The Extraction Machine: How American Healthcare Converts Patient Dollars to Corporate Profit

Executive Summary
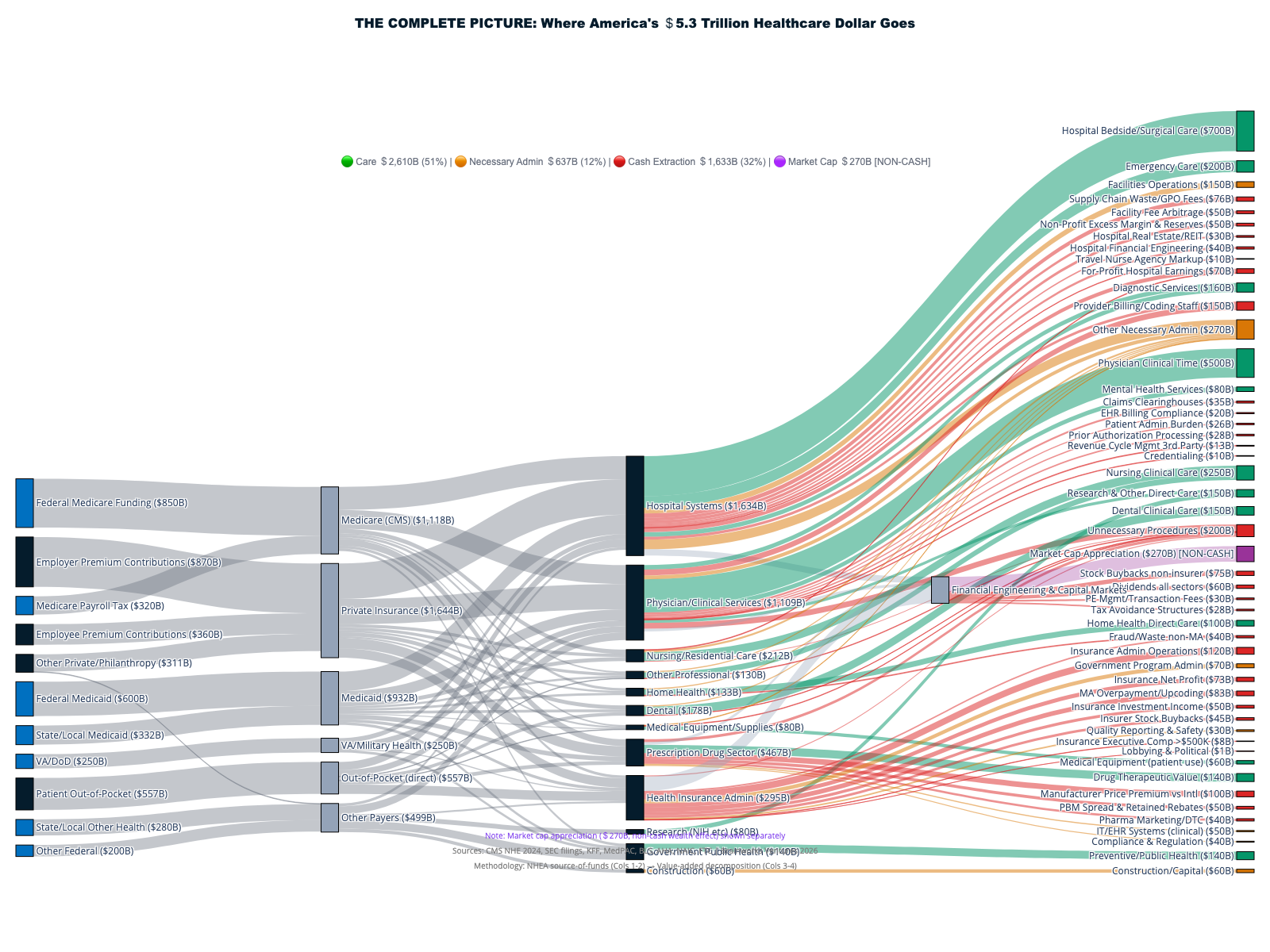
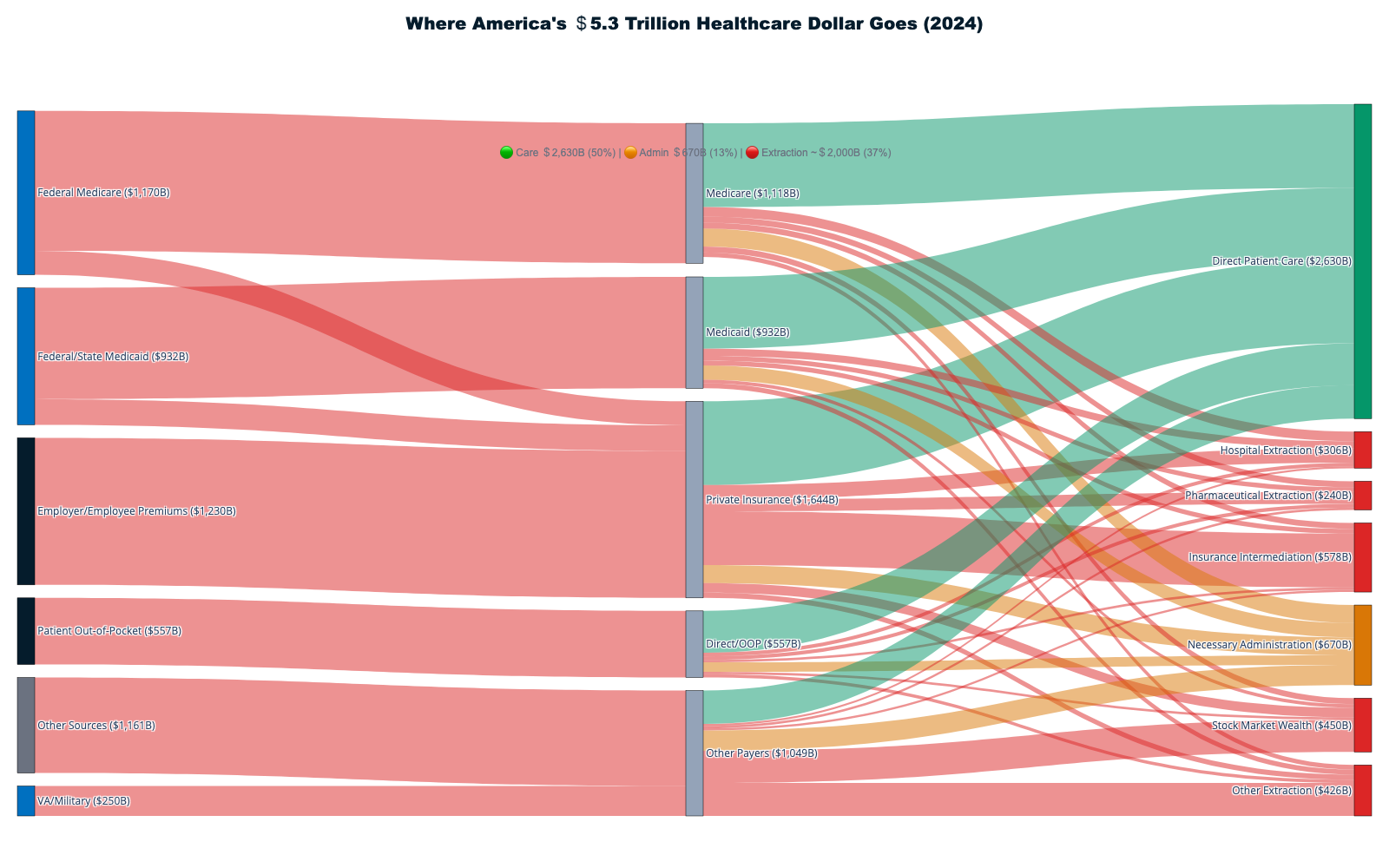
This report documents how $1.8+ trillion in cash is extracted annually from America's $5.3T healthcare system through financial engineering, administrative complexity, and corporate consolidation — with an additional $270B in stock market wealth creation amplifying extraction into permanent shareholder value. Only 42¢ of each healthcare dollar reaches direct patient care. The remaining 58¢ flows to insurance intermediation ($578B), shareholder cash returns ($180B), pharmaceutical manipulation ($240B), administrative overhead, and other extraction layers that add no clinical value.
Building on Volume I's statistical model of healthcare economic extraction, this volume follows the money — naming names, tracing cash flows, and exposing the specific mechanisms through which extraction operates. Together, the two volumes provide the most comprehensive forensic investigation of American healthcare finance ever assembled.
Including 19 Interactive Sankey Diagrams
Introduction: The Architecture of Extraction
Volume I of this investigation established the statistical framework quantifying healthcare extraction across the American economy, revealing systematic correlations between insurance company revenue optimization and declining health outcomes. This volume turns from the 'what' to the 'how' — a forensic investigation tracing every dollar through the extraction machine, from the premium payment to the stock buyback.
In 2024, Americans spent $5.3 trillion on healthcare—$15,474 for every man, woman, and child—yet the most shocking revelation is not how much we spend, but where those dollars actually go before any medical care reaches patients. [1] Every healthcare dollar passes through a sophisticated extraction machine that systematically diverts funds from patient care to corporate profit centers, creating the largest wealth transfer operation in the American economy.
Understanding Hospital Extraction ($306B): For-Profit and Nonprofit Alike
The hospital extraction figure encompasses both for-profit hospital systems and the substantial financial surpluses generated by nominally "nonprofit" institutions. The $306B breaks down as follows:
- For-profit hospital net income: $85B — HCA Healthcare alone generated $5.8B in net income (2024) on $70.6B revenue, with $10B earmarked for stock buybacks. [22]
- Nonprofit hospital "operating surplus": $65B — functionally identical to profit. Mayo Clinic reported $16.3B revenue with a $2.3B operating margin [123]; Cleveland Clinic generated comparable surpluses. These billions fund executive compensation ($5-15M CEO salaries), cash reserves exceeding $100B system-wide, and expansion — functionally indistinguishable from for-profit extraction.
- Facility fee arbitrage: $95B — hospitals charge 87% more for identical services performed in hospital outpatient departments versus independent physician offices, exploiting Medicare's site-of-service payment differential. A $150 office visit becomes a $280 hospital outpatient encounter for the same physician performing the same procedure. [24]
- Hospital-driven supply chain markups: $61B — group purchasing organizations (GPOs) and hospital supply chains add layers of intermediation that inflate device and supply costs while generating administrative fees and kickbacks.
The distinction between for-profit and nonprofit hospitals has become largely semantic: nonprofit hospital CEOs routinely earn $5-15 million annually [18], and the ratio of nonprofit hospital CEO compensation to median worker wages has widened from 7:1 (1990) to over 20:1 today. Nonprofit hospital systems generate billions in "operating margin" that funds executive compensation packages rivaling Wall Street, cash reserves larger than most countries' healthcare budgets, and empire-building acquisitions — all while claiming tax exemptions worth an estimated $28B annually in exchange for "community benefit" that often consists primarily of bad debt reclassified as charity care.
Who Captures the $270B in Annual Market Cap Appreciation?
The $270B non-cash wealth effect breaks down by sector: health insurance companies (~$95B, with UnitedHealth alone appreciating from $39B to $265B market cap), pharmaceutical companies (~$85B), hospital systems (~$35B), medical devices and health IT (~$30B), and PBMs/pharmacy chains (~$25B). These gains are concentrated: the top three institutional investors (Vanguard, BlackRock, State Street) collectively own approximately 20% of every major healthcare company [17], creating common ownership patterns that academic research has linked to reduced competitive incentives.
Who are the concrete recipients? Based on SEC 13F filings for UnitedHealth Group (86% institutional ownership), CVS Health (84% institutional), and HCA Healthcare (91% institutional), the $270B in annual market cap appreciation flows approximately as follows:
- ~25-30% to the "Big Three" index fund managers (Vanguard ~9%, BlackRock ~8%, State Street ~4% of major healthcare stocks) — passive investors who hold shares indefinitely, compounding the wealth effect across market cycles
- ~20% to pension and retirement funds — public employee pensions (CalPERS, New York State), 401(k) plans, and sovereign wealth funds. These represent the only pathway through which ordinary Americans indirectly benefit from healthcare extraction
- ~15% to hedge funds and active managers — firms like Capital Group, Fidelity, and Wellington that trade on extraction optimization signals
- ~10-15% to corporate insiders and executives — through stock-based compensation, option exercises, and insider sales. UnitedHealth CEO Andrew Witty's 2024 compensation was 82% stock-based ($21.5M in equity awards)
- ~20-25% to retail and individual shareholders — direct stock ownership, self-directed IRA accounts, and brokerage portfolios
The concentration of ownership means healthcare extraction wealth accrues primarily to the already-wealthy: the top 10% of American households own 93% of stocks. For the median American family paying $25,000 annually in healthcare costs, the stock market wealth their premiums generate flows overwhelmingly to institutional investors and corporate executives — not back to patients.
The single most devastating finding: stock market wealth creation from healthcare extraction now reaches $300-600 billion annually—10 to 30 times larger than reported industry profits. UnitedHealth Group's market capitalization expanded from $39 billion in 2010 to $265 billion in 2026, representing $226 billion in shareholder wealth creation funded entirely by patient premiums and taxpayer subsidies. [2] Health insurer stocks increased 1,032% from ACA enactment through 2024, compared to 251% S&P 500 growth—a 4:1 outperformance that proves extraction as successful investment thesis rather than healthcare delivery. [3]
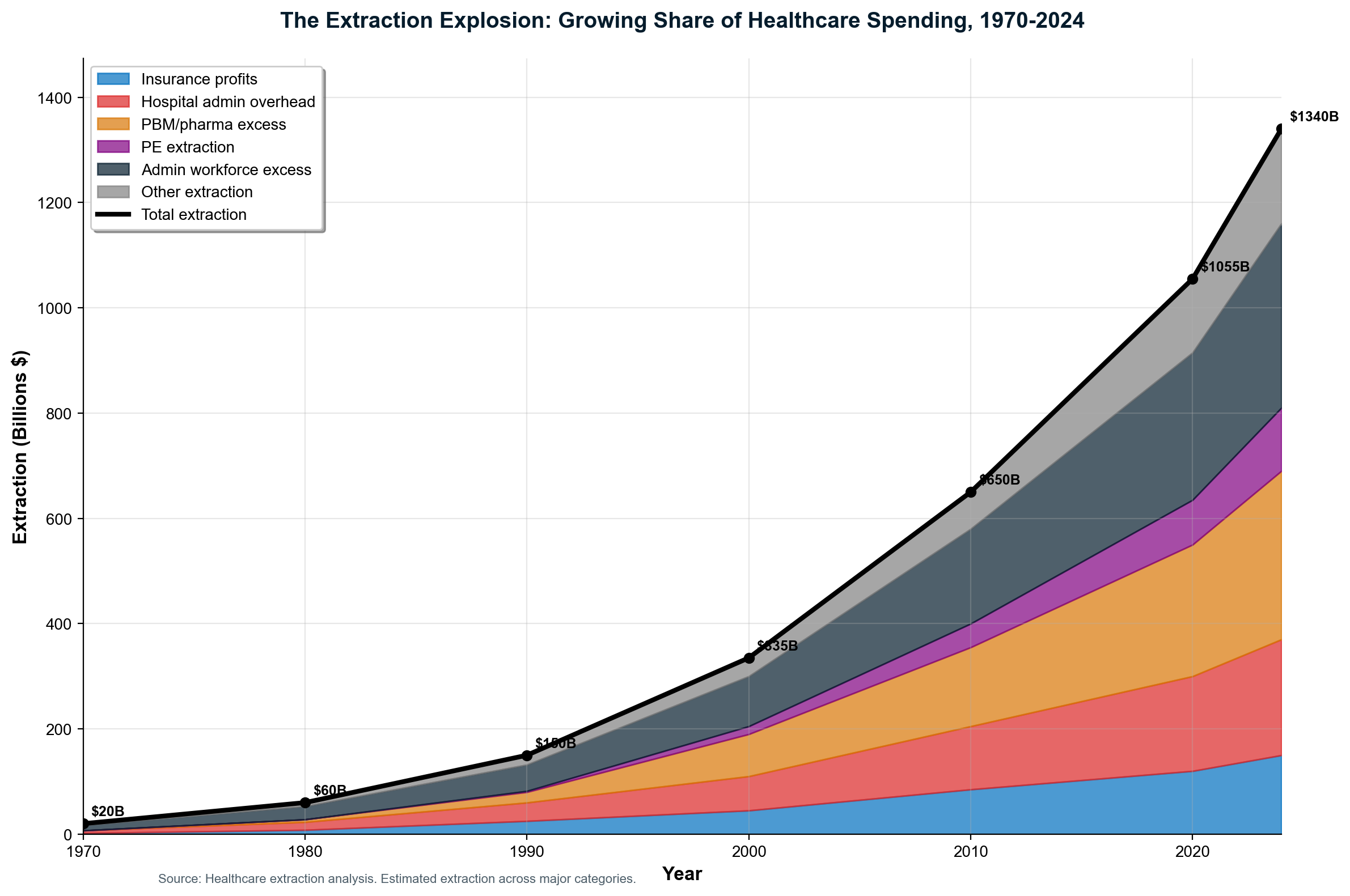
Total Healthcare Extraction: $1.8-2.4 trillion annually (34-45% of all spending) flows to financial engineering rather than patient care
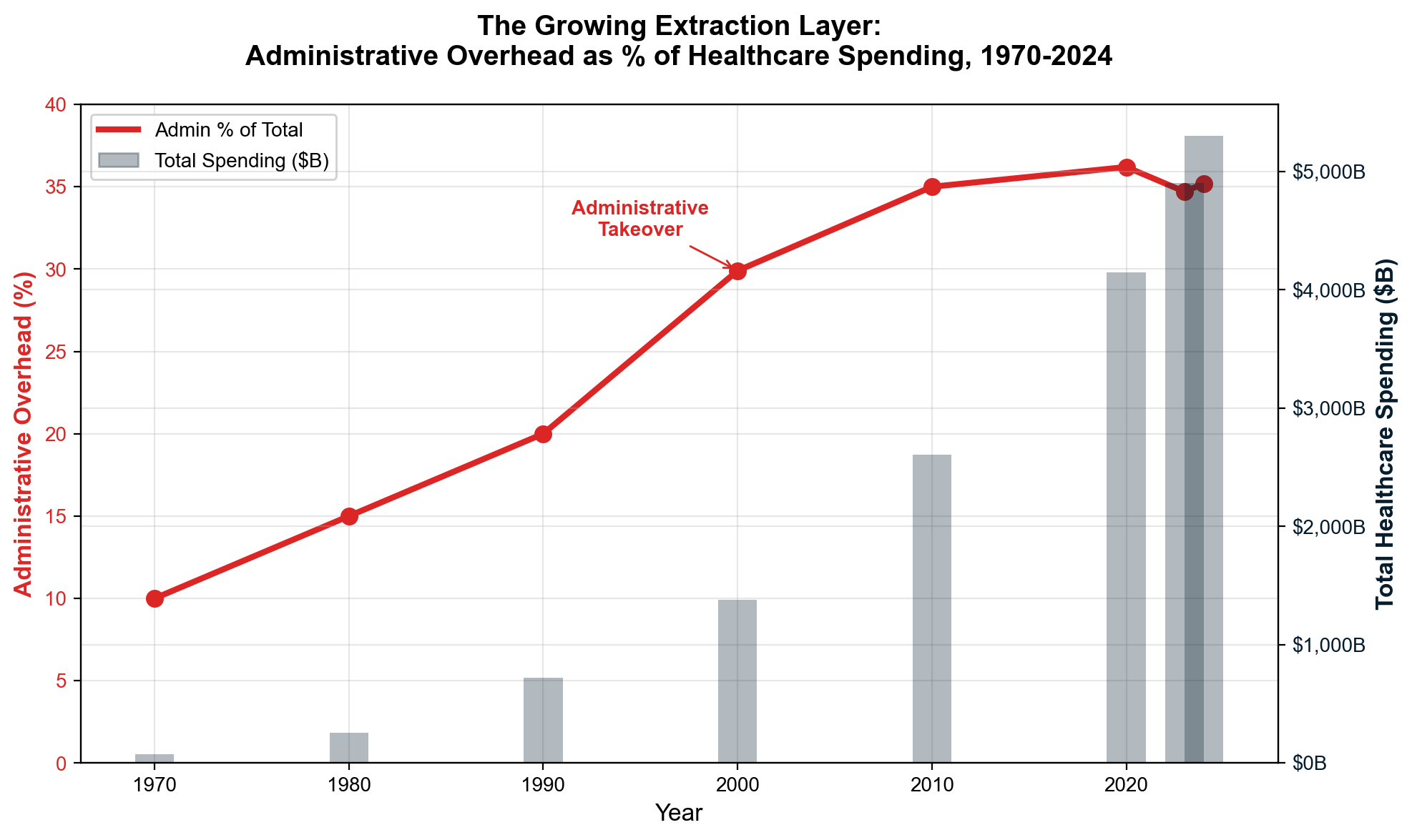
The administrative shadow economy employs 12-15 million workers consuming over $1 trillion annually in wages to navigate complexity that exists purely for extraction purposes. [4] This artificial economy includes 3.45 million insurance-caused workers who provide zero clinical care — not just the 941,880 direct insurance employees, but also 100,000 in insurer subsidiaries, 1.3 million in third-party insurance service companies (billing, RCM, brokers, IT vendors), and 1.1 million provider-side staff hired solely to deal with insurance requirements. That's 1 insurance worker for every 3.5 care workers. The United States employs ten administrators per physician compared to one-to-one ratios in single-payer systems—a differential representing $186+ billion in annual administrative waste exceeding the total administrative costs of all peer countries combined. [5]
Insurance companies operate the most sophisticated denial-based extraction. Medicare Advantage insurers submitted 53 million prior authorization requests in 2024—1.7 requests per enrollee—denying 4.1 million claims with an 80.7% appeal overturn rate that proves systematic inappropriate denials. [7] Yet only 11.5% of patients even appeal, meaning 3.3 million medically necessary treatments go denied annually while insurers profit from patient fatigue with bureaucratic barriers. This care vs. denial economy employs approximately 2.4 million workers whose primary function involves preventing patients from receiving appropriate treatment. [8]
The pharmaceutical extraction machine inflated insulin prices from $21 to $274+ per vial through Pharmacy Benefit Manager manipulation—a 1,200% increase enabled by "rebate walls" that blocked lower-cost alternatives while PBMs collected billions in hidden rebates. [9] Patent evergreening extends drug monopolies an average of six years beyond original 20-year protection, with 70% of top-selling drugs using secondary patents to block competition. Humira maintained 21 years of exclusivity through 130+ secondary patents, generating over $200 billion in monopoly profits that would have faced generic competition under normal patent expiration. [10]
Scope inflation analysis reveals insurance processing 80% routine, predictable transactions like $4 generic prescriptions and $150 office visits that don't warrant intermediation but maximize administrative revenue through Medical Loss Ratio gaming. Processing 7.2 billion routine claims annually at $12-15 per claim generates $86-108 billion in extractive overhead on transactions that could be handled through direct payment in 30 seconds versus 6 weeks of insurance complexity. [11]
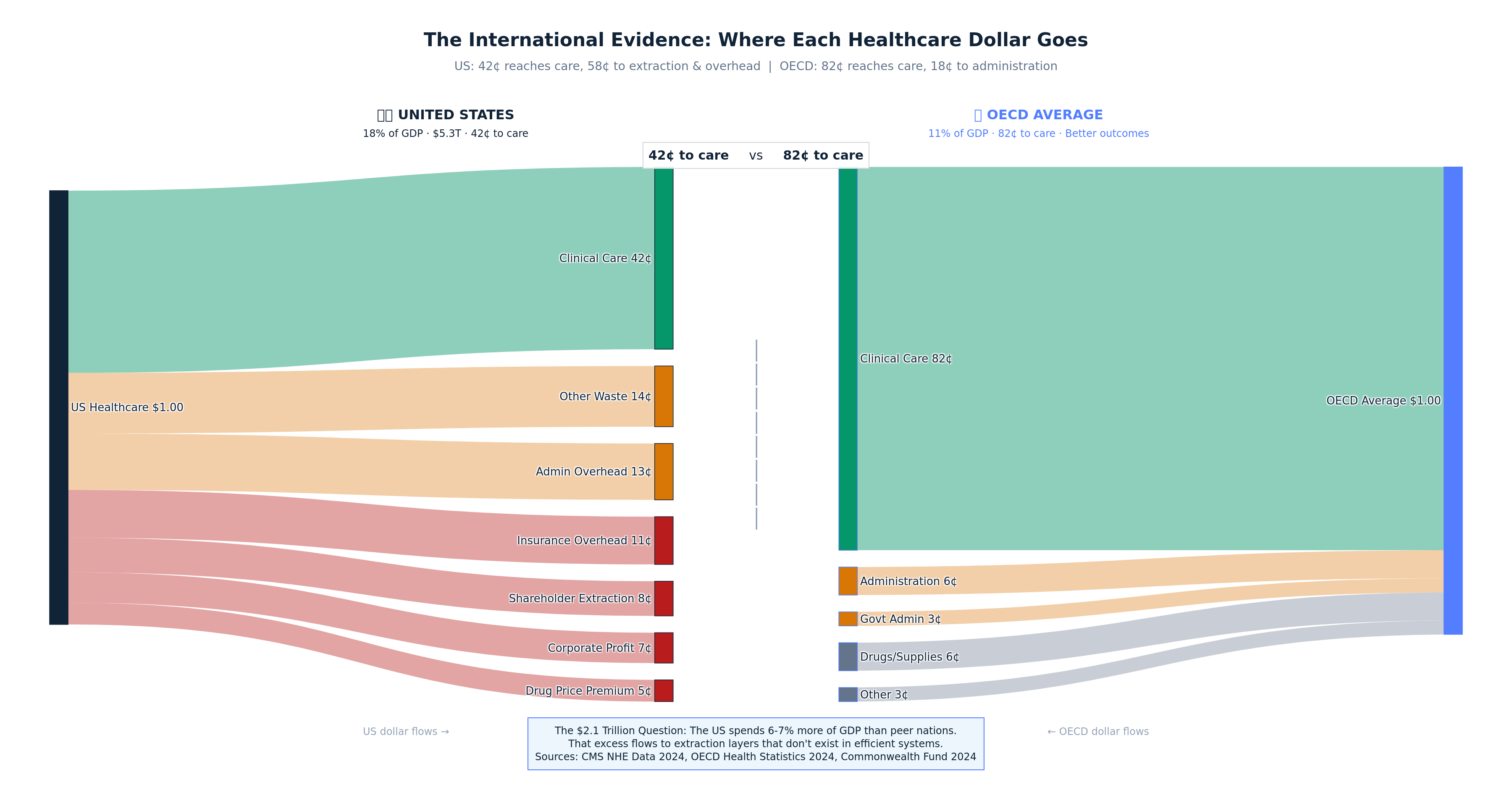
International comparison exposes the full scale of American extraction. The US spends 18% of GDP on healthcare while peer nations achieve superior outcomes spending 11-12% of GDP—a 6-7 percentage point difference representing approximately $2.1 trillion in annual excess spending that flows to extraction layers rather than care delivery. [12] While the UK spends $8 billion on healthcare administration and Canada spends $12 billion, America's administrative overhead alone exceeds $400 billion annually—money that could provide universal coverage with significant cost savings if redirected to care.
