverage, increasing the uninsured population and the uncompensated care burden that drives up costs for everyone else.
- Delayed care becomes emergency care: Displaced workers who lose insurance delay preventive care, leading to more expensive emergency interventions.
- Mental health crisis: Job displacement causes depression, anxiety, and substance abuse — all of which increase healthcare costs dramatically.
- Safety net strain: Medicaid and emergency rooms absorb displaced workers who lose private coverage, increasing public healthcare spending.
The Integrated Solution
Parts III and IV of this report together address the two biggest threats to American economic competitiveness:
| Threat | Part III Response | Part IV Response | Combined Effect |
|---|---|---|---|
| Healthcare cost crisis | Five-phase state reform strategy eliminating waste and introducing competition | AI workforce programs include healthcare continuation guarantees | Universal coverage provides the security foundation for economic transition |
| AI workforce displacement | Healthcare reform frees employers to invest in workforce development instead of insurance premiums | AI Transition Fund, retraining programs, wage insurance | Workers can transition to AI-era careers without losing healthcare — making adaptation voluntary, not desperate |
| National competitiveness | Eliminates the $15,000+/worker healthcare tax on American employers | Creates AI-ready workforce competitive with China, EU, Singapore | America competes on innovation and productivity, not on who can absorb the most healthcare waste |
The Bottom Line
You cannot build a resilient AI-era economy on a healthcare system that strips workers of insurance when they're displaced. And you cannot fix healthcare costs when the workforce is too insecure to support reform. Parts III and IV are not separate policy agendas — they are two halves of the same national competitiveness strategy.
Part III Bibliography
- [1] Analysis of Vermont (Act 48, 2011), California (AB 1400, 2022; AB 2200, 2024; AB 1900, 2026), Colorado (Amendment 69, 2016), Oregon (HB 3260, 2013; SB 770, 2019; SB 1089, 2023), and New York (NY Health Act, introduced 1991). See Chapter 21 for detailed case studies.
- [2] Massachusetts General Court, Chapter 58 of the Acts of 2006; Blue Cross Blue Shield Foundation of Massachusetts, "10 Years of Impact" (2016).
- [3] Doonan, M.T. & Tull, K.R., "Health Care Reform in Massachusetts," Milbank Quarterly (2010).
- [4] Based on existing OHCA authority under California Health and Safety Code §127500 et seq.
- [5] OIG, "Medicare Advantage Prior Authorization Denials" (2024); Maryland HSCRC rate-setting data (1977–present).
- [6] Washington State SB 5526 (Cascade Care, 2019); Colorado HB 21-1232 (Colorado Option, 2021).
- [7] Maryland Total Cost of Care Model evaluation reports; Busse, R. & Blümel, M., "Germany: Health System Review," Health Systems in Transition (2014).
- [8] Cheng, T.M., "Taiwan's New National Health Insurance Program," Health Affairs (2003); Himmelstein, D.U. et al., Annals of Internal Medicine (2020).
- [9] Vermont Workers' Center response to Governor Shumlin's decision (December 2014).
- [10] Gruber, J., "Covering the Uninsured in the U.S.," Journal of Economic Literature (2008).
- [11] California Health and Human Services Agency, H.R. 1 impact analysis (2025).
- [12] CalMatters, "California Governor's Race 2026: Healthcare Positions" (February 2026).
- [13] David Binder Research poll commissioned by CNA/NNU (February 2026).
- [14] HCAI/OHCA reports (2025–2026); AB 1415 and SB 351 legislative analysis.
- [19] New York Health Act legislative history: A.6058/S.7590 (2021-22), A.1466/S.3425 (2025-26).
- [20] Campaign for New York Health analysis of Senate blockage.
- [22] Workers' transition provisions modeled on Massachusetts Chapter 58.
- [23] Governor Hochul, H.R. 1 response executive budget proposals (2025-2026).
- [26] One Payer States state tracking; NASHP state healthcare transformation database.
- [32] Comprehensive analysis of six state reform attempts (2006–2026) plus international models.
- [33] Long, S.K., "On the Road to Universal Coverage," Health Affairs (2008).
- [35] Synthesis from all major state reform attempts and international models.
- [37] McDonough, J., "Inside National Health Reform" (2011).
- [43] Timeline based on Massachusetts implementation (2004–2007), Canada's cascade (1947–1971).
- [44] Cascade effect analysis based on ACA experience and Canada's provincial cascade.
- [47] "The Healthcare Extraction Machine," Volumes I and II, Brainworks Ventures (2025–2026).
- [48] Galvani, A.P. et al., "Universal healthcare as pandemic preparedness," PNAS (2022).
- [49] ERISA, 29 U.S.C. §1001 et seq.
- [51] Shaw v. Delta Air Lines, 463 U.S. 85 (1983); Travelers, 514 U.S. 645 (1995); Rutledge v. PCMA, 592 U.S. ___ (2020).
- [57] GAO-15-238, "Healthcare.gov: CMS Has Taken Steps to Address Problems" (March 2015).
- [63] Workforce transition: PERI fiscal analysis of the New York Health Act (Gerald Friedman).
- [69] Brainworks AI campaign production metrics, March 2026.
v3.0 Additional Sources: KFF 2025 Employer Health Benefits Survey; Peterson-KFF Health System Tracker (March 2026); Peter G. Peterson Foundation (October 2025); OECD Health at a Glance 2025; Himmelstein et al., Annals of Internal Medicine (2019); Mercer 2025 National Survey; Madrian, B.C., "Employment-Based Health Insurance and Job Mobility," QJE (1993); CFPB medical debt reports; Cornell ILR School bankruptcy statistics; CRS IF12660 (FY2025 MHS); Military.com (September 2022); CDC "Unfit to Serve" (June 2023); Urban Institute Federal Evaluation of Indiana HIP 2.0 (October 2025); AHA Value Initiative Case Study — Intermountain Health (2019); Commonwealth Fund International Health Policy Center — Singapore Profile; Michigan Journal of International Law — Swiss Healthcare (January 2024); Heritage Foundation healthcare proposals (1989–2025); AEI Health Policy publications; Niskanen Center universal catastrophic coverage proposals; Arnold Ventures healthcare reform program; Maryland HSCRC 47-year evaluation data; Marriage equality campaign analysis (Freedom to Marry); Marijuana legalization state-by-state data; Strategy comparison research (Brainworks, March 2026); State profiles research (Brainworks, March 2026); National competitiveness data compilation (Brainworks, March 2026).