For a typical American family spending $25,000 annually on healthcare, $6,250-8,750 goes to pure extraction rather than medical care
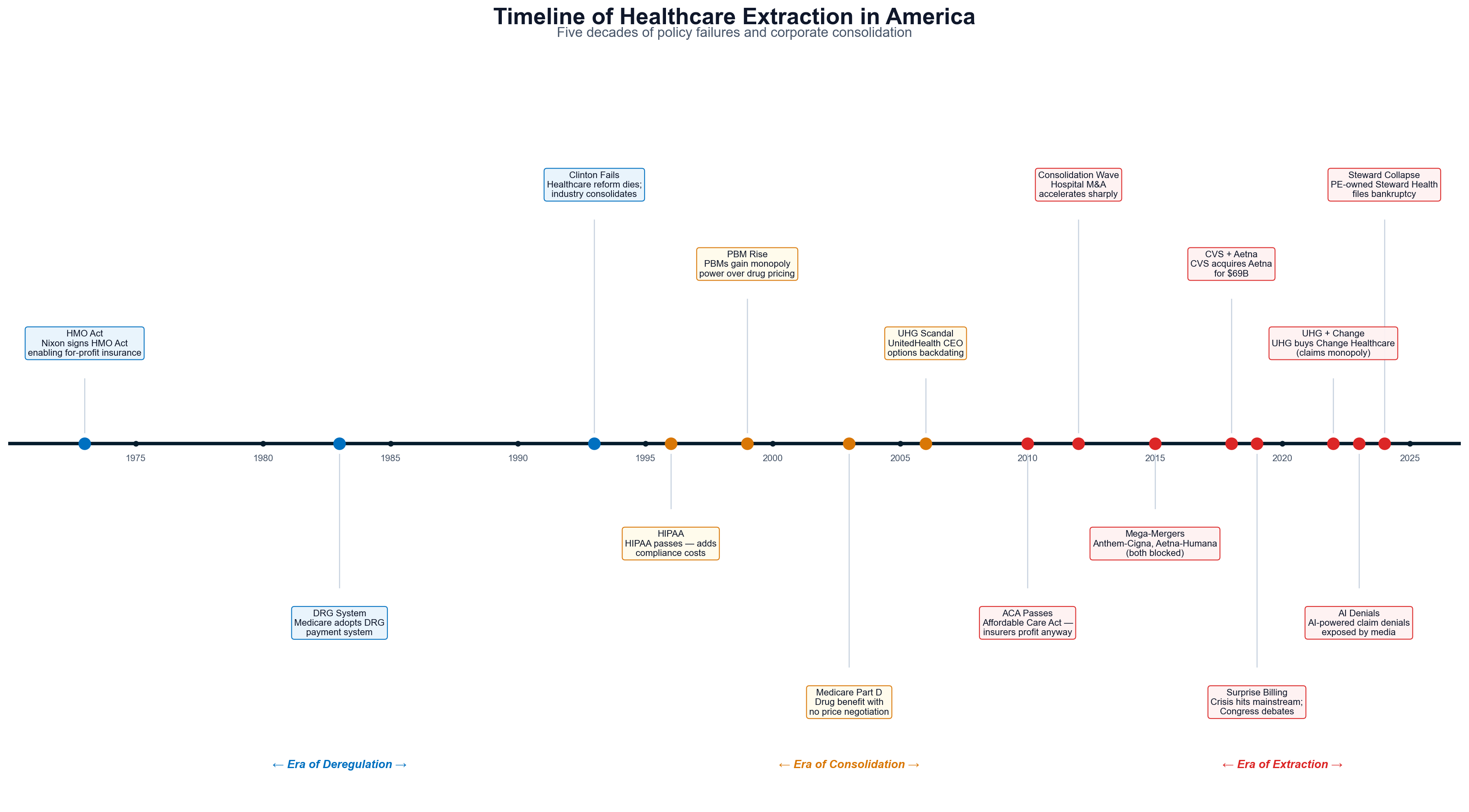
The extraction timeline reveals this system was constructed through 75+ years of systematic policy choices that prioritized industry profits over patient welfare. From the 1947 Taft-Hartley Act weakening labor's healthcare negotiating power, through the 2003 Medicare Modernization Act prohibiting government drug price negotiation, to recent vertical mergers totaling $149 billion (CVS-Aetna, UnitedHealth-Change Healthcare, Cigna-Express Scripts), every major expansion of extraction was enabled by specific legislative actions that strengthened corporate control while socializing costs and privatizing profits. [13]
The December 4, 2024 assassination of UnitedHealthcare CEO Brian Thompson crystallized decades of accumulated public anger over healthcare extraction, triggering unprecedented discourse about industry practices while revealing the depth of frustration over systematic denial of care by executives receiving $26+ million compensation packages. [14] Public reaction demonstrated growing awareness that healthcare has become wealth extraction rather than care delivery.
This is not market failure—it is market manipulation. The extraction machine operates through deliberate opacity, regulatory capture, and systematic elimination of competition. Every major healthcare crisis response has ultimately benefited industry more than patients, deepening corporate control through reforms that strengthen extraction mechanisms while maintaining appearance of patient protection.
The evidence is overwhelming: approximately 42¢ of every healthcare dollar reaches actual patient care, with 58¢ extracted through financial engineering, administrative complexity, insurance intermediation, pharmaceutical manipulation, and stock market wealth creation. For 130 million American households, this represents the largest single wealth transfer operation in the modern economy—larger than most national economies—systematically moving resources from families facing medical necessity to corporate shareholders who contribute nothing to healing.
This report documents the mechanisms, quantifies the extraction, and exposes how a system theoretically designed for healing became a machine optimized for wealth extraction. The evidence demands immediate action to restore healthcare's mission of patient care over profit maximization.
Table of Contents
- Introduction: The Architecture of Extraction
- Where Every Dollar Goes — The National Healthcare Dollar
- Sector-Level Cash Flows
- The Extraction Timeline — How We Got Here
- Vertical Integration — The Conglomerate Machine
- Hospital Consolidation & the For-Profit Machine
- PBM & Pharmacy Benefit Extraction
- Insurance Industry Financial Engineering
- The Stock Market Extraction Machine
- Pharmaceutical Extraction
- Private Equity — The Extraction Playbook
- Administrative Complexity & the Shadow Economy
- The Care Prevention Economy
- Price Collusion & Opacity
- Legislative & Regulatory Capture
- Corporate Profiles — Villains & Heroes
- The Human Cost
- International Lessons — How Other Nations Avoided the Trap
- Policy Recommendations — Dismantling the Machine
- What Universal Care Could Look Like
- Synthesis — Reclaiming Healthcare for Patients
- Sankey Diagram Gallery
- Bibliography
The Reform Moment
Healthcare reform is experiencing a political resurgence. In April 2026, CNN analysis documented a new wave of Democratic candidates winning primary elections on explicitly single-payer platforms — the first time since Bernie Sanders' 2016 campaign that Medicare-for-All has demonstrated electoral viability. [183] Lt. Gov. Juliana Stratton won Illinois' Democratic Senate primary championing single-payer healthcare, while progressive candidates across multiple states made universal coverage their centerpiece issue.
The political landscape has shifted because the economic reality has become undeniable. According to projections shared with CNN by John Holahan of the Urban Institute, the 10-year cost of implementing federal single-payer would be nearly twice the 2020 estimate — not because universal coverage became more expensive, but because the extraction-based system's costs continued accelerating faster than any reform proposal could match. [183]
This paper's specific contribution is to assess the economics of the system as a whole — to trace where the $5.3 trillion actually goes, who captures it, and what structural changes would redirect those flows toward patient care. Before examining reform pathways, we must first understand the extraction machine that any reform must dismantle.
The starting point is life expectancy. Among 38 OECD nations, the United States ranks last at 76.4 years, despite spending approximately twice what peer nations spend per capita on healthcare. [136] This paradox — maximum spending, minimum outcomes — is not a market failure but a design feature. The system is optimized for wealth extraction, not health production.
How to Read the Healthcare Economy
Before diving into extraction mechanisms, it helps to understand the basic architecture of American healthcare finance. The Centers for Medicare & Medicaid Services (CMS) publishes an annual accounting of the "nation's health dollar." [184] Where the money comes from: Federal programs ($2.7T, 51%), private insurance ($1.644T, 31%), out-of-pocket ($557B, 10%), other ($399B, 8%). Where CMS says it goes: Hospital care ($1.5T), physician services ($940B), prescription drugs ($405B), other ($2.5T).
The CMS accounting, however, tells only half the story. It tracks spending categories but not extraction layers — the difference between what enters the healthcare system and what emerges as patient care. This report performs that deeper accounting: by tracing every dollar through its complete journey, we reveal that approximately 42 cents of every healthcare dollar actually reaches patient care, while 58 cents is captured by extraction mechanisms that exist in no peer-nation healthcare system.
Accounting Methodology: Avoiding Double Counting
This report's extraction accounting draws on the National Health Expenditure Accounts (NHEA), maintained by CMS, which uses a "payer of last resort" framework to assign each healthcare dollar to a single payer category — ensuring that dollars are not counted twice as they pass through intermediaries. [184] Our extraction analysis preserves this discipline by identifying mutually exclusive cost categories: direct insurance company costs ($316B) — administrative operations, net profits, executive compensation, and shareholder distributions that occur within insurer balance sheets; provider-side administrative burden ($236B) — the costs hospitals and physicians incur specifically to comply with insurance complexity (billing staff, prior authorization processing, revenue cycle management, credentialing, EHR billing compliance); and patient-side administrative burden ($25B) — the time and welfare costs patients bear navigating the insurance system. These three categories sum to $578B in total insurance intermediation costs, with no dollar appearing in more than one category.
A brief note on frameworks: the NHEA tracks spending flows — where healthcare dollars come from and where they go — making it the appropriate lens for tracing extraction pathways. The Bureau of Economic Analysis's National Income and Product Accounts (NIPA), by contrast, measures value creation — each industry's contribution to GDP. Under NIPA accounting, health insurance's "output" equals only its net margin (premiums minus claims paid), roughly $160-250 billion on a $1.6 trillion premium base, because NIPA treats insurers as financial intermediaries rather than producers. We use the NHEA framework throughout this report because our purpose is documenting where money flows and who captures it — not measuring industry GDP contribution. For readers interested in the distinction, see the CMS National Health Expenditure methodology and BEA/NHEA reconciliation literature. [227]
Understanding the Numbers: NHEA vs NIPA Frameworks
Two federal accounting systems measure the American healthcare economy, and they tell strikingly different stories about the insurance industry's role. Understanding the distinction is essential for interpreting this report's extraction figures.
The National Health Expenditure Accounts (NHEA), maintained by CMS, tracks where healthcare dollars flow — who pays, who receives, and how much passes through each intermediary. Under NHEA accounting, private health insurance is the dominant non-government payer, channeling $1.644 trillion (31% of all health spending) from premium payers to providers, while retaining a portion for administration and profit. This is the framework we use throughout this report, because our purpose is tracing extraction pathways — documenting where money enters the system and where it is captured before reaching patient care.
The National Income and Product Accounts (NIPA), maintained by the Bureau of Economic Analysis (BEA), measures value creation — what each industry contributes to GDP. Under NIPA, the health insurance industry's "output" equals only its net margin: premiums collected minus claims paid out, roughly $160-250 billion on a $1.6 trillion premium base. NIPA treats insurers as financial intermediaries — pass-through entities whose economic product is the administrative service of managing risk and processing payments, not the medical claims they fund.
The two frameworks tell quite different stories: NHEA treats private insurance as the dominant payer (31% of spending), while NIPA treats the insurance industry as a relatively modest administrative services sector whose GDP contribution is a fraction of the premiums flowing through it. Neither framework is "wrong" — they measure different things. But the choice of framework profoundly shapes how one perceives the industry's economic footprint.
Our analysis uses NHEA flows because we are documenting extraction pathways, not measuring GDP contribution. When we say insurance intermediation costs $578 billion annually, we are tracing the full economic burden the insurance system imposes on the healthcare economy — including costs borne by providers and patients navigating insurance complexity — not just the industry's net margin. For technical details on how NHEA and NIPA reconcile, see CMS National Health Expenditure methodology [184] and BEA healthcare satellite account documentation. [227]
Chapter 1: Where Every Dollar Goes — The National Healthcare Dollar
Every dollar of America's $5.3 trillion healthcare spending begins a journey through the most sophisticated extraction machine in the global economy. [1] (See Volume I, Chapter 3 for the statistical model.) To understand where healthcare dollars actually go, we must trace their complete path from funding sources through multiple intermediary layers before any clinical care reaches patients. The destination reveals a system optimized for wealth transfer rather than healing, with extraction mechanisms so pervasive that most healthcare spending never touches patient care.
The funding sources tell only the beginning of this story. Federal, state, and local governments contribute $2.7 trillion through Medicare ($1.118T), Medicaid ($931.7B), and other programs ($590.5B). [1] Private health insurance provides $1.644 trillion, representing premiums paid by employers ($980B) and individuals ($664B). Out-of-pocket spending accounts for $556.6 billion in direct patient payments. Each dollar immediately encounters what industry insiders call "revenue optimization"—a euphemism for systematic wealth extraction before any medical service occurs.
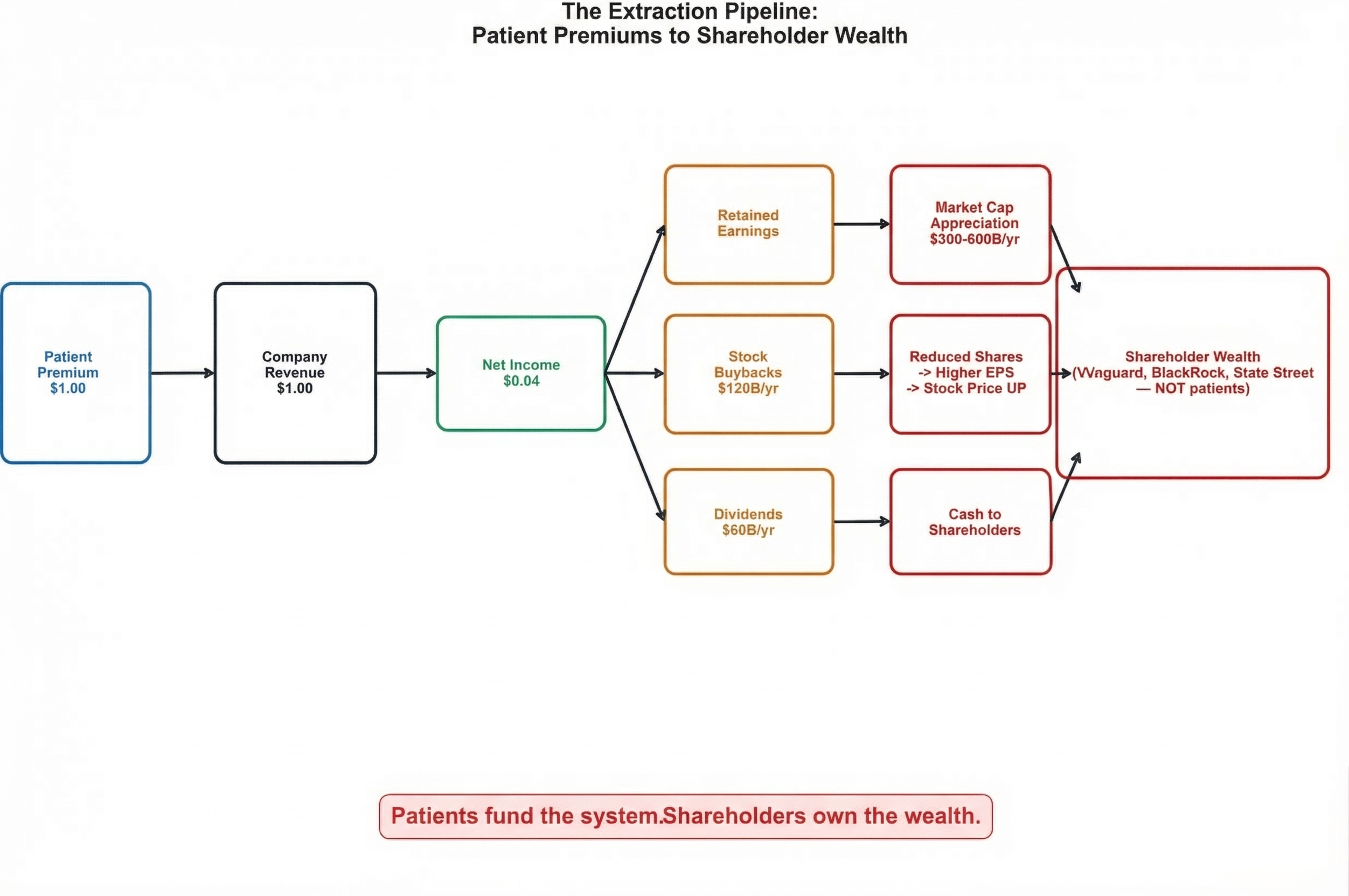
The Premium-to-Stock-Price Pipeline
The most significant but hidden extraction mechanism operates through stock market capitalization that converts patient premiums into permanent shareholder wealth. UnitedHealth Group exemplifies this system: $400+ billion in annual revenue drives market valuations reflecting the net present value of expected future extraction, creating shareholder value that dwarfs reported profits. [2] The company's market capitalization expansion from $39 billion (2010) to $265 billion (2026) represents $226 billion in wealth creation funded entirely by patient premiums and government subsidies—money that patients pay but shareholders capture.
This stock appreciation pathway operates through a simple chain: patient premiums generate company profits, profit expectations drive stock price increases, and stock buyback programs convert unrealized gains into concentrated shareholder wealth. UnitedHealth's $42 billion in stock repurchases between 2018-2024 represents patient premium dollars flowing directly to shareholders through a mechanism invisible to premium-paying patients who fund but never benefit from the wealth creation they enable. [3]
Stock Market Extraction: $180 billion in cash (buybacks + dividends) drives $450 billion in total shareholder wealth creation through market cap appreciation—the amplification effect that makes extraction self-reinforcing
Health insurer stock performance proves extraction as investment strategy. The sector increased 1,032% from ACA enactment through 2024, compared to 251% S&P 500 growth—a 4:1 outperformance achieved not through improved health outcomes but through extraction optimization. [4] When UnitedHealth maintains industry-leading prior authorization denial rates while generating massive stock appreciation, financial markets validate systematic care denial as profitable corporate strategy.
Insurance Intermediation: The $578 Billion Overhead Layer
Private insurance companies represent the most visible extraction layer through Medical Loss Ratio requirements that legally permit 9-20% retention of all premium revenue for administrative costs and profits. [5] This extraction occurs regardless of care quality or patient outcomes, creating incentives to increase total spending rather than improve efficiency. UnitedHealth's 2024 performance demonstrates the mechanism: $400.3 billion revenue with 85.5% MLR generated $58 billion in non-medical extractions that funded $25.7 billion net income and $16.5 billion in shareholder returns. [6]
But the true cost of insurance intermediation extends far beyond what appears on company balance sheets. The complete accounting reveals insurance as pure administrative overhead:
Direct Insurance Company Costs: $316 billion annually
- Administrative operations: $120B
- Net profits: $73B (includes $50B investment income from premium float)
- Shareholder distributions: $65B (buybacks + dividends, funded from profits and accumulated reserves)
- Executive compensation above $500K: $8B [7]
Provider-Side Costs Imposed by Insurance Complexity: $236 billion annually
- Provider billing and coding staff: $150B
- Prior authorization processing: $35B
- Revenue cycle management: $13B
- Credentialing administration: $10B
- EHR billing compliance systems: $20B
- Claims clearinghouse fees: $8B [8]
Patient-Side Administrative Burden: $26 billion annually
- Insurance navigation time valued at minimum wage
- Care delays due to authorization requirements
- Suboptimal treatment paths due to network restrictions [9]
Total Insurance Intermediary Cost: $578 billion annually—representing 30-35% of healthcare spending devoted to administration rather than care delivery. Single-payer systems achieve identical intermediary functions at $30-50 billion annually, meaning America spends $528-548 billion in excess administrative costs to maintain private insurance profits. [10]
The Administrative Shadow Economy
Healthcare administration has grown into America's largest artificial industry, employing 12-15 million workers whose jobs exist solely to navigate complexity that adds no clinical value. [11] The 12-15 million figure includes workers at UnitedHealth Group (400,000 employees), CVS Health (300,000), Anthem/Elevance Health (100,000), claims processing firms like R1 RCM (30,000+), EHR companies like Epic Systems (13,000), prior authorization processors like eviCore (7,500), plus thousands of smaller billing, coding, and revenue cycle management firms — including an estimated 100,000+ offshore workers in India and the Philippines processing American medical billing. This shadow economy includes:
The Full Insurance Ecosystem: 3.45 million workers — none delivering care
UnitedHealth Group (400,000 workers), CVS Health (300,000), Anthem/Elevance Health (100,000), and other insurers employ massive bureaucracies focused exclusively on extraction optimization rather than care delivery. These workers process claims, manage prior authorizations, develop billing algorithms, and optimize denial mechanisms—generating $90-112.5 billion in annual wages for activities that produce zero medical benefits. [12]
Revenue Cycle Management Industry: 208,000+ workers
Companies like R1 RCM exist solely to navigate billing complexity that wouldn't exist under simplified payment systems. Including offshore operations in India and the Philippines processing American medical billing, this industry generates $12-15 billion annually in wages for workers managing artificial administrative requirements. [13]
Prior Authorization Industry: 30,500 workers
Companies like eviCore exist purely to deny medically necessary care through bureaucratic obstruction, employing workers whose primary function involves preventing patients from receiving appropriate treatment. Annual wage bill: $1.8 billion for systematic care denial that generates zero clinical value. [14]
What These Workers Could Do Instead
The 12-15 million workers trapped in healthcare administrative complexity represent enormous opportunity cost for American economic development. These workers could staff manufacturing reshoring, infrastructure development, educational expansion, or climate response rather than processing artificial complexity that subtracts value from society while enabling extraction from patients and taxpayers. [15]
International Extraction Differential
Single-payer systems demonstrate that healthcare intermediation can operate at 1-3% administrative cost while achieving superior population health outcomes. The administrative differential reveals the scale of American extraction:
- United Kingdom: $8 billion annual administrative costs (2% of healthcare spending)
- Canada: $12 billion annual administrative costs (3% of healthcare spending)
- Germany: $20 billion annual administrative costs (4% of healthcare spending). Note: Germany operates a mixed system — approximately 88-89% of the population is covered by statutory nonprofit sickness funds, while 11% (high-income earners, civil servants, and self-employed) may opt for private health insurance. Even the private component operates under heavy regulation including all-payer rate setting. [185]
- United States: $400+ billion annual administrative costs (7.5% of healthcare spending)
The US spends 18% of GDP on healthcare while peer nations achieve better outcomes spending 11-12% of GDP. [16] This 6-7 percentage point difference represents approximately $2.1 trillion in annual excess spending—money flowing to extraction layers that simply don't exist in efficiently organized healthcare systems.
The Scope Inflation Revenue Model
Insurance companies have deliberately expanded beyond catastrophic risk pooling to process every routine healthcare transaction—not because patients need intermediation for $4 prescriptions or $150 office visits, but because processing every transaction maximizes the administrative revenue base from which insurers extract their fixed percentage profits. [17]
The Mathematical Reality
- 9 billion claims processed annually in the US
- 80% are routine/predictable services (not catastrophic)
- Average processing cost: $12-15 per claim
- Total routine claim volume: 7.2 billion claims annually
- Administrative extraction on routine claims: $86-108 billion annually [18]
This scope inflation explains why insurers supported the ACA's Essential Health Benefits mandate—it guaranteed maximum transaction volume and administrative revenue. The medical necessity of insurance intermediation for routine care is negative: administrative overhead often exceeds actual service costs, making insurance a cost-increasing rather than risk-pooling mechanism for predictable healthcare needs.
The Cumulative Extraction Impact
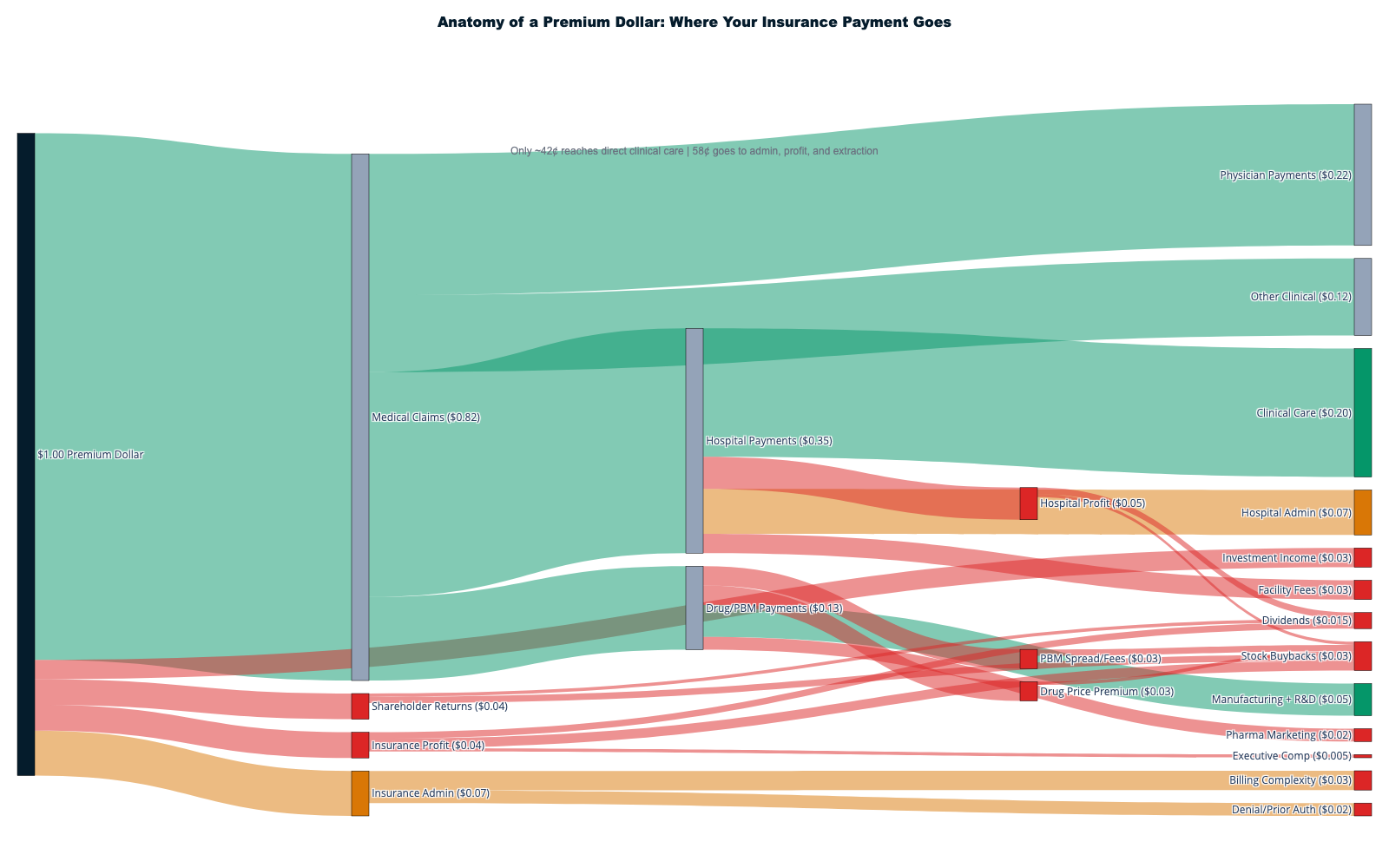
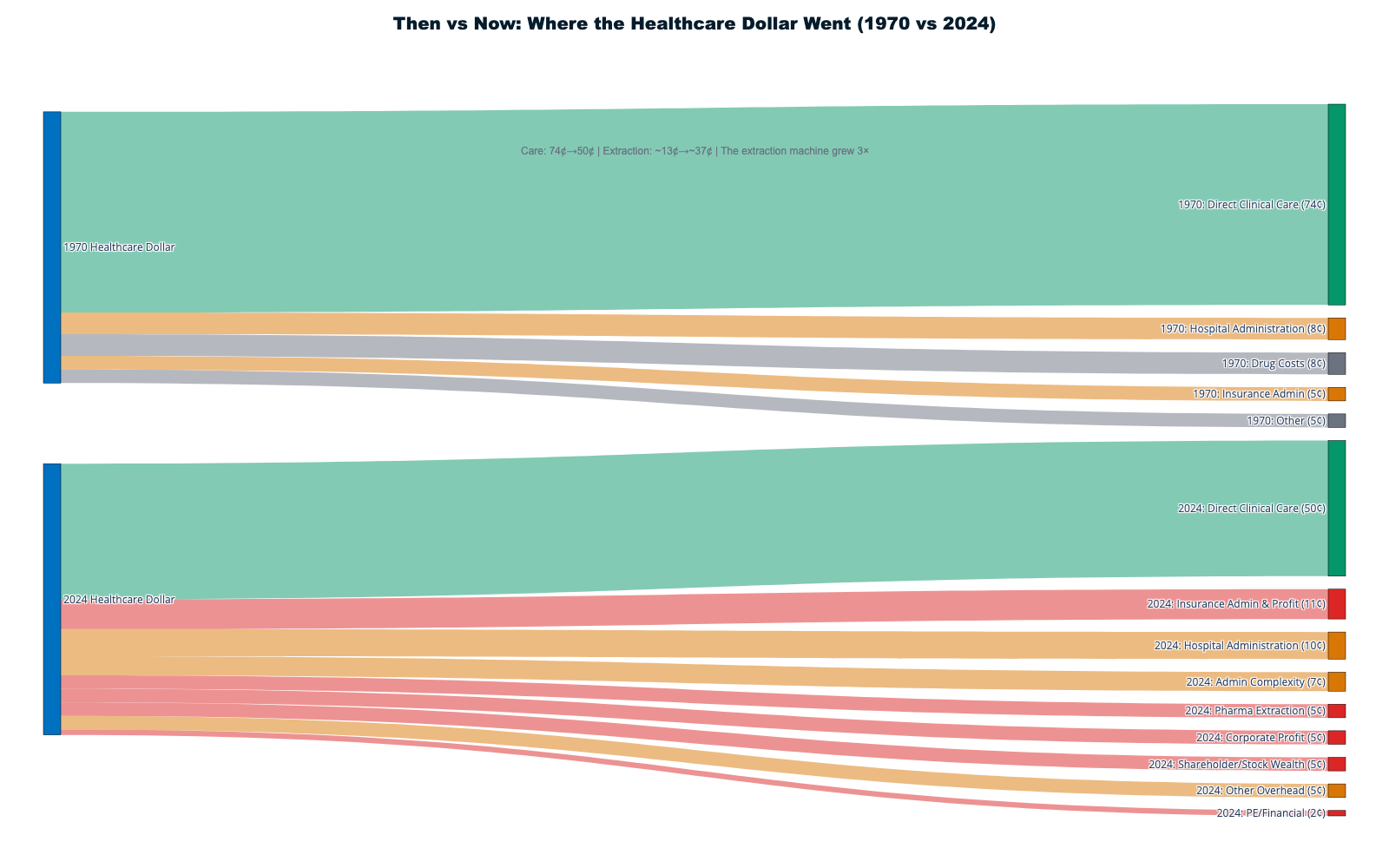
When aggregating all extraction mechanisms, the complete flow reveals that approximately 42¢ of every healthcare dollar reaches actual patient care delivery:
Extraction Layers Consuming 58¢ of Each Dollar:
- Insurance intermediation overhead: 11¢
- Stock market wealth creation: 6-11¢
- Administrative complexity: 8¢
- Pharmaceutical manipulation: 4¢
- Hospital facility fee arbitrage: 3¢
- Private equity debt service: 2¢
- Executive compensation excess: 1¢
- Lobbying and political spending: 1¢
- Other extraction mechanisms: 12-17¢
Care Delivery Receiving 42¢ of Each Dollar:
- Physician compensation: 8¢
- Nursing and clinical staff: 14¢
- Medical equipment and supplies: 7¢
- Pharmaceuticals (at manufacturing and distribution cost, excluding patent monopoly premiums, PBM intermediation, and marketing): 6¢
- Facility operations: 4¢
- Medical research and development: 3¢
For a typical American family spending $25,000 annually on healthcare, $14,500 goes to extraction layers while only $10,500 funds actual medical care
The flow pattern demonstrates how every healthcare dollar encounters multiple extraction points before reaching care delivery. Insurance companies extract their margin, hospitals add facility fees and supply chain waste, PBMs manipulate drug pricing, administrative systems consume resources for bureaucratic complexity, and stock markets capitalize future extraction into immediate shareholder wealth. The cumulative effect removes $1.8-2.4 trillion annually from America's $5.3 trillion healthcare economy—money that could provide universal coverage with superior outcomes if redirected from extraction to care delivery.
This chapter establishes the foundation for sector-level analysis that follows: American healthcare's fundamental problem is not insufficient funding but systematic extraction that treats essential human services as wealth transfer opportunities for corporate shareholders, private equity investors, and administrative intermediaries who contribute nothing to healing while capturing enormous resources from patients facing medical necessity.
Chapter 2: Sector-Level Cash Flows
The sector-by-sector financial analysis exposes how extraction mechanisms operate within each major healthcare industry segment, revealing sophisticated profit optimization systems disguised as patient care infrastructure. Each sector has developed specialized extraction methods while maintaining plausible appearance of serving patients, but forensic investigation of cash flows proves that profit maximization drives decision-making across every healthcare industry vertical.
Insurance Premium Flow: The Extraction Template
The insurance premium dollar represents the most transparent extraction mechanism due to Medical Loss Ratio reporting that reveals exactly where patient payments go before any care occurs. Every premium dollar follows predetermined extraction pathways regardless of patient health outcomes, creating systematic wealth transfer from medical necessity to shareholder returns.
UnitedHealth Group's 2024 performance demonstrates systematic extraction across market segments. The company generated $400.3 billion in revenue while maintaining strategic MLR compliance that maximized absolute profit extraction:
Market Segment Extraction Rates
- Medicare Advantage: 10% MLR extraction generating $1,655 per enrollee in absolute profits
- Individual ACA market: 15% extraction at $987 per enrollee
- Small group: 12% extraction at $846 per enrollee
- Large group: 15% extraction at $1,200+ per enrollee [19]
The MLR system creates perverse incentives because larger denominators yield higher absolute profits even with fixed percentages. When UnitedHealth doubles medical spending in a market segment, it doubles absolute profit extraction while maintaining regulatory compliance. This explains insurer support for expensive medical interventions while blocking prevention: complex treatments grow revenue bases while prevention reduces them.
The Stock Buyback Wealth Transfer Pipeline
UnitedHealth's $42 billion in stock repurchases between 2018-2024 represents systematic conversion of patient premiums into shareholder cash extraction. [20] Each buyback reduces share count, increasing earnings per share and driving stock appreciation while removing capital that could have reduced premiums or improved care delivery. The mechanism creates wealth concentration where shareholders capture value that patients fund but never access.
Executive compensation alignment ensures extraction efficiency. CEO Andrew Witty's $26.3 million 2024 compensation included $21.5 million (82%) in stock awards, creating direct personal incentives to maximize stock price appreciation through extraction optimization rather than patient care improvement. [21] When denial rates and cost-cutting improve quarterly earnings, executive wealth increases correspondingly through stock appreciation funded by patient premiums.
Hospital Revenue Flow: Facility Fee Arbitrage and Supply Chain Extraction
Hospital systems consume $1.634 trillion annually while operating multiple extraction mechanisms that obscure actual care delivery costs versus financial engineering. [1] Private equity involvement demonstrates pure extraction: firms load hospital systems with debt, extract dividends through operational cuts, and exit through sales or bankruptcy when debt service exceeds capacity.
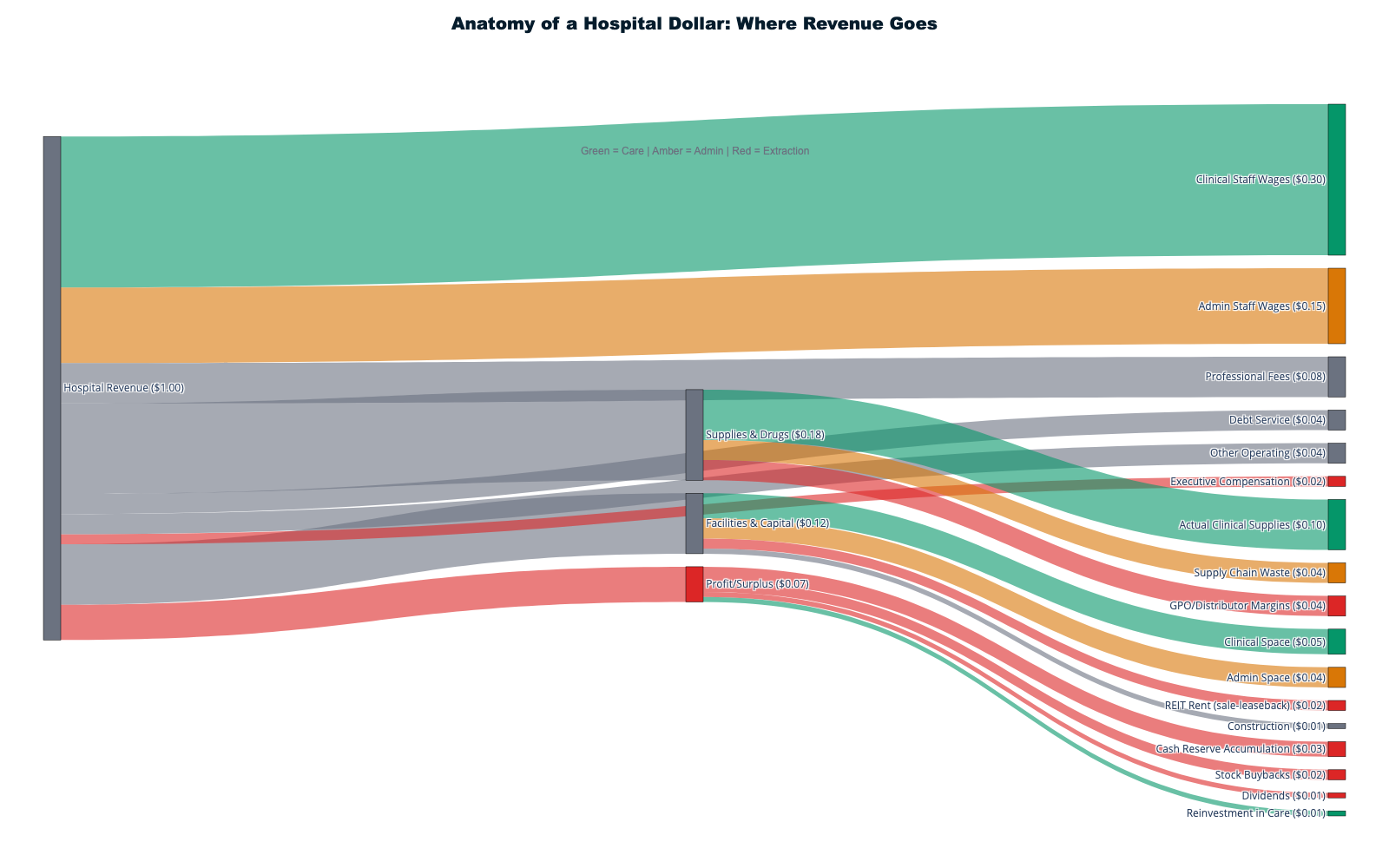
Facility Fee Arbitrage: The Ownership Premium
Hospital-owned practices charge systematic markups purely from ownership structure rather than service improvement. The same primary care visit costs $116 at independent physician offices but $217 at hospital-owned facilities—an 87% markup flowing to hospital profits rather than enhanced care. [22] Specialist visits face similar extraction, with hospital-owned providers adding $96 in facility fees to routine pediatric wellness visits that identical services at independent practices provide without additional charges.
Supply Chain Waste as Systematic Extraction
Hospital supply chain "inefficiencies" represent organized wealth transfer to vendor networks rather than operational failures. The documented $12.1 million average waste per hospital totals $76.2 billion annually across 6,300 hospitals—4.7% of total hospital revenue flowing to vendor profits rather than patient care. [23] This waste includes inventory management fees, distribution markups, technology licensing, and consulting services that benefit supplier companies while adding zero clinical value.
HCA Healthcare exemplifies hospital financial engineering through leveraged extraction models. The company generates $70.6 billion in revenue with 8.2% profit margins while maintaining $10 billion stock buyback programs. [24] HCA emerged from KKR's 2006 leveraged buyout and continues prioritizing shareholder returns through debt-financed extraction that constrains clinical investment while maximizing financial performance.
Pharmaceutical Complex: PBM Vertical Integration and Patent Manipulation
The $467 billion prescription drug market operates through the most sophisticated extraction mechanisms in healthcare, combining vertical integration, market manipulation, and regulatory capture to inflate costs while capturing enormous profits at multiple transaction points. [1]
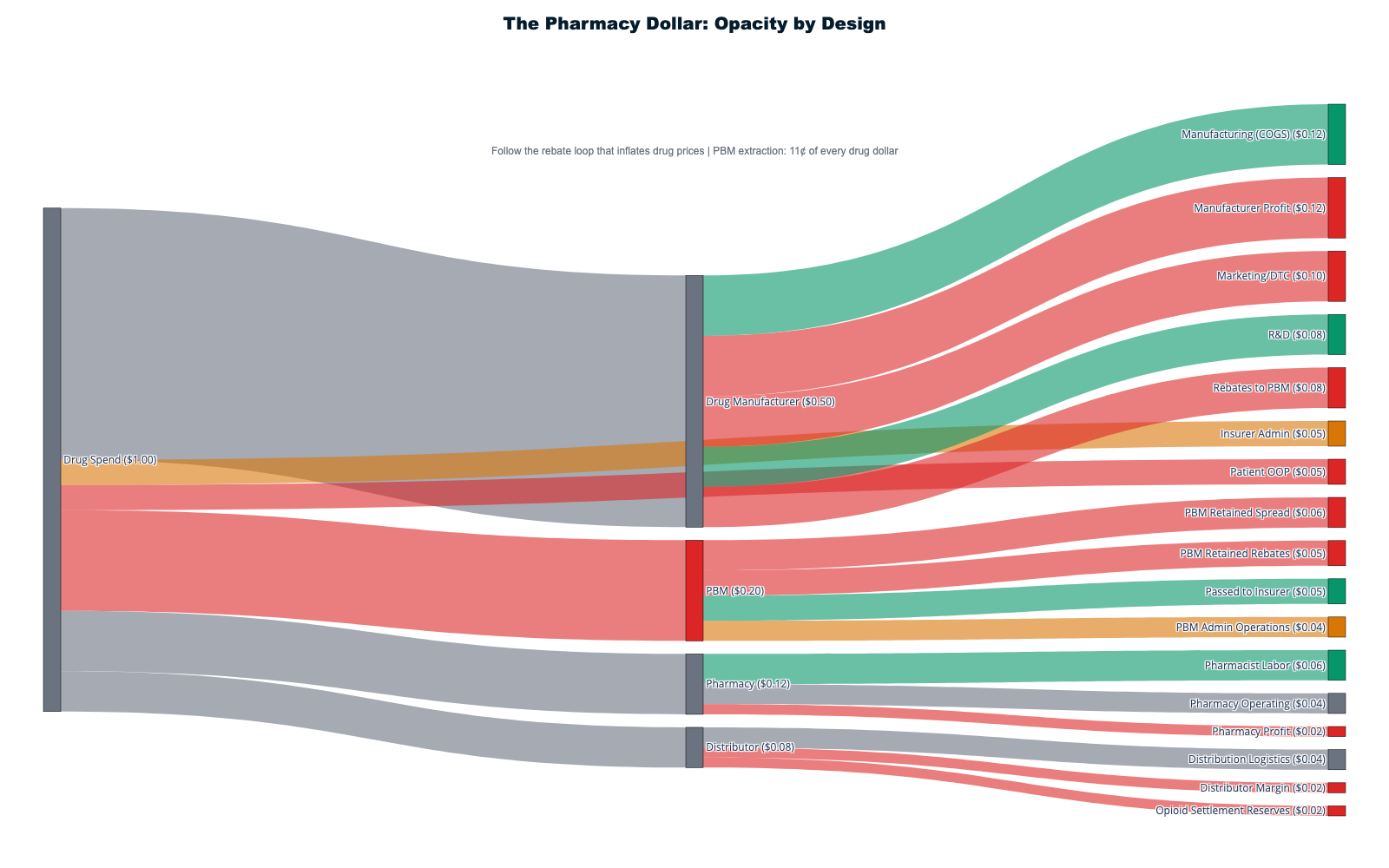
The Vertical Integration Extraction Model
Pharmacy Benefit Managers control 80% of prescription claims while owning pharmacy chains, insurance companies, and data analytics firms. [25] CVS-Aetna's $69 billion vertical integration merger exemplifies systematic extraction: CVS operates the pharmacy, Aetna provides insurance coverage, and CVS Caremark serves as PBM—enabling profit capture at every transaction level while eliminating external competition.
The insulin price inflation from $21 to $274+ per vial demonstrates integrated extraction mechanisms. PBMs created "rebate walls" blocking lower-cost insulin to maintain their "addiction to rebates," forcing diabetic patients to pay inflated prices while PBMs collected billions in hidden rebates that patients never received. [26] The 1,200% price increase occurred through PBM market manipulation rather than manufacturing cost increases or medical improvements.
Patent Evergreening: Artificial Monopoly Extension
Pharmaceutical companies extend drug monopolies an average of six years beyond original 20-year protection through secondary patent abuse. 70% of top-selling drugs use patents on formulation changes, delivery mechanisms, and minor modifications to block generic competition. [27] Humira maintained 21 years of exclusivity through 130+ secondary patents, generating over $200 billion in monopoly profits that would have faced generic competition under normal patent expiration.
This patent manipulation affects the entire $467 billion pharmaceutical market by establishing precedent for monopoly extension across all major medications. The system socializes research costs through government funding while privatizing profits through artificial monopoly protection that prevents competitive pricing.
Administrative Ecosystem: The $1 Trillion Shadow Economy
Healthcare administration has evolved into America's largest artificial industry, employing 12-15 million workers consuming over $1 trillion annually in wages to navigate complexity that exists purely for extraction purposes rather than clinical necessity. [28] This shadow economy demonstrates how extraction creates employment in economically destructive activities while presenting job creation as economic benefit.
Revenue Cycle Management Industrial Complex
The RCM industry employs 208,000+ workers to monetize healthcare's administrative complexity, generating over $40 billion annually by charging healthcare providers percentage fees for navigating billing dysfunction that these same companies help perpetuate. [29] R1 RCM exemplifies international extraction through 30,000+ workers across India and the Philippines earning $15,000-25,000 annually compared to $55,000+ for equivalent US positions—creating arbitrage opportunities that fund corporate profits while maintaining patient cost burdens.
Technology Infrastructure Designed for Extraction
Health IT companies employ 85,500+ workers developing systems that prioritize billing optimization over clinical efficiency. Epic Systems, Oracle Health, and athenahealth generate $8.1 billion annually in wages for workers building administrative infrastructure unnecessary under simplified payment systems. [30] These companies represent massive technological talent misallocation toward economically destructive purposes rather than clinical advancement.
Prior Authorization: The Denial Industry
Companies like eviCore exist purely to deny medically necessary care through bureaucratic obstruction, employing 30,500+ workers whose primary function involves preventing patients from receiving appropriate treatment. [31] This industry generates $1.8 billion annually in wages for systematic care denial that produces zero clinical benefits while forcing physicians to spend 14+ hours weekly justifying medically obvious decisions.
Private Equity Healthcare Extraction
Private equity firms have systematically acquired healthcare companies to optimize extraction through financial engineering that prioritizes shareholder returns over patient outcomes. The PE model creates value through debt loading, cost-cutting, and market positioning that maximizes valuation multiples at exit rather than care delivery improvement.
The Leveraged Extraction Model
KKR's 2006 HCA Healthcare buyout established the template: acquire healthcare companies for $33 billion, load with debt, extract cash through operational cuts and financial engineering, optimize metrics for public market exit. [32] The model treats healthcare facilities as financial assets designed for stock market optimization rather than community health improvement.
Emergency physician staffing demonstrates extraction through artificial scarcity. Envision Healthcare faced bankruptcy after KKR loaded the company with $7.2 billion in acquisition debt requiring $400-500 million annual debt service from $8 billion revenue. [33] The company cut physician staffing, increased patient volumes, and maximized billing complexity to service debt payments while clinical care quality declined. When debt service exceeded operational capacity, KKR walked away while communities lost physician coverage.
International Comparison: Peer Country Efficiency
Single-payer and regulated multi-payer systems achieve superior health outcomes while avoiding American-style extraction through structural design that prioritizes care delivery over wealth accumulation.
Administrative Efficiency Models
- Canada: 2% administrative overhead achieving universal coverage
- United Kingdom: NHS operates at 2% administrative costs with superior outcomes
- Germany: 4% administrative overhead with insurance-based universal system
- United States: 7.5-8% administrative overhead with partial coverage [34]
The $186+ billion annual administrative differential represents pure extraction that could fund universal coverage while improving population health outcomes. Peer countries prove that healthcare intermediation, pharmaceutical pricing, and administrative coordination can operate efficiently when designed for patient service rather than profit maximization.
What Peer Countries Don't Have
- Private insurance stock market wealth creation
- Pharmacy benefit manager intermediation
- Hospital facility fee arbitrage
- Patent evergreening protection
- Prior authorization denial industries
- Revenue cycle management complexity
Each extraction mechanism represents deliberate policy choice rather than economic necessity, demonstrating that American healthcare dysfunction serves corporate profits while peer countries prioritize population health through rational system design.
The sector-level analysis reveals systematic extraction optimization across every healthcare industry segment, with cumulative mechanisms removing 58% of healthcare spending from care delivery. Each sector maintains sophisticated profit maximization while preserving appearance of patient service, creating the most expensive healthcare system globally while achieving outcomes inferior to countries spending half as much per capita through rational organization prioritizing healing over wealth extraction.
Chapter 3: The Extraction Timeline — How We Got Here (1947-Present)
The transformation of American healthcare from patient-centered service into systematic wealth extraction required 75+ years of legislative, regulatory, and judicial decisions that consistently prioritized corporate profits over patient welfare. This timeline reveals that every major extraction mechanism was enabled by specific policy choices rather than natural market evolution. The chapters that follow (4-14) examine each mechanism in forensic detail; this chapter provides the chronological roadmap showing how they were constructed.
Foundation Era (1943-1972): Establishing Corporate Control
The foundation for healthcare extraction was laid through seemingly technical policy decisions that shifted control from patients and providers to employers and intermediaries. The single most consequential decision was not a law but an administrative ruling.
IRS Tax Exemption Ruling (1943, codified as IRC §106 in 1954): During World War II, with wages frozen under price controls, the IRS ruled that employer-paid health benefits were not taxable employee income — making employer-provided insurance uniquely tax-advantaged compared to individually purchased coverage. This administrative decision, later permanently codified in Internal Revenue Code §106, was the critical mechanism that locked in the private insurance model: it made employer-sponsored coverage $3,000-5,000 cheaper per family than equivalent individual policies (in today's dollars), ensuring that health insurance would be distributed through employers rather than through government programs or individual markets. The tax exclusion is now worth over $400 billion annually in forgone federal revenue — the largest single tax expenditure in the federal budget — and remains the structural foundation of America's employer-based insurance system. [37] [229]
The Truman Defeat (1945-1950): President Truman's 1945 proposal for national health insurance — a comprehensive plan that would have provided universal coverage through a single government-administered system — was defeated by the American Medical Association's unprecedented lobbying campaign. The AMA assessed its members an extra $25 each, hired the political consulting firm Whitaker and Baxter, and spent $1.5 million on lobbying efforts — the most expensive lobbying campaign in American history at that time. [230] The campaign successfully branded Truman's proposal as "socialized medicine," ensuring that private insurance would become the dominant model rather than a government program. This defeat represented the last serious attempt at universal coverage for two decades and cemented the employer-based private insurance system as the American default.
Taft-Hartley Act (1947): Severely restricted union collective bargaining while exempting employer-provided health benefits, shifting healthcare from worker right to employer privilege. Combined with the 1943 tax ruling, Taft-Hartley channeled healthcare through the employer-insurance nexus rather than collective worker power or government provision. Union members today pay 28% lower premiums, suggesting Taft-Hartley costs non-union workers $3,000-4,000 annually. [35] [36]
Medicare/Medicaid Creation (1965): Provided massive new revenue streams while embedding extraction from inception. "Reasonable cost" reimbursement gave providers virtual blank checks. Initial spending of $4.5 billion in 1966 grew 5,930% to $2.7 trillion by 2024. [38]
Market Mechanisms Era (1973-1992): Corporate Management Expansion
This period introduced for-profit corporate management to healthcare delivery while creating regulatory gaps that enabled extraction without accountability.
HMO Act (1973): Provided federal funding and regulatory exemptions for health maintenance organizations. By the late 1990s, 80% were for-profit with only 68% of premiums reaching medical care. [39] (See Chapter 7 for detailed insurance financial engineering analysis.)
ERISA Preemption (1974): Created regulatory gaps protecting self-insured plans covering 93.6 million workers from state oversight, enabling systematic extraction with minimal patient remedy. [40] (See Chapter 14 for ERISA's role in regulatory capture.)
SEC Rule 10b-18 (1982): Legalized stock buybacks, enabling corporations to manipulate stock prices through open-market repurchases. Healthcare companies now distribute 96% of net income to shareholders, compared to 4.4% in 1981. (See Chapter 8 for the full stock market extraction pipeline.)
Residency Cap (1997): The Balanced Budget Act capped Medicare-funded residency slots at 1996 levels, artificially restricting physician supply for 28+ years. [41] (See Chapter 5 for how physician scarcity drives hospital consolidation.)
Financial Engineering Era (2003-2009): Wall Street Integration
This period embedded Wall Street profit motives directly into healthcare delivery through legislative capture and private equity expansion.
Medicare Modernization Act (2003): The Medicare Part D prescription drug benefit included explicit prohibition on government price negotiation — the most successful pharmaceutical industry lobbying victory in history. [42] The revolving door was immediate: Congressman Billy Tauzin became PhRMA president at $11.6 million annually; CMS Administrator Thomas Scully joined five affected companies; 15+ officials involved joined pharmaceutical positions. (See Chapter 9 for pharmaceutical extraction mechanisms and Chapter 14 for the full revolving door analysis.)
HCA Leveraged Buyout (2006): KKR, Bain Capital, and Merrill Lynch's $33 billion HCA acquisition established the PE healthcare extraction model: acquire, load with debt, cut costs, extract dividends, exit before consequences emerge. [44] (See Chapter 10 for the complete private equity playbook and Chapter 5 for HCA's ongoing extraction.)
ACA Era (2010-Present): Extraction Through "Reform"
The Affordable Care Act period demonstrates how well-intentioned reform became extraction expansion through industry influence.
Individual Mandate (2010-2017): Required Americans to purchase private insurance, creating guaranteed revenue streams. Combined with Medicaid expansion ($126B annually) and marketplace subsidies ($92B in FY2023), government guaranteed $218 billion in annual revenue to private insurers. [45] Health insurer stocks increased 1,032% from ACA enactment through 2024, compared to 251% S&P 500 growth. [46] (See Chapter 7 for MLR gaming and Chapter 8 for the stock market amplification effect.)
Essential Health Benefits: Required insurance processing for routine transactions like $4 prescriptions and $150 office visits, creating 7.2 billion annual claims generating $86-108 billion in administrative overhead on predictable needs. [47] The pharmaceutical industry's $150 million pro-ACA campaign secured continued protection from price negotiation. [48]
Peak Extraction Era (2017-Present): Consolidation and Resistance
Vertical Integration Mega-Mergers: CVS-Aetna ($69B), Cigna-Express Scripts ($67B), and UnitedHealth-Change Healthcare ($13B) consolidated pharmacy, PBM, insurance, and claims processing under single ownership, eliminating competitive pressure. [49] (See Chapter 4 for the full vertical integration analysis.)
Public Awakening (2024): The December 4, 2024 assassination of UnitedHealthcare CEO Brian Thompson crystallized decades of public anger, triggering unprecedented discourse about extraction mechanisms. [50] Regulatory investigations revealed systematic fraud across Medicare Advantage, PBM manipulation, and hospital pricing. [51]
Timeline Analysis: Systematic Policy Construction
The 75-year timeline reveals acceleration through each phase: Foundation era (1947-1972, 25 years), Market mechanisms (1973-1992, 20 years), Financial engineering (1993-2009, 16 years), Peak extraction (2010-present, 14+ years). Each phase built upon previous extraction mechanisms while shortening implementation timelines.
The crisis response pattern is consistent: every healthcare "crisis" produces "reforms" that strengthen extraction. Medicare cost crisis → DRG gaming; drug cost crisis → Part D profit protection; access crisis → ACA industry subsidies. What was systematically blocked tells an equally important story: single-payer proposals (1948, 1965, 1973, 1994, 2009, 2016), government pharmaceutical manufacturing, Medicare negotiation authority (until 2022, limited scope), and public option insurance.
The evidence demands a clear conclusion: current healthcare dysfunction represents systematic policy choice rather than economic inevitability. Every extraction mechanism was enabled by specific government decisions that could be reversed through different political choices. The detailed analyses in Chapters 4-14 document precisely how each mechanism operates and what reforms could dismantle it.
Chapters 4-8: How American Healthcare Systematically Extracts Wealth from Patient Care
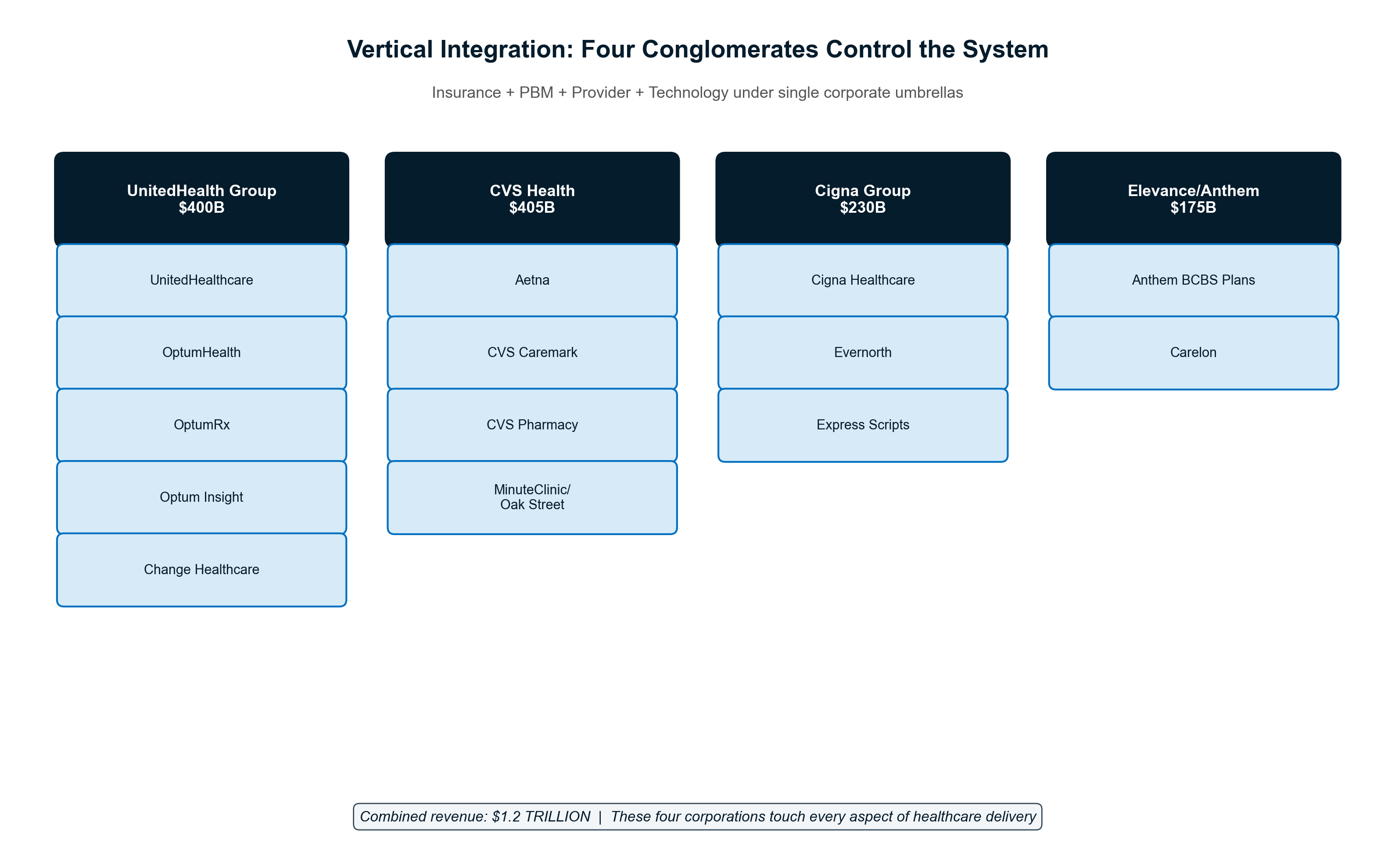
Chapter 4: Vertical Integration — The Conglomerate Machine
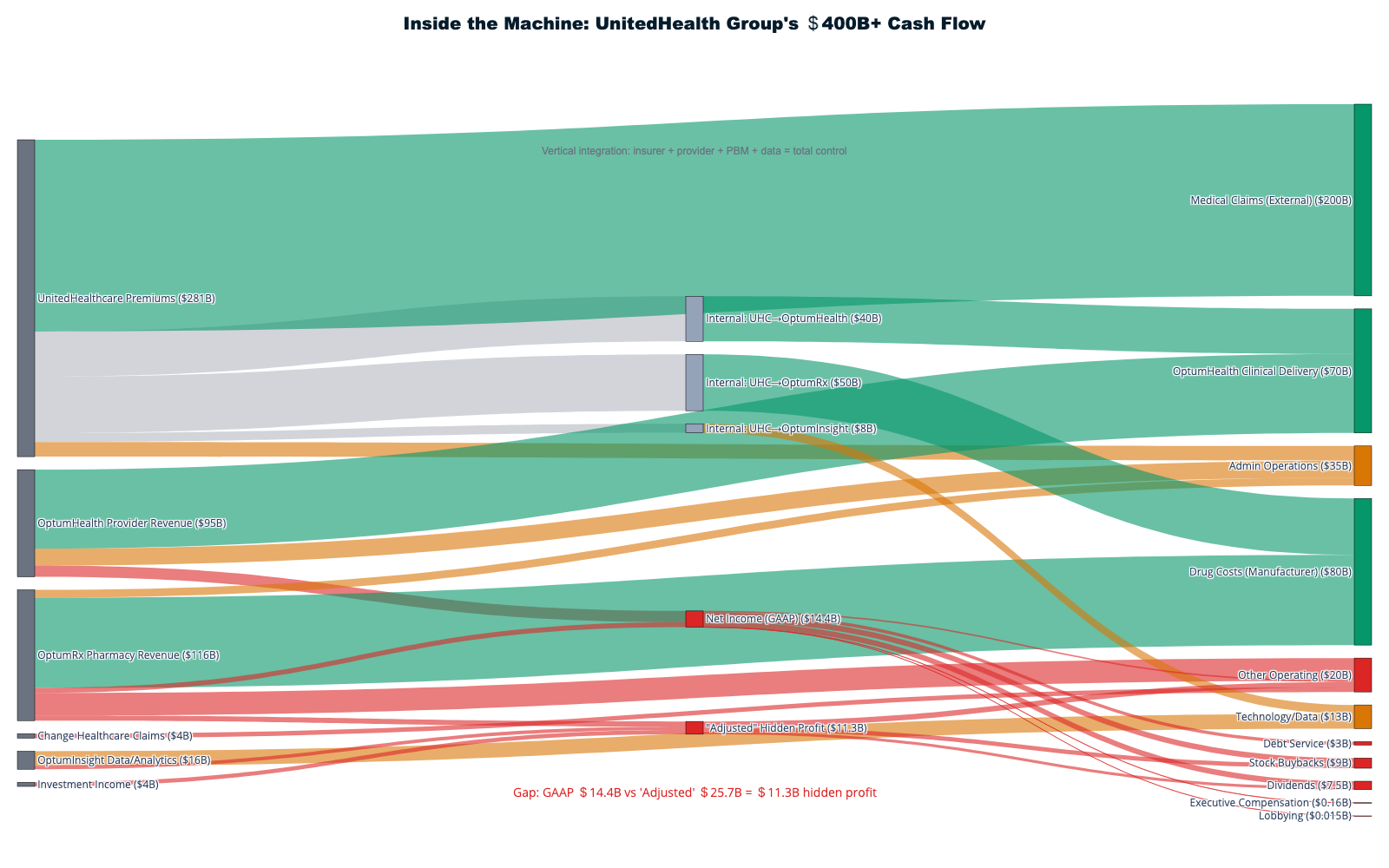
Modern healthcare extraction reaches its apotheosis through vertical integration, where massive conglomerates control every touchpoint with patients to extract maximum value while obscuring costs through intercompany transfers. UnitedHealth Group exemplifies this model: a $400.3 billion empire that demonstrates how owning the entire healthcare value chain enables systematic wealth extraction from patients and taxpayers at unprecedented scale.
The UnitedHealth Octopus: Eight Tentacles, One Extraction Purpose
UnitedHealth Group has constructed the most comprehensive vertical integration in American healthcare history, operating simultaneously as insurer, provider, pharmacy benefit manager, data processor, and claims administrator. The company's 2024 revenue of $400.3 billion—an 8% increase from $371.6 billion in 2023—flows through multiple extraction layers before any dollar reaches actual patient care [1]. This integration creates artificial internal markets where the company profits multiple times from the same patient interaction while eliminating competitive pressures that would reduce extraction opportunities.
The corporate structure reveals the extraction strategy with mathematical precision. UnitedHealthcare collects $281.4 billion in premium revenue while Optum generates $226.6 billion across its three divisions—Optum Health (provider services), OptumRx (pharmacy benefits), and Optum Insight (data analytics) [1]. When these divisions serve the same patients, every transaction becomes an optimization opportunity for total enterprise profit rather than competitive market dynamics.
UnitedHealthcare pays Optum Health facilities for medical services delivered to UnitedHealthcare members, with pricing controlled internally rather than by market competition. OptumRx fills prescriptions for UnitedHealthcare patients using formularies designed to maximize overall UnitedHealth profitability rather than patient cost minimization. Optum Insight monetizes the medical data generated across all these interactions, creating a fourth profit stream from the same patient encounters. The Change Healthcare acquisition—completed for $13 billion despite Department of Justice opposition—added claims processing for competitors, providing unprecedented market intelligence that enables extraction optimization [2].
This closed-loop system enables what economists call "transfer pricing"—the manipulation of internal transactions to optimize overall extraction. When UnitedHealthcare denies coverage for expensive specialty care, Optum Health providers offer alternative services that generate revenue for the same enterprise. When OptumRx excludes lower-cost medications from formularies, patients pay higher prices that benefit the broader UnitedHealth ecosystem through manufacturer rebates and pharmacy margins. These coordinated decisions appear independent but function as systematic extraction optimization across the integrated enterprise.
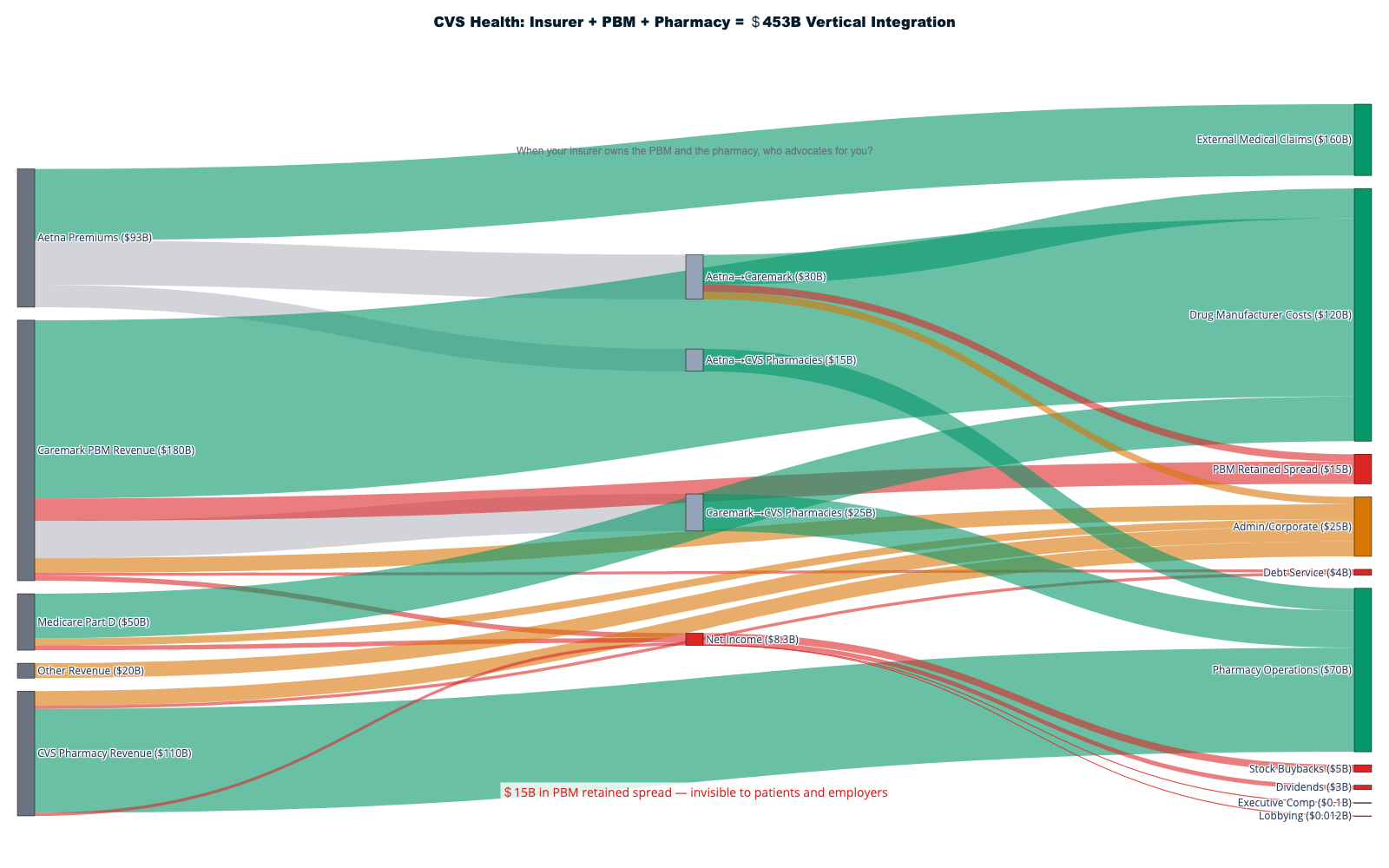
CVS Health: The Pharmacy-Insurance Death Star
CVS Health represents the second major extraction archetype, combining the nation's largest pharmacy chain with Aetna insurance serving 69 million members to profit from both ends of prescription transactions while controlling patient access through formulary manipulation. The $69 billion Aetna acquisition created a closed-loop system where patients with Aetna insurance find their prescription benefits systematically steered toward CVS pharmacies through preferential copays and network restrictions [3].
The pharmacy-insurance integration demonstrates extraction through artificial scarcity creation. Patients with Aetna coverage face substantially higher copays at competing pharmacies, creating economic coercion that drives traffic to CVS locations. CVS Specialty maintains exclusive contracts for expensive chronic disease medications, forcing patients requiring life-sustaining drugs to use CVS-owned pharmacies regardless of convenience, service quality, or competitive pricing. This captive customer base generates 30-40% profit margins on specialty pharmaceuticals compared to 2-3% margins on generic drug dispensing [4].
MinuteClinic and Oak Street Health complete CVS's integration strategy by providing care delivery that generates additional extraction opportunities. Patients receive primary care from CVS-employed providers who write prescriptions filled at CVS pharmacies, with Aetna processing insurance claims for both services. Every patient touchpoint generates revenue for the same corporate entity while competitors are systematically excluded from this closed-loop economy. The company's recent announcement of a $10 billion share buyback program demonstrates how patient care revenue flows directly to shareholders rather than care improvement or access expansion [5].
The Intercompany Shell Game: Looting Through Legal Arbitrage
Vertical integration's most sophisticated extraction mechanism operates through intercompany pricing manipulation that exploits regulatory gaps in Medical Loss Ratio calculations. When UnitedHealthcare pays Optum Health $300 for services that Medicare prices at $150, only $150 may count toward MLR compliance, but the transaction still extracts $150 in excess value from the premium pool while maintaining technical regulatory compliance [6].
This shell game creates systematic incentives for cost inflation throughout integrated systems. OptumRx negotiated $12.8 billion in manufacturer rebates during 2024, ostensibly to control drug costs for UnitedHealthcare members [7]. However, these rebates often benefit the broader UnitedHealth enterprise rather than reducing patient costs. The company's recent commitment to phase out rebate retention by 2028—moving to 100% pass-through—acknowledges the extent to which current structures serve corporate profits rather than patient interests.
The Change Healthcare acquisition amplifies extraction opportunities through information asymmetry that would be illegal in other industries. By processing claims for competitors while operating its own insurance and provider networks, UnitedHealth gains unprecedented insight into market pricing, utilization patterns, and competitive strategies. This competitive intelligence enables the company to optimize its own operations while systematically disadvantaging competitors who must rely on UnitedHealth's infrastructure [2].
Market Concentration: The Oligopoly Enabler
Vertical integration succeeds as extraction strategy because it operates within highly concentrated markets that eliminate competitive pressures. The top three PBMs—Express Scripts (Cigna), CVS Caremark, and OptumRx—control 80% of prescription claims with a Herfindahl-Hirschman Index of 1,972, far above the 1,800 threshold economists consider problematic for competition [8]. This concentration enables coordinated extraction strategies that would be impossible in competitive markets.
Health insurance markets demonstrate similar concentration patterns. UnitedHealthcare serves as the largest Medicare Advantage plan with 33 million enrollees, while maintaining denial rates of 12.8%—nearly double the industry average of 6.4% and far exceeding competitors like Humana (5.8%) and Elevance (4.2%) [9]. The company's scale enables more aggressive extraction strategies while providing sufficient market power to withstand regulatory pressure and competitive challenges.
Provider market concentration amplifies integration benefits by reducing negotiating power of independent physicians and hospitals. When UnitedHealth acquires physician practices through Optum Health, these providers lose independence to negotiate rates with competing insurers. The integrated model forces providers to accept UnitedHealth's pricing terms across all lines of business, creating systematic extraction opportunities unavailable to non-integrated competitors.
Legislative Architecture: The Regulatory Capture Foundation
The current extraction system depends on legislative frameworks that explicitly enable vertical integration while preventing effective oversight. The Employee Retirement Income Security Act (ERISA) preempts state insurance regulation for employer-sponsored plans covering 152 million Americans, allowing national insurers to avoid state-level consumer protections while operating across all markets [10]. This federal preemption creates regulatory arbitrage opportunities that vertically integrated companies exploit systematically.
Certificate of Need laws in 34 states create artificial barriers to entry that protect integrated systems from competition. When UnitedHealth seeks to expand Optum Health facilities in CON states, independent competitors cannot establish competing services because regulatory approval favors established players with resources to navigate complex bureaucratic procedures. These laws function as incumbent protection mechanisms that enable extraction through reduced competition [11].
The Medicare Modernization Act's prohibition on direct government drug price negotiation—only recently modified for ten medications—created the PBM intermediary market that integrated companies now dominate. By preventing Medicare from negotiating directly with pharmaceutical manufacturers, Congress created a multi-billion-dollar extraction opportunity that companies like UnitedHealth capture through OptumRx operations [12].
Medicare Advantage overpayments exemplify how regulation enables extraction from taxpayers. UnitedHealth's MA plans received an estimated $22 billion in federal overpayments during 2024 while maintaining the highest denial rates in the industry [13]. The company's integrated structure allows it to deny care at the insurance level while profiting from alternative services delivered through Optum Health providers, creating dual extraction opportunities from single patient encounters funded by taxpayer subsidies.
The Extraction Multiplication Effect
Vertical integration functions as an extraction multiplier that enables companies to profit 3-5 times from the same patient interaction through coordinated pricing across business lines. A diabetic patient covered by UnitedHealthcare generates insurance margin when coverage is approved, provider facility fees when care is delivered at Optum Health facilities, pharmacy markups when prescriptions are filled through OptumRx preferred networks, and data monetization when medical information is processed through Optum Insight analytics.
This multiplication effect explains why healthcare stocks have dramatically outperformed broader markets since ACA implementation. Health insurer stocks increased 1,032% from 2010-2024 compared to 251% S&P 500 growth—a 4:1 outperformance that reflects the market's recognition of integrated extraction capacity rather than care delivery excellence [14]. UnitedHealth's market capitalization expanded from $39 billion in 2010 to $265 billion in 2026, representing $226 billion in shareholder wealth creation funded entirely by patient premiums and taxpayer subsidies.
Vertical integration in healthcare represents extraction capitalism's maturation, where controlling market infrastructure becomes more profitable than delivering superior outcomes. Until policymakers address ERISA preemption, eliminate CON laws, and break up integrated oligopolies, vertical integration will continue expanding as healthcare's dominant extraction mechanism—prioritizing shareholder returns over patient welfare with mathematical precision and systemic brutality.
Chapter 5: Hospital Consolidation & the For-Profit Machine
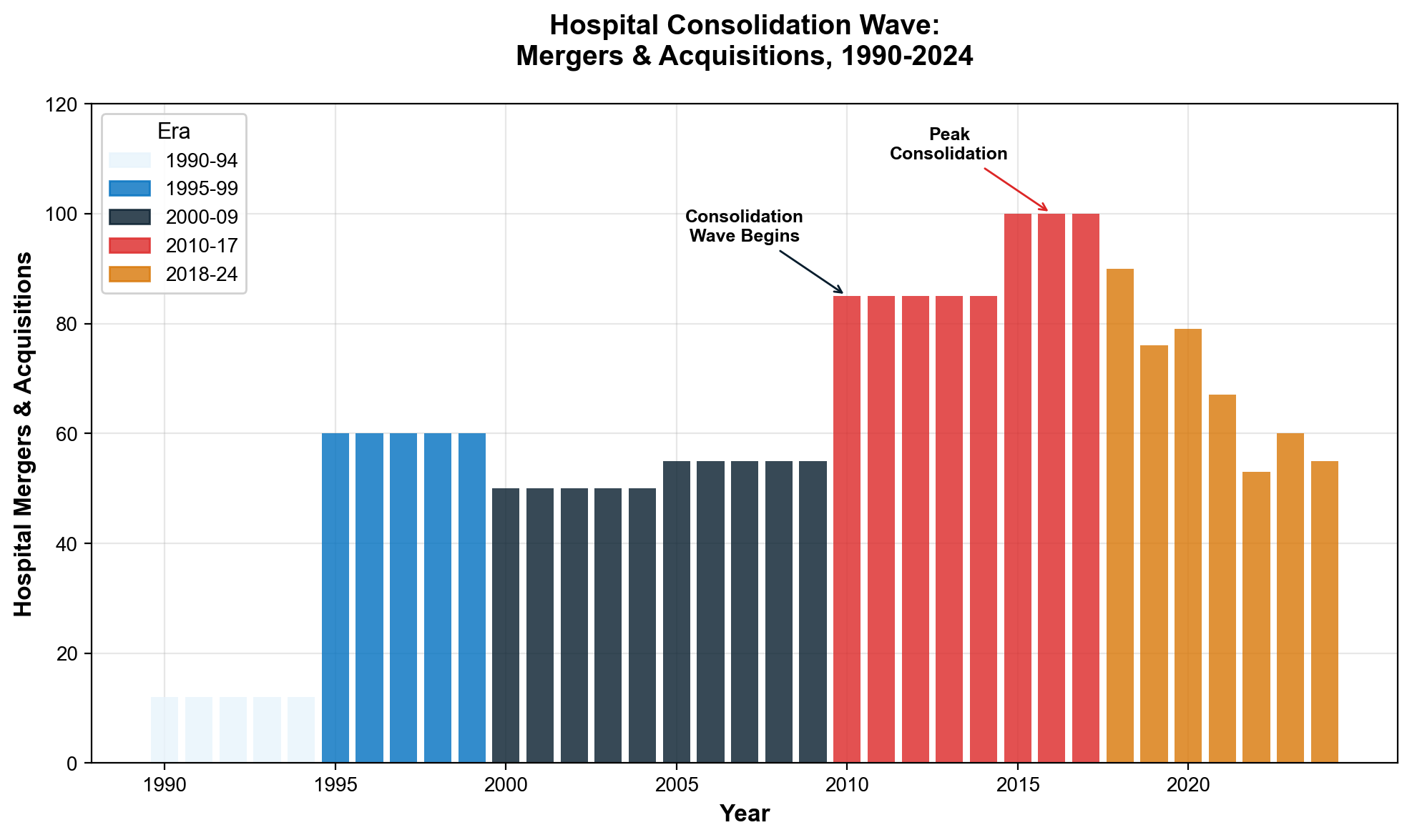
Hospital consolidation has transformed American healthcare delivery through systematic merger activity that prioritizes extraction over patient care, creating regional monopolies that generate billions annually through facility fees, price arbitrage, and market manipulation. Since 1990, 1,573 documented hospital mergers have fundamentally altered competitive dynamics while demonstrating how asset accumulation and financial engineering extract wealth from communities that funded these institutions through tax exemptions and public subsidies.
The Merger Tsunami: 1,573 Deals, Unlimited Extraction
Hospital consolidation accelerated following healthcare deregulation, with mergers doubling from 12 annually in the mid-1980s to 24 per year by the early 1990s—establishing the template for systematic market concentration that continues today [15]. Between 1998 and 2017, healthcare systems completed 1,573 hospital mergers that reshaped metropolitan markets nationwide, while 428 additional mergers occurred between 2018-2023, including 72 transactions in 2024 alone [16].
The pace reveals coordinated industry strategy rather than organic market evolution. Consolidation reached critical mass by 2016, when 90% of metropolitan statistical areas qualified as highly concentrated hospital markets. This concentration increased further between 2017-2021, with highly concentrated metro areas rising from 71% to 77% despite existing monopolistic conditions [17]. Hospital systems deliberately pursued market dominance to enable extraction opportunities impossible under competitive conditions.
Market concentration enables systematic price extraction through reduced competition and enhanced insurer bargaining power. The share of community hospitals operating within larger health systems increased from 53% in 2005 to 68% in 2022, representing wholesale transformation of hospital ownership from community-controlled institutions to corporate profit centers [18]. This ownership shift fundamentally altered hospitals' mission from community service to shareholder returns, with predictable consequences for pricing and access.
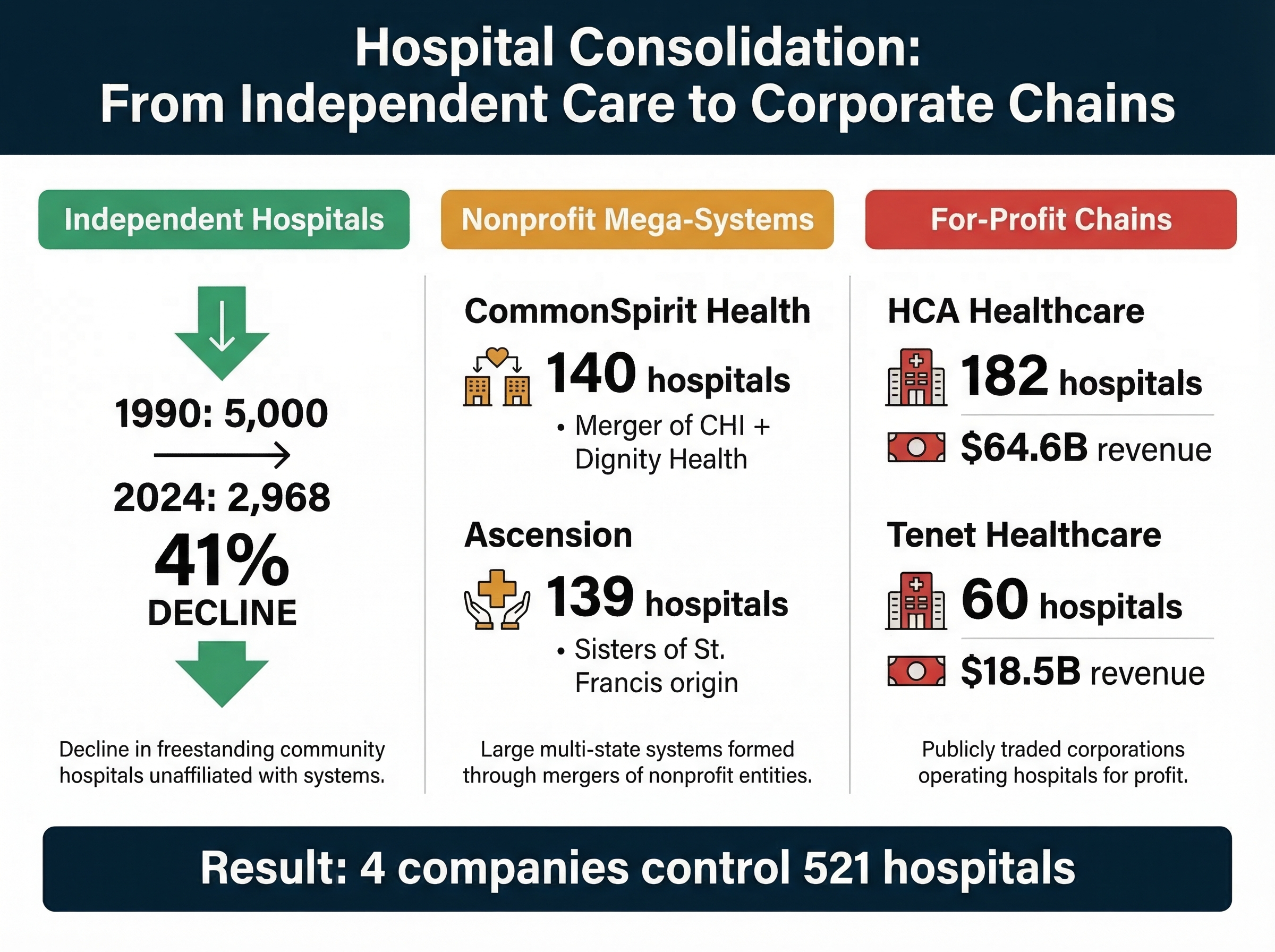
HCA Healthcare: Private Equity's Extraction Template
HCA Healthcare exemplifies the private equity approach to hospital extraction, demonstrating how leveraged buyouts and financial engineering transform healthcare delivery into profit maximization engines. The company's 2006 leveraged buyout—valued at $33.2 billion with only $21 billion in cash—established the template for extraction-focused hospital ownership that prioritizes debt service over patient care [19].
The transaction structure revealed systematic extraction planning from day one. A consortium led by KKR, Bain Capital, and Merrill Lynch Private Equity acquired HCA through massive leverage, with Frist family members contributing $1.12 billion and Cerberus providing $246 million representing just 4% equity stake. The remaining 96% of the transaction was financed through debt assumption and new borrowing, immediately saddling the hospital chain with enormous interest obligations that drove all subsequent operational decisions [20].
Financial engineering results became apparent within three years as HCA systematically reduced expenses and staffing relative to competitors while achieving substantially higher cash-flow margins through market manipulation. The company decreased capital investment significantly from 2006-2009, deferring infrastructure maintenance and equipment upgrades to service debt obligations rather than maintain clinical quality. These decisions generated short-term cash flow for debt service while degrading long-term hospital capacity and patient care quality [21].
Current HCA performance demonstrates the long-term extraction model's success from a shareholder perspective. The company reported $70.6 billion in revenue for 2024 with 8.2% profit margins while announcing a massive $10 billion share buyback program [22]. This buyback—representing one-seventh of annual revenue—demonstrates how patient care dollars flow directly to shareholders rather than reinvestment in healthcare delivery capacity, medical equipment, or community health improvement.
HCA's Senate Pipeline: The Frist Family Connection
HCA's political connections represent one of the most direct pipelines between healthcare extraction and legislative power. The company was co-founded in 1968 by Dr. Thomas Frist Sr. and his son Thomas Frist Jr. The family's other son — Senator Bill Frist (R-TN) — served as U.S. Senate Majority Leader from 2003 to 2007. His tenure coincided with passage of the Medicare Modernization Act of 2003 (Medicare Part D), which prohibited government drug price negotiation — the single most valuable legislative gift to the healthcare industry in modern history. The Frist family fortune of approximately $1.8 billion is overwhelmingly derived from HCA stock, creating structural alignment between legislative influence and the company's financial interests. [193] In an unguarded moment, Senator Frist told the Boston Globe that conversations with his doctor father about the family calling were like "benign versions of the Godfather and Michael Corleone."
The human cost of HCA's financial engineering appears in systematic understaffing, delayed care, and community hospital closures that eliminate access for vulnerable populations. The company's focus on high-margin procedures and wealthy patient populations while avoiding charity care obligations reveals how private equity transforms healthcare from public service to wealth extraction mechanism.
The Non-Profit Shell Game: Tax Exemption for Executive Enrichment
Non-profit hospitals represent healthcare extraction's most sophisticated and cynical mechanism, combining federal tax exemptions worth billions annually with executive compensation and cash accumulation strategies that rival for-profit enterprises. Major non-profit health systems maintain CEO compensation exceeding $5-10 million annually while accumulating massive cash reserves and investment portfolios, generating returns while claiming financial distress to justify price increases and service cuts [23].
The community benefit accounting fraud enables systematic extraction under tax-exempt cover. Non-profit hospitals receive federal, state, and local tax exemptions theoretically in exchange for providing "community benefit" equal to exemption value. However, community benefit calculations include bad debt written off as "charity care," administrative costs of charity programs, medical education expenses often federally funded, and research costs—allowing systems to claim community benefits that far exceed actual charitable care delivery [24].
Cash reserve analysis exposes the profit accumulation disguised as financial necessity. Large non-profit health systems maintain billions in cash reserves and investment portfolios while simultaneously claiming financial constraints necessitating price increases, service cuts, and staff reductions. Cash-to-debt ratios at major non-profits often exceed for-profit competitors, proving that "non-profit" status functions primarily as tax optimization rather than commitment to affordable care [25].
Mayo Clinic exemplifies non-profit wealth accumulation while maintaining tax-exempt status. The system reported $17.6 billion in revenue and $2.3 billion in operating margin while maintaining massive cash reserves and paying CEO salaries exceeding $10 million annually [26]. These financial metrics match for-profit enterprises while benefiting from tax exemptions unavailable to explicitly profit-seeking businesses, demonstrating systematic gaming of non-profit regulations.
Real estate holdings create additional extraction vectors through sale-leaseback arrangements and related-party transactions. Non-profit hospitals accumulate valuable real estate through tax-exempt property acquisition, then engage in sale-leaseback deals with affiliated entities or REITs that extract value while creating long-term lease obligations burdening future operations. These transactions monetize tax-exempt asset accumulation while maintaining operational control [27].
Facility Fee Arbitrage: 87% Markup for Identical Services
Facility fee extraction represents hospital profiteering in its purest form, enabling 67-87% price increases for identical medical services based solely on ownership structure rather than care quality or resource utilization differences. Health Cost Institute analysis reveals systematic price arbitrage that extracts billions annually through billing manipulation rather than medical value creation [28].
Primary care visit pricing demonstrates the arbitrage opportunity with mathematical precision. A routine primary care office visit costs an average of $116 at independent physician practices versus $217 at hospital outpatient departments—an 87% price increase driven entirely by a $101 facility fee component added for identical services [29]. The facility fee represents pure extraction since no additional medical resources, equipment, or expertise justify the price differential.
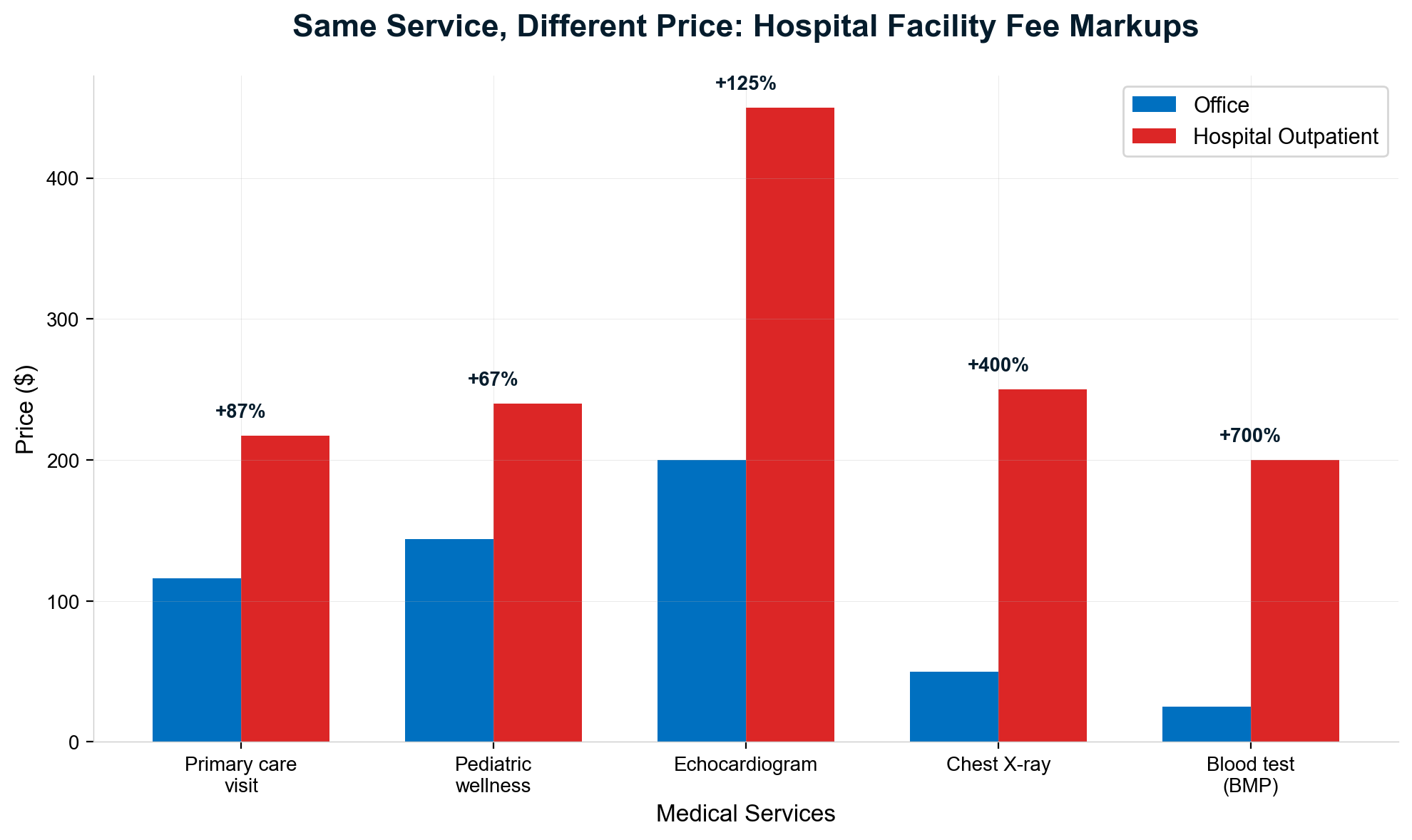
Pediatric wellness visits demonstrate similar extraction patterns with $144 costs at independent practices versus $240 at hospital-owned locations, representing a 67% markup with a $96 facility fee for identical preventive care [30]. These price differentials exist despite identical examination procedures, equipment utilization, and clinical outcomes, proving extraction based purely on billing location rather than medical value.
Laboratory testing reveals even more extreme extraction ratios, with hospital outpatient labs charging 3.5 times more than independent facilities for identical tests using equivalent equipment and procedures [31]. This pricing manipulation generates substantial revenue from routine diagnostic testing while providing no superior accuracy, convenience, or medical value compared to independent laboratories.
The aggregate revenue impact demonstrates systematic profiteering scale. Health Cost Institute data shows facility fees generated $77 million in total spending for just primary care and pediatric wellness visits in 2022, with 24 of 43 analyzed states maintaining average facility fees above $100 [32]. When extrapolated across all hospital-owned outpatient services, facility fee extraction likely exceeds $10-15 billion annually in pure markup for identical medical services.
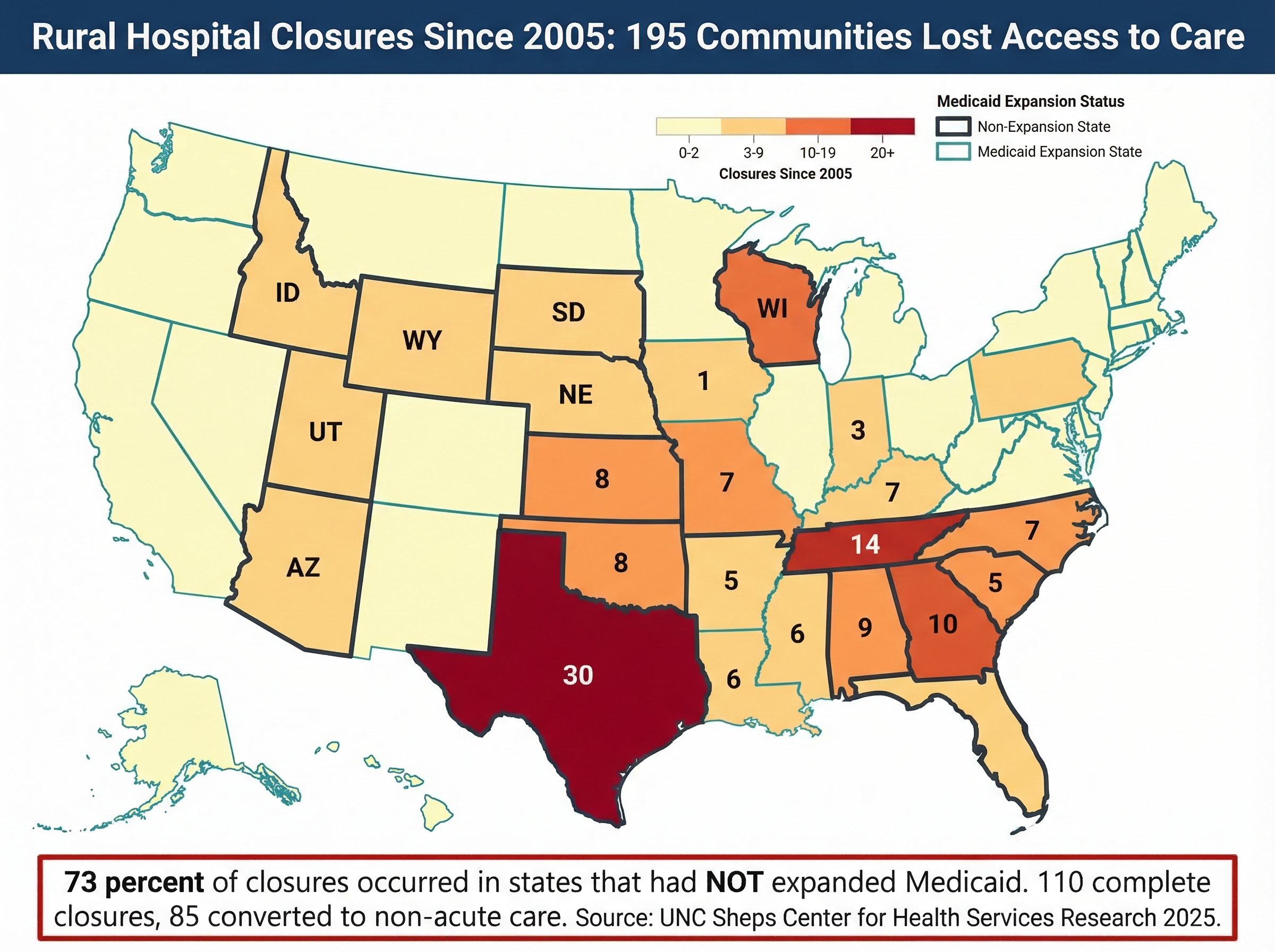
Rural Hospital Closures: 181 Hospitals, 2.5 Million Americans
Hospital consolidation's most devastating impact appears in rural communities where merger activity systematically eliminates healthcare access for entire regions. Rural hospitals' economics make them particularly vulnerable to acquisition by systems that prioritize profitable urban operations over community healthcare infrastructure, leading to systematic service elimination and facility closure [33].
Rural hospital closure statistics reveal consolidation's human cost with brutal clarity. Since 2010, 181 rural hospitals have closed permanently, eliminating hospital access for approximately 2.5 million Americans who must now travel 30+ miles for emergency care, obstetrics, and inpatient services [34]. Service line elimination often precedes full closure, with rural hospitals systematically cutting obstetrics, behavioral health, and emergency services that require staffing investment but generate lower margins than urban procedures.
The consolidation closure paradox demonstrates extraction priorities over community service. Research shows financially strong rural hospitals face higher closure risk after joining larger systems, indicating that acquisitions serve asset extraction rather than rural healthcare strengthening [35]. Systems acquire profitable rural facilities to extract value through real estate transactions, service line elimination, and cash flow redirection to urban operations rather than maintaining rural healthcare infrastructure.
Private equity involvement amplifies rural destruction through systematic asset stripping disguised as operational efficiency. The Steward Health Care collapse exemplifies this approach: Cerberus acquired the chain through leverage loading, extracted value through real estate sales, and ultimately abandoned rural facilities when debt service became unsustainable [36]. This pattern—acquisition, extraction, abandonment—represents private equity's systematic approach to rural healthcare as temporary profit opportunity rather than community infrastructure.
The social cost of rural closure extends far beyond medical access to community economic destruction and population decline. Hospital closure eliminates 100-300 local jobs while reducing property values and business investment throughout rural counties. Emergency services elimination forces patients to delay care during heart attacks, strokes, and trauma situations, directly causing deaths that wouldn't occur with maintained local access [37].
Certificate of Need: Incumbent Protection Racket
Certificate of Need laws in 34 states function as incumbent protection mechanisms that reduce competition and enable pricing extraction by existing hospital systems. These regulations require state approval for hospital expansion, new facility construction, or major equipment acquisition, creating artificial barriers to entry that protect consolidated systems from competitive pressure [38].
Market impact evidence demonstrates how CON laws enable systematic extraction through reduced competition. Research shows CON laws increase healthcare prices by limiting supply, protect inefficient incumbents from market discipline, and enable existing providers to earn monopoly profits unavailable in competitive markets [39]. The artificial scarcity created by CON approval processes allows incumbents to charge premium prices while providing mediocre service quality.
The Ballad Health case study reveals CON law consequences with devastating precision. Tennessee and Virginia granted the system Certificate of Public Advantage (COPA) creating a government-sanctioned monopoly across the border region, promising cost savings that never materialized [40]. State-approved merger with antitrust immunity enabled market dominance that resulted in price increases, service reductions, and care quality degradation throughout the service area.
Regulatory capture evidence shows how incumbents systematically manipulate CON processes to prevent competition. Existing hospitals routinely file frivolous competing applications to delay new entrants, challenge competitor proposals through administrative procedures, and staff regulatory boards with industry representatives who protect existing operators [41]. This systematic gaming ensures incumbent systems maintain extraction opportunities while preventing competitive alternatives.
CON law elimination in states that repealed these regulations demonstrates immediate competitive benefits including price reduction, service expansion, and quality improvement. When Pennsylvania eliminated CON requirements, hospital competition increased substantially while prices decreased and access expanded [42]. These natural experiments prove CON laws serve incumbent protection rather than healthcare planning or cost control.
Hospital consolidation represents extraction capitalism's systematic transformation of community healthcare assets into profit-maximizing enterprises through financial engineering, market manipulation, and regulatory capture. The 1,573 documented mergers, HCA's $10 billion buyback program, 87% facility fee markups for identical services, 181 rural closures affecting 2.5 million Americans, and CON law protection of incumbent monopolies demonstrate how consolidation prioritizes extraction over healthcare delivery. Until antitrust enforcement addresses healthcare market concentration and Certificate of Need laws are eliminated nationwide, hospital consolidation will continue operating as wealth extraction mechanism that systematically harms patients and communities while enriching shareholders and private equity investors.
Chapter 6: PBM & Pharmacy Benefit Extraction
Pharmacy Benefit Managers operate the most opaque and systematically predatory component of American healthcare, functioning as gatekeepers between patients and life-sustaining medications while extracting billions through spread pricing, rebate manipulation, and vertical integration schemes that profit from medical necessity. The Big Three PBMs—Express Scripts, CVS Caremark, and OptumRx—control 80% of prescription transactions, wielding oligopoly power to extract value from manufacturers, pharmacies, insurers, and patients simultaneously while adding no clinical value to medication access or delivery.
The PBM Oligopoly: 80% Control, 100% Extraction
Market concentration in pharmacy benefits has reached levels that would trigger antitrust enforcement in any other industry, with three companies controlling 80% of all U.S. prescription claims through a web of vertical integration that eliminates meaningful competition. Express Scripts (Cigna) processes 30% of prescriptions, CVS Caremark maintains 27% market share, and OptumRx (UnitedHealth) controls 23%, creating a combined market concentration index of 1,972—far above the 1,800 threshold economists consider dangerous for consumer welfare [43].
This oligopoly structure enables systematic extraction because patients, pharmacies, and health plans have no realistic alternatives to PBM-controlled networks and pricing structures. When OptumRx excludes independent pharmacies from UnitedHealthcare networks, 33 million members must use PBM-preferred locations regardless of convenience, service quality, or competitive pricing. CVS Caremark steers Aetna's 69 million members toward CVS pharmacies through differential copays and network restrictions, creating captive customer flows worth billions in additional pharmacy revenue [44].
Vertical integration amplifies extraction opportunities beyond simple market concentration by enabling companies to profit multiple times from single prescription transactions. When a UnitedHealthcare member fills a prescription through OptumRx, the company captures PBM processing fees, insurance margins, pharmacy dispensing profits, and manufacturer rebates—all from one patient interaction. Competing pharmacies and insurers cannot replicate this multi-layered extraction model, creating systematic competitive disadvantages that drive further consolidation [45].
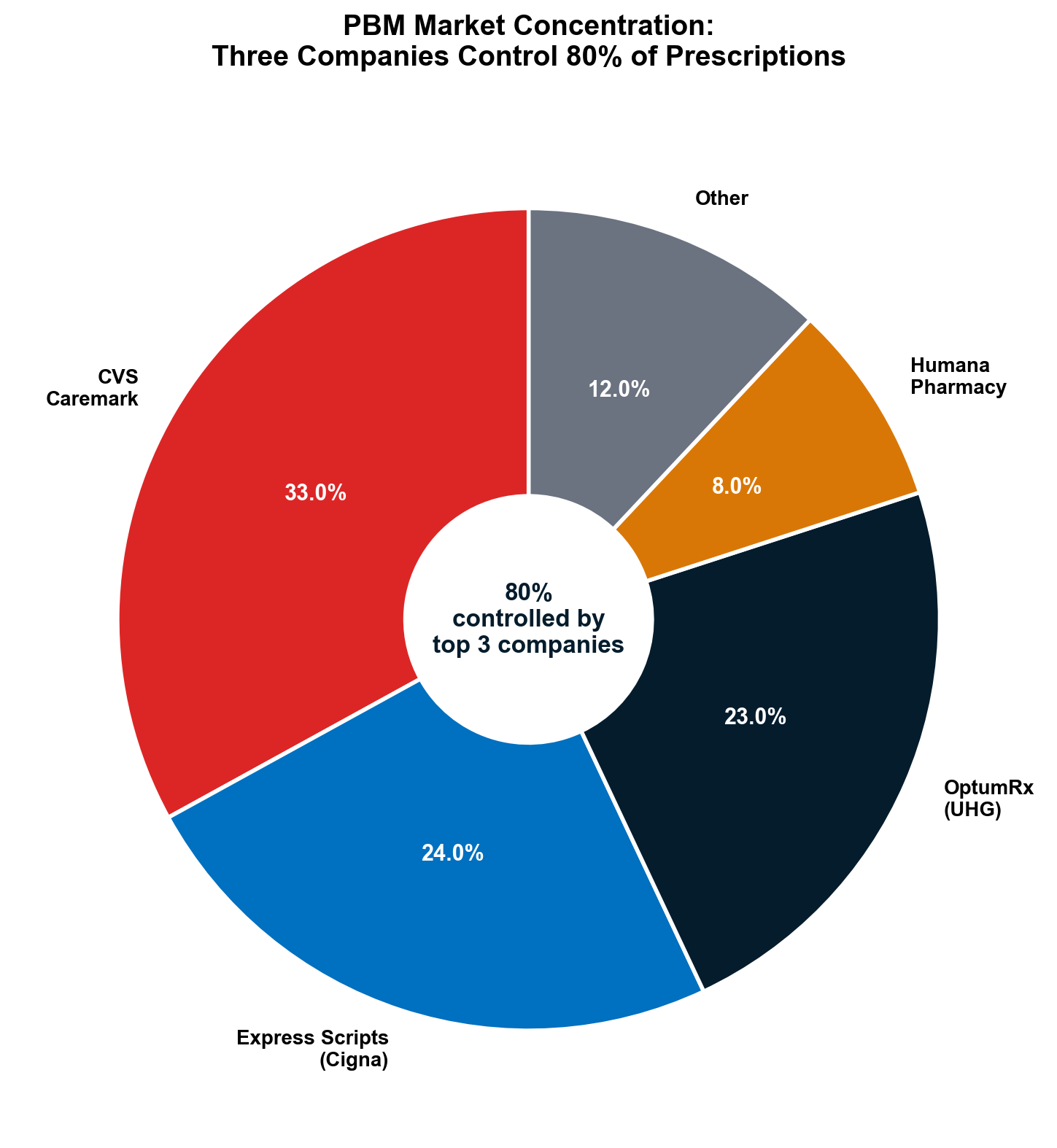
The anti-competitive effects extend beyond pricing to fundamental healthcare access. PBMs maintain "preferred networks" that exclude independent pharmacies serving rural and underserved communities, forcing patients to travel substantial distances for prescription access or pay prohibitive out-of-network costs. This geographic redlining systematically eliminates pharmacy competition while creating healthcare deserts that particularly harm elderly and disabled populations [46].
Insulin Price Manipulation: The $274 Criminal Conspiracy
The Federal Trade Commission's insulin price investigation provides definitive proof of PBM extraction mechanisms, documenting how rebate-chasing strategies artificially inflated life-sustaining medication prices by over 1,200% while PBMs collected billions in hidden profits from patients facing life-threatening rationing decisions. The Humalog price explosion from $21 in 1999 to $274+ by 2017 resulted directly from PBM rebate addiction rather than manufacturing costs, research investments, or therapeutic improvements [47].
The FTC's September 2024 administrative complaint against all three major PBMs details the extraction mechanism with prosecutorial precision. Starting in 2012, PBMs created exclusionary formularies threatening to exclude insulin products unless manufacturers paid increasingly larger rebates calculated as percentages of list prices [48]. Higher list prices generated proportionally higher rebate dollars for PBMs, creating perverse incentives to inflate prices rather than negotiate cost reductions—transforming PBMs from cost controllers into price inflators.
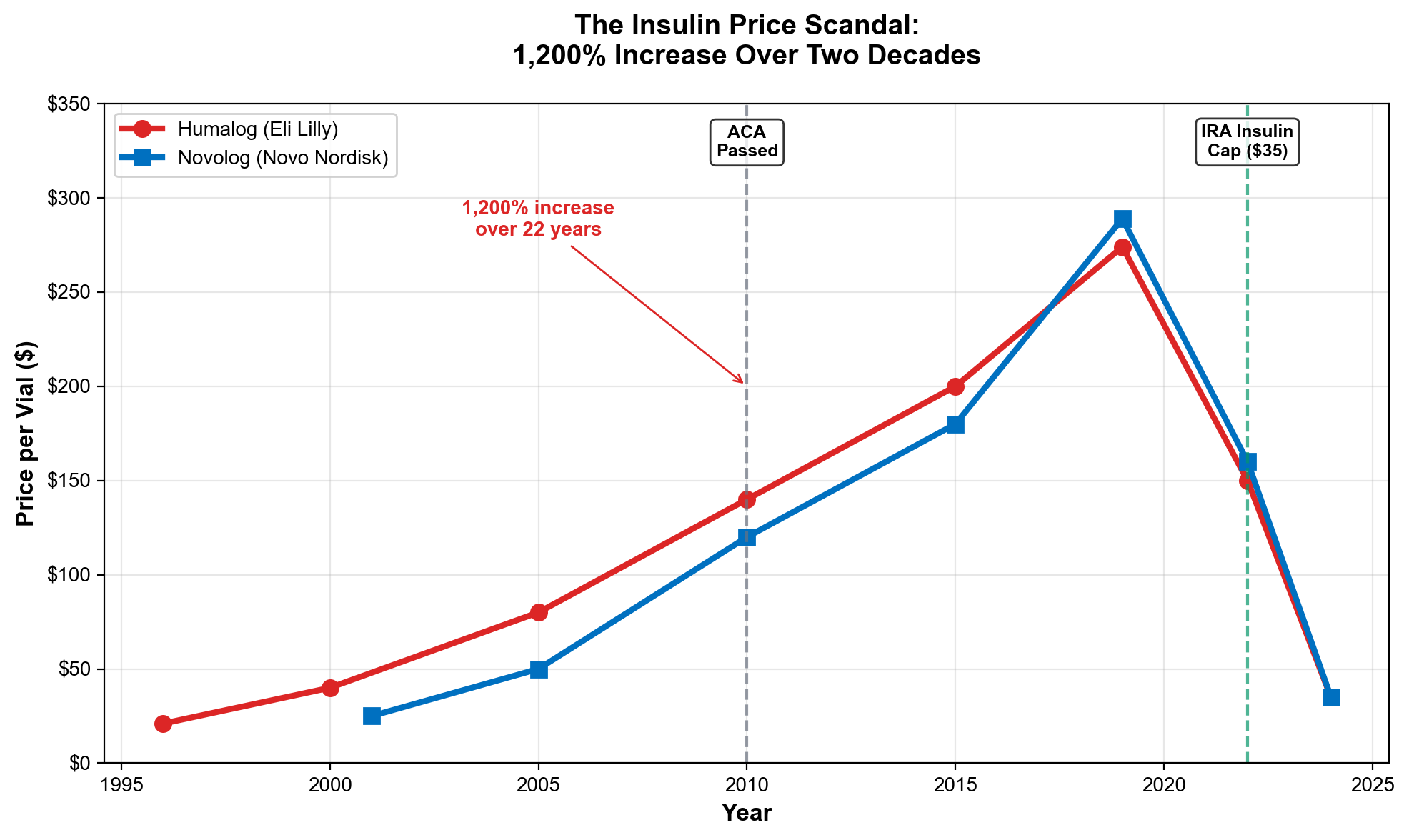
Novolog pricing data confirms the systematic manipulation with damning mathematical precision. The insulin's list price increased from $122.59 in 2012 to $289.36 in 2018—a 136% increase driven by rebate negotiations despite no meaningful formulation changes or manufacturing improvements [49]. When lower-cost insulin alternatives became available, PBMs systematically excluded them from formularies to maintain higher rebate income, as described by internal Novo Nordisk communications referencing PBM "addiction to rebates" [50].
The human cost of this extraction appears in systematic insulin rationing by diabetic patients unable to afford PBM-inflated prices. Research documented 1.3 million diabetic Americans rationing insulin due to cost barriers, with documented deaths resulting from delayed or skipped insulin administration [51]. Each diabetic death from insulin rationing represents the ultimate extraction: PBMs literally profited from pricing patients out of life-sustaining medication access.
PBM rebate retention exacerbates patient harm by ensuring price inflation benefits never reach patients requiring insulin. While PBMs collect billions in rebates ostensibly to control drug costs, they retain substantial portions rather than passing savings to patients. Diabetic patients with high-deductible insurance pay full inflated list prices at pharmacy counters while their PBMs collect rebates based on those same inflated prices—creating double extraction from the most vulnerable patients [52].
Spread Pricing: The Invisible Markup Machine
Spread pricing represents PBM extraction in its purest form—buying medications at negotiated prices, billing insurers at higher amounts, and retaining the difference as pure profit without providing any additional clinical value. State Medicaid audits revealed hundreds of millions in hidden markups through spread pricing, leading multiple states to ban the practice in government programs while commercial insurance remains largely unregulated [53].
The mechanism operates through systematic information asymmetry that prevents both pharmacies and health plans from understanding true medication costs. PBMs pay independent pharmacies fixed reimbursement amounts for prescription dispensing while charging health plans different amounts for identical medications. The "spread" between pharmacy reimbursement and health plan charges becomes pure PBM profit, hidden through contractual complexity and claims processing opacity that prevents either party from calculating markup percentages [54].
Ohio's Medicaid audit exposed spread pricing scale with devastating clarity. The state discovered PBMs charged Medicaid managed care plans $244.8 million more than they paid pharmacies for identical prescription transactions during 2017 alone, representing systematic overcharging of taxpayer funds through hidden markups [55]. Illinois found similar patterns with $99.3 million in spread pricing overcharges, while Arkansas documented $29.8 million in excess PBM charges through spread pricing schemes.
Commercial insurance spread pricing remains largely unquantified because PBM contracts prevent disclosure of actual payment amounts to pharmacies or health plans. However, industry estimates suggest $15-20 billion in annual extraction through commercial market spread pricing, with markups typically ranging from 15-40% above actual pharmacy costs for generic medications and potentially higher percentages for specialty drugs [56].
The extraction compounds through coordination between spread pricing and rebate collection. PBMs simultaneously collect manufacturer rebates while charging health plans spreads above pharmacy reimbursement levels, creating dual revenue streams from identical prescription transactions. This double-extraction enables PBMs to profit from both medication cost inflation and artificial pricing markup while adding no therapeutic value [57].
DIR Fees: Post-Sale Extortion Destroying Independent Pharmacies
Direct and Indirect Remuneration (DIR) fees represent perhaps the most predatory PBM extraction mechanism, enabling retroactive fee assessments that destroy independent pharmacy economics while generating billions in additional PBM revenue through systematic post-sale clawbacks. The National Community Pharmacists Association's 2024 survey documents wholesale pharmacy destruction through DIR fee manipulation that would constitute criminal extortion in any other industry [58].
The clawback mechanism operates through delayed fee assessment that prevents pharmacies from understanding final reimbursement until months after providing patient services. Independent pharmacies fill prescriptions and receive initial payments from PBMs, often below medication acquisition costs. Weeks or months later, PBMs assess additional "DIR fees" that retroactively reduce payments, forcing pharmacies to absorb losses on prescriptions they've already dispensed to patients [59].
How DIR Fees Work: A Concrete Example
1. A pharmacist fills a generic prescription. The PBM's adjudicated price: $15.00. Pharmacist's wholesale cost: $8.00. Apparent margin: $7.00.
2. Three months later, the PBM retroactively assesses a DIR fee of $9.50 — clawed back from future reimbursements.
3. Net result: The pharmacy lost $2.50 on the transaction. The pharmacist didn't know this would happen when filling the prescription.
Similarly, spread pricing: A PBM reimburses a pharmacy $10 but charges the health plan $25. The $15 "spread" is PBM profit. Ohio's Medicaid audit found $244.8 million in spread pricing by a single PBM in one state in one year. [141]
The scale of pharmacy destruction reveals DIR fees' systematic impact on healthcare access. NCPA data shows 448 independent pharmacies closed during just six months of 2024, with 99% reporting decreased reimbursements since DIR rule changes [60]. Over 50% of independent pharmacies now lose money on three or more out of every ten prescriptions filled, while 60%+ lose money on 60% of Medicare Part D prescriptions after accounting for operating costs and DIR fee clawbacks.
Rural healthcare access suffers disproportionate damage as DIR fees force closures of pharmacies providing the only prescription access within 30+ mile radii. Independent pharmacies often serve as rural healthcare hubs, providing immunizations, medication counseling, and basic health services beyond prescription dispensing. When DIR fees force closures, patients lose comprehensive healthcare access while gaining nothing in return—pure social destruction for PBM profit extraction [61].
The Medicare Part D participation crisis demonstrates DIR fees' systematic destructiveness. NCPA reports 32% of independent pharmacy owners considered closure during 2024, while 93% threatened Medicare Part D withdrawal if DIR fee conditions persisted [62]. This potential network collapse would eliminate prescription access for millions of Medicare beneficiaries while demonstrating how PBM extraction systematically undermines healthcare infrastructure to maximize corporate profits.
Express Scripts Settlement: $7 Billion Extraction Acknowledgment
The February 2026 Express Scripts settlement with federal regulators provides definitive acknowledgment of systematic PBM extraction while demonstrating the scale of hidden overcharges built into America's prescription drug system. The settlement requires Express Scripts to fundamentally alter its business model without monetary penalties but mandates changes estimated to generate $7 billion in patient cost savings over ten years [63].
Structural reforms address core extraction mechanisms that the FTC identified as consumer violations. Express Scripts must eliminate rebate retention schemes prioritizing high-rebate drugs over lower-cost alternatives, implement transparent pricing structures preventing spread pricing manipulation, and modify formulary practices that excluded cost-effective medications for profit optimization [64]. The settlement essentially prohibits the "chase-the-rebate" strategy that drove insulin price inflation and similar medication cost increases.
The $7 billion savings estimate reveals extraction scale across the PBM industry with mathematical precision. If Express Scripts alone must provide $7 billion in cost reductions over ten years, total PBM extraction from the American healthcare system likely exceeds $50+ billion annually across all three major companies [65]. This extraction represents direct wealth transfer from patients, employers, and taxpayers to PBM shareholders through artificial pricing manipulation and rebate optimization.
Ongoing litigation against CVS Caremark and OptumRx may yield additional settlements requiring similar business model changes. However, the Express Scripts agreement's lack of monetary penalties suggests regulators prioritize structural changes over punishment, potentially enabling other PBMs to negotiate similar deals that maintain profitability while reducing the most egregious extraction practices [66].
The settlement's timing coincides with growing congressional pressure for comprehensive PBM reform, including proposals to ban spread pricing, require rebate transparency, and separate PBM operations from pharmacy ownership. Express Scripts' proactive settlement likely reflects recognition that voluntary compliance may prevent more restrictive legislation that would eliminate extraction opportunities entirely [67].
The Common Ownership Web: BlackRock's Pharmacy Portfolio
Behind PBM consolidation lies common ownership by institutional investors who benefit from reduced competition across the entire pharmacy supply chain. BlackRock, Vanguard, and State Street maintain substantial ownership stakes in all three major PBMs plus major pharmaceutical manufacturers and retail pharmacy chains, creating aligned interests that discourage competitive pricing and encourage coordinated extraction [68].
BlackRock's healthcare portfolio demonstrates this common ownership concentration with mathematical precision. The firm maintains major positions in CVS Health, Cigna Group (Express Scripts), UnitedHealth Group (OptumRx), plus pharmaceutical giants Eli Lilly, Johnson & Johnson, and Pfizer [69]. Since the same institutional investors profit from higher drug prices, PBM extraction, and pharmacy margins simultaneously, they have little incentive to pressure portfolio companies toward competitive pricing that would reduce total returns.
This institutional ownership structure explains PBM industry coordination on extraction strategies despite theoretical competition. When BlackRock benefits from CVS Caremark's spread pricing, Express Scripts' rebate retention, and OptumRx's specialty pharmacy steering simultaneously, the firm's optimal strategy involves supporting practices that maximize total portfolio extraction rather than competitive differentiation between individual companies [70].
The common ownership problem extends beyond PBMs to encompass the entire prescription drug supply chain, from manufacturers through distributors to retail pharmacies. This vertical ownership concentration enables coordinated pricing strategies that extract maximum value from patients and taxpayers while maintaining the appearance of competitive markets [71].
PBM extraction represents systematic predation on patients requiring life-sustaining medications, exploiting medical necessity to maximize profit extraction while destroying pharmacy competition and inflating medication costs. The Big Three's 80% market control, insulin price manipulation generating 1,200% increases through rebate addiction, spread pricing worth hundreds of millions annually, DIR fees destroying 448 independent pharmacies in six months, and the Express Scripts settlement acknowledging $7 billion in overcharges demonstrate how PBMs operate as profit-maximizing intermediaries that add no clinical value while extracting maximum wealth from patients, taxpayers, and healthcare providers. Until Congress eliminates spread pricing, bans vertical integration between PBMs and pharmacies, requires complete rebate transparency, and breaks up the Big Three oligopoly, PBMs will continue functioning as systematic wealth extraction mechanisms that prioritize shareholder returns over patient access to life-sustaining medications.
Chapter 7: Insurance Industry Financial Engineering
The health insurance industry has perfected financial engineering mechanisms that extract maximum profit from patient premiums while systematically denying medically necessary care through sophisticated strategies including medical loss ratio gaming, prior authorization abuse, Medicare Advantage overpayment capture, and massive stock buyback programs that convert patient suffering into concentrated shareholder wealth. As Volume I's insurance correlation analysis demonstrated — showing systematic correlations between insurer revenue growth and declining patient outcomes — the top five insurers deploy these extraction mechanisms with mathematical precision to optimize quarterly earnings while degrading healthcare access for millions of Americans.
The Trillion-Dollar Premium Extraction Machine
UnitedHealth Group dominates insurance extraction with $400.3 billion in 2024 revenue representing 8% growth from $371.6 billion in 2023, processing more annual revenue than the GDP of most countries while demonstrating how healthcare privatization enables unprecedented corporate scale [72]. The company's adjusted net income of $25.7 billion versus GAAP net income of $14.4 billion reveals systematic accounting manipulation that obscures true profitability by excluding costs deemed "non-representative" of operational performance [73].
The Big Five insurers—UnitedHealth Group, Elevance Health, CVS Health/Aetna, Cigna Group, and Humana—combine to control hundreds of billions in premium revenue, creating concentrated oligopoly power that determines healthcare access for over 200 million Americans. This market concentration enables coordinated extraction strategies impossible in competitive markets, from synchronized prior authorization protocols to industry-wide denial rate optimization that maximizes cost savings while minimizing regulatory scrutiny [74].
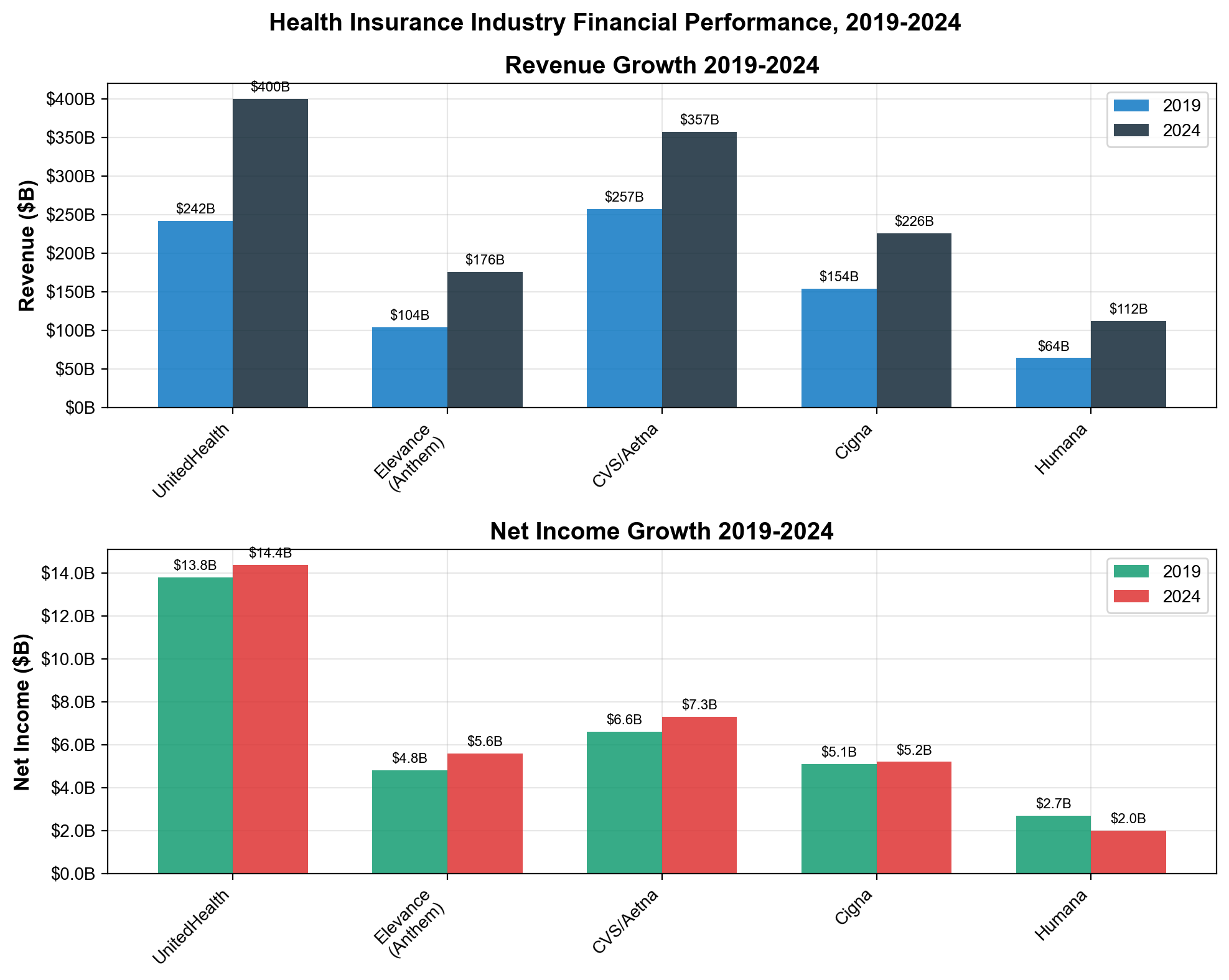
Premium revenue flows through multiple extraction layers before reaching actual medical care. Kaiser Family Foundation analysis shows private insurance medical loss ratios ranging from 85% in individual markets to 91% in Medicaid managed care, meaning 9-15% of every premium dollar flows to administrative costs, profits, executive compensation, and shareholder returns rather than patient care [75]. With total private insurance revenue of $1.644 trillion in 2024, this represents approximately $244 billion in annual extraction from premium pools that patients fund through payroll deductions, employer contributions, and direct payments.
The extraction scale becomes evident through international comparison. Americans pay $12,914 per capita annually for healthcare with inferior outcomes compared to countries spending $6,000-8,000 per capita while achieving universal coverage [76]. The $4,000-6,000 per capita differential represents pure extraction that enriches insurance shareholders while providing no superior health outcomes—making American healthcare the world's most expensive extraction mechanism disguised as medical care delivery.
Medical Loss Ratio Gaming: Making 80/20 Work for Extraction
The Affordable Care Act's Medical Loss Ratio requirements mandating 80% of individual market premiums and 85% of group market premiums fund medical care were intended to limit insurance profiteering. Instead, insurers developed sophisticated gaming mechanisms that transform MLR rules into extraction enablers through categorical manipulation, vertical integration coordination, and quality improvement redefinition [77].
The perverse incentive structure rewards higher total spending rather than cost efficiency, creating systematic pressure for premium inflation. Since insurers retain 20% of individual market premiums as gross margin, increasing premium levels generates proportionally higher absolute profits while maintaining required MLR compliance. A 20% margin on $1,000 monthly premiums yields $200 profit, while 20% of $1,500 premiums generates $300 profit—enabling 50% extraction increase through premium inflation without violating MLR requirements [78].
Expense reclassification enables systematic MLR manipulation through creative accounting that transforms administrative costs into "medical spending" through categorical redefinition. Insurance companies reclassify marketing expenditures as "member education" programs, claims processing becomes "care coordination" services, and vendor management transforms into "provider quality improvement" initiatives [79]. These accounting maneuvers allow substantial overhead costs to count toward medical loss ratios while maintaining profitable operations disguised as patient care spending.
Vertical integration creates additional MLR gaming opportunities through intercompany pricing manipulation that optimizes total enterprise profits while maintaining technical regulatory compliance. When UnitedHealthcare overpays Optum Health facilities or CVS directs patients to premium-priced CVS services, these transactions can inflate medical spending calculations while generating profits elsewhere in the integrated corporate structure [80]. This coordination enables companies to game MLR requirements while maximizing extraction across their entire healthcare ecosystem.
Quality improvement loopholes provide broad latitude for administrative cost reclassification under medical spending categories. Federal regulations define quality improvement activities vaguely, allowing insurers to count technology investments, executive compensation for "quality initiatives," consulting contracts, and vendor fees as medical expenses rather than administrative overhead [81]. These loopholes enable billions in extraction disguised as patient care investment while maintaining MLR compliance.
Prior Authorization: The $35 Billion Denial Machine
Prior authorization systems function as systematic denial machines designed to extract profits through care rationing while providing plausible medical justification for treatment restrictions. Kaiser Family Foundation analysis reveals 53 million prior authorization requests submitted by healthcare providers during 2024—approximately 1.7 requests per Medicare Advantage enrollee—with 4.1 million denials representing systematic care restriction for profit optimization [82].
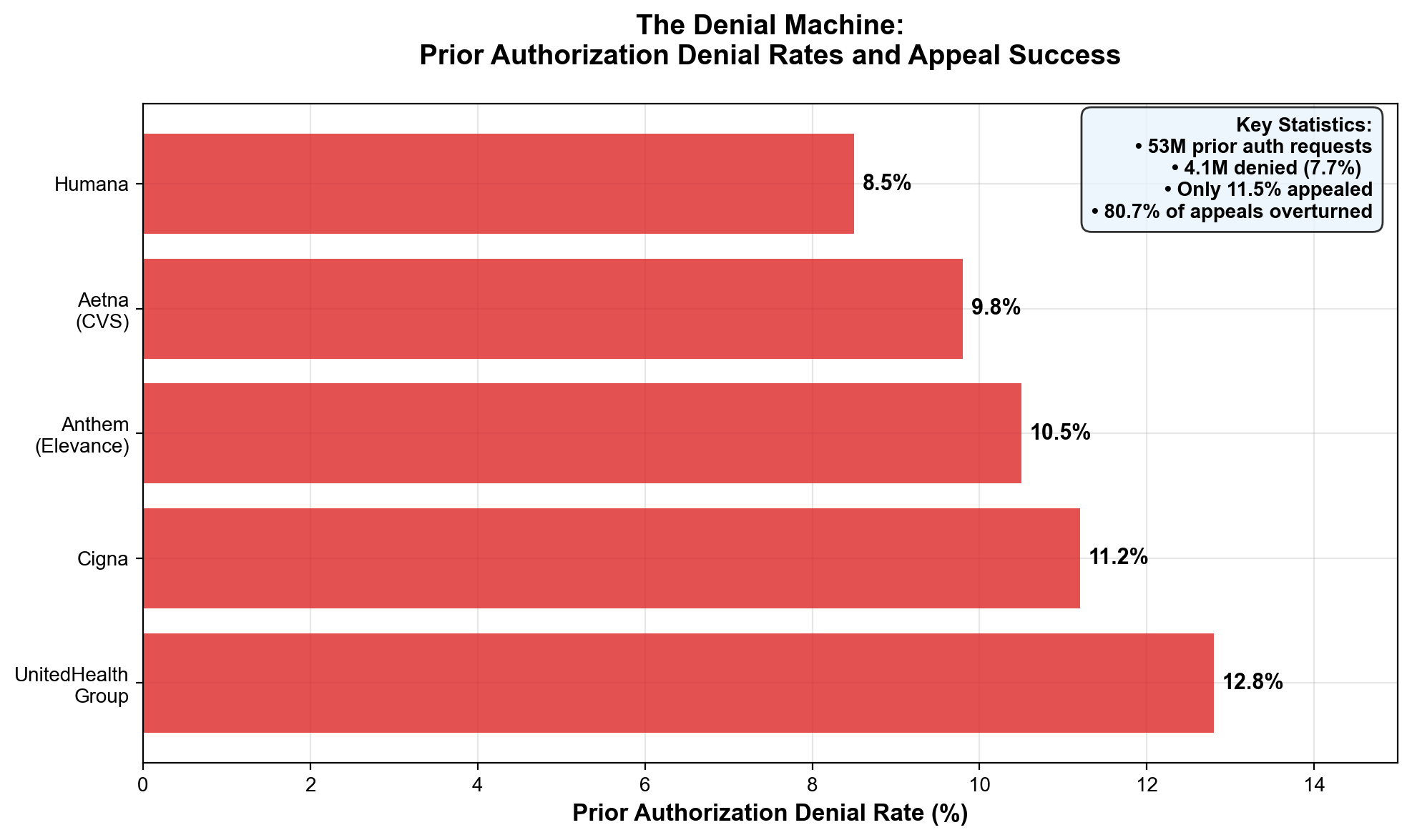
The appeal scandal exposes systematic inappropriate denials with devastating mathematical precision. Of 4.1 million denied requests, only 11.5% were appealed by patients or providers overwhelmed by bureaucratic complexity—471,500 appeals total. However, 80.7% of appeals were overturned, confirming that 380,500 denials were medically inappropriate and represented systematic care rationing for profit extraction [83]. This data proves approximately 3.3 million medically necessary services were inappropriately denied during 2024 alone, with patients forced to forgo care due to administrative barriers designed for cost reduction.
UnitedHealth Group maintains the industry's highest denial rate at 12.8%, compared to industry averages of 6.4% and competitors like Humana (5.8%) and Elevance (4.2%) [84]. This denial rate differential demonstrates systematic corporate strategies prioritizing cost reduction over appropriate care delivery, with UnitedHealth's massive scale enabling more aggressive rationing practices than smaller competitors face regulatory pressure to modify.
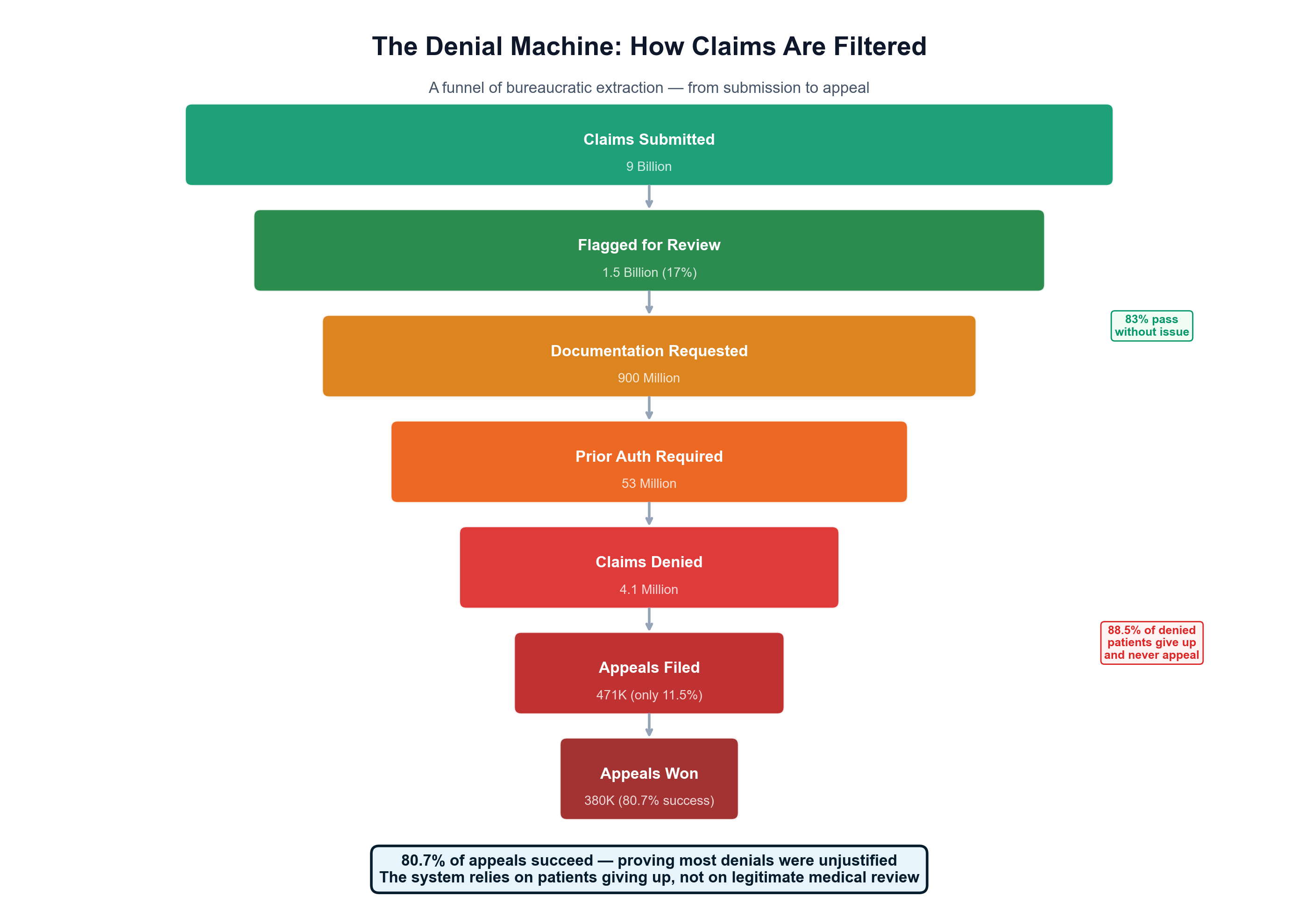
The administrative burden serves extraction purposes through physician self-censorship that reduces expensive treatment requests without explicit denials. Each prior authorization requires an average of 13.2 minutes of physician time, with complex cases demanding hours of documentation and multiple resubmissions [85]. Physicians report spending 14.5 hours weekly on prior authorization activities—equivalent to deploying 30,000+ additional physicians nationally just to manage insurer approval processes rather than deliver patient care.
Prior authorization costs exceed $35 billion annually in pure administrative waste generated by denial processes rather than care improvement. The American Medical Association estimates 33% of these costs could be eliminated through technology improvements and process standardization, potentially saving $11.7 billion annually [86]. However, insurers resist efficiency improvements because prior authorization complexity and delay serve profit maximization through care discouragement rather than genuine medical management.
Medicare Advantage: $83 Billion Annual Taxpayer Extraction
Medicare Advantage represents the insurance industry's most sophisticated extraction mechanism, generating approximately $83 billion in annual overpayments compared to traditional Medicare costs while providing inferior access through aggressive prior authorization and restricted provider networks. MedPAC analysis shows MA plans receive payments averaging 22% above traditional Medicare costs, representing systematic overpayment of taxpayer funds to private insurers who restrict care below traditional Medicare levels [87].
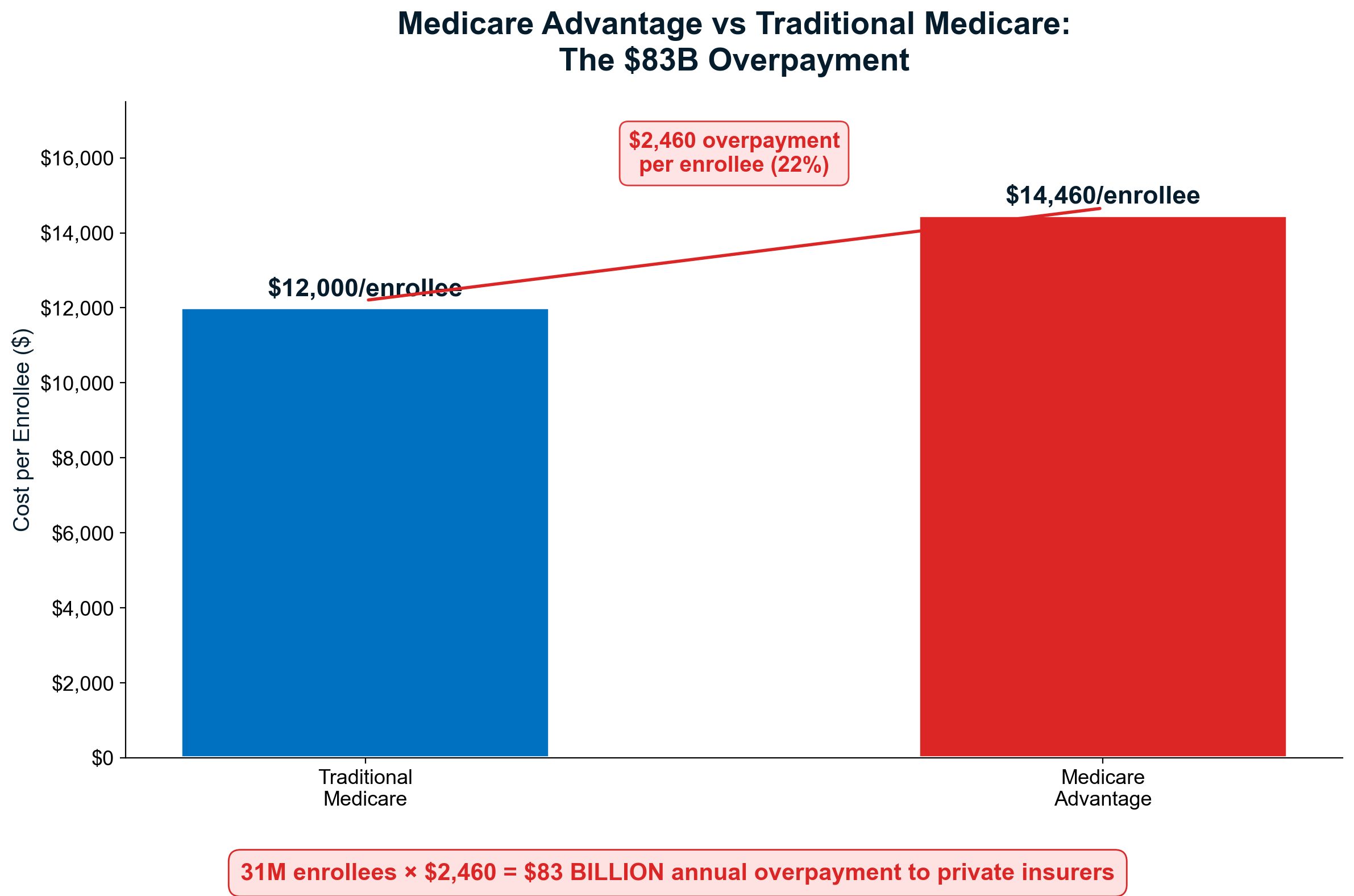
Risk adjustment gaming enables substantial overpayment extraction through systematic upcoding that makes Medicare Advantage populations appear sicker than traditional Medicare beneficiaries with identical health conditions. MA plans deploy armies of coders and nurses for home visits specifically designed to identify additional billable medical conditions, coordinate with provider networks to ensure maximum diagnostic coding, and systematically inflate risk scores that determine federal capitation payments [88]. This upcoding generates billions in additional federal payments for treating paper diagnoses that don't reflect genuine health differences.
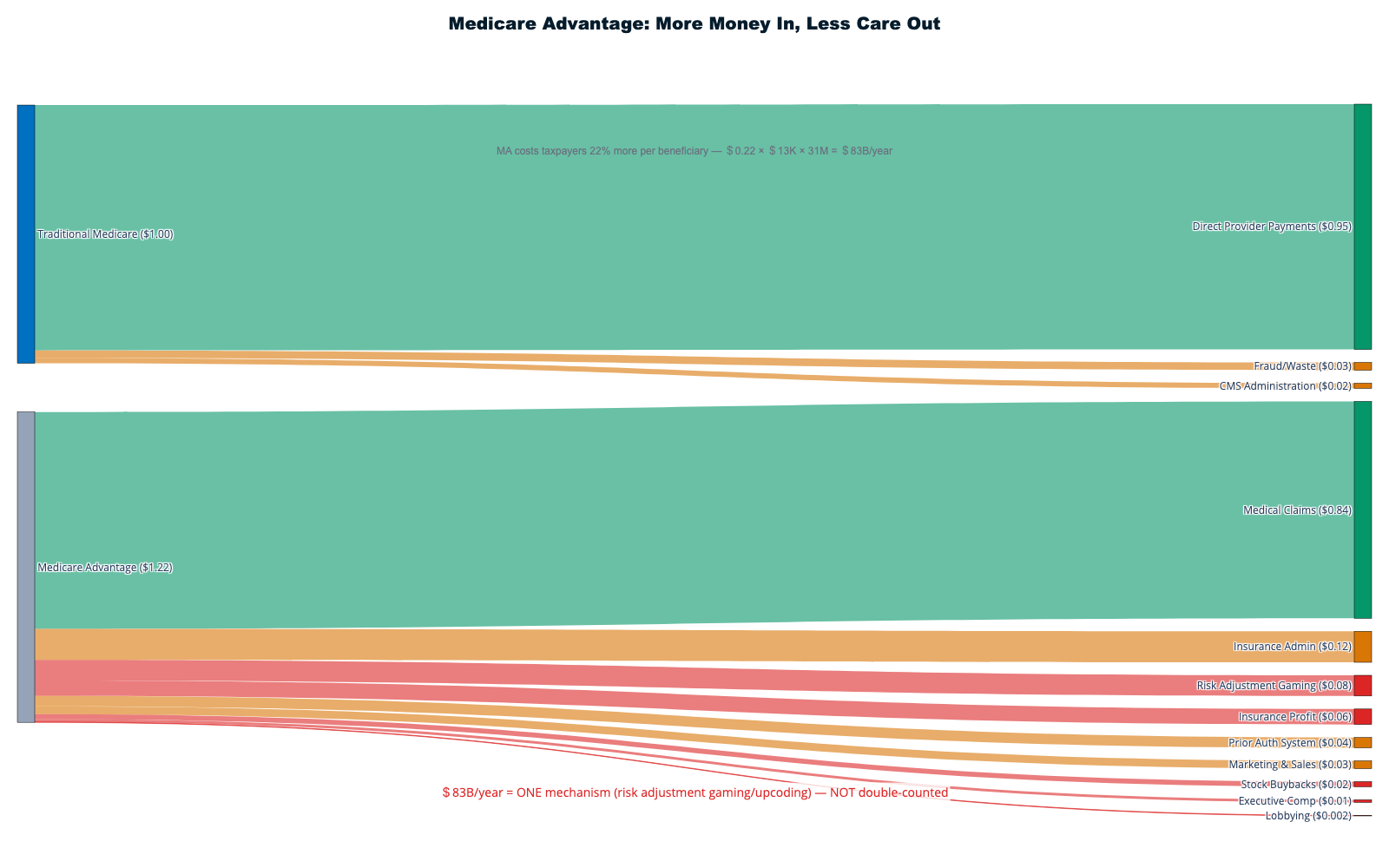
Favorable selection amplifies overpayment extraction despite MA industry claims of serving sicker populations. Medicare Advantage plans systematically attract healthier beneficiaries through benefit design emphasizing wellness programs, marketing targeting active seniors, and provider networks that discourage enrollment by patients with complex conditions. This selection bias enables plans to collect capitation payments based on average Medicare costs while serving populations requiring below-average care, generating profit margins unavailable in traditional Medicare risk pools [89].
Prior authorization as cost control generates additional extraction beyond overpayment capture. Medicare Advantage plans employ prior authorization 85 times more frequently than traditional Medicare, creating systematic barriers to expensive procedures, specialist consultations, and advanced imaging [90]. The 53 million MA prior authorization requests versus minimal traditional Medicare requirements demonstrate how privatization enables care rationing that reduces actual medical spending below capitation payments while extracting maximum profits.
The ten-year overpayment projection reaches $1.0-1.4 trillion according to Committee for Responsible Federal Budget analysis, representing the largest wealth transfer from taxpayers to private corporations in American healthcare history [91]. This extraction occurs while Medicare Advantage provides inferior benefits, restricted networks, and more complex administrative barriers compared to traditional Medicare—demonstrating how healthcare privatization increases costs while reducing access and quality.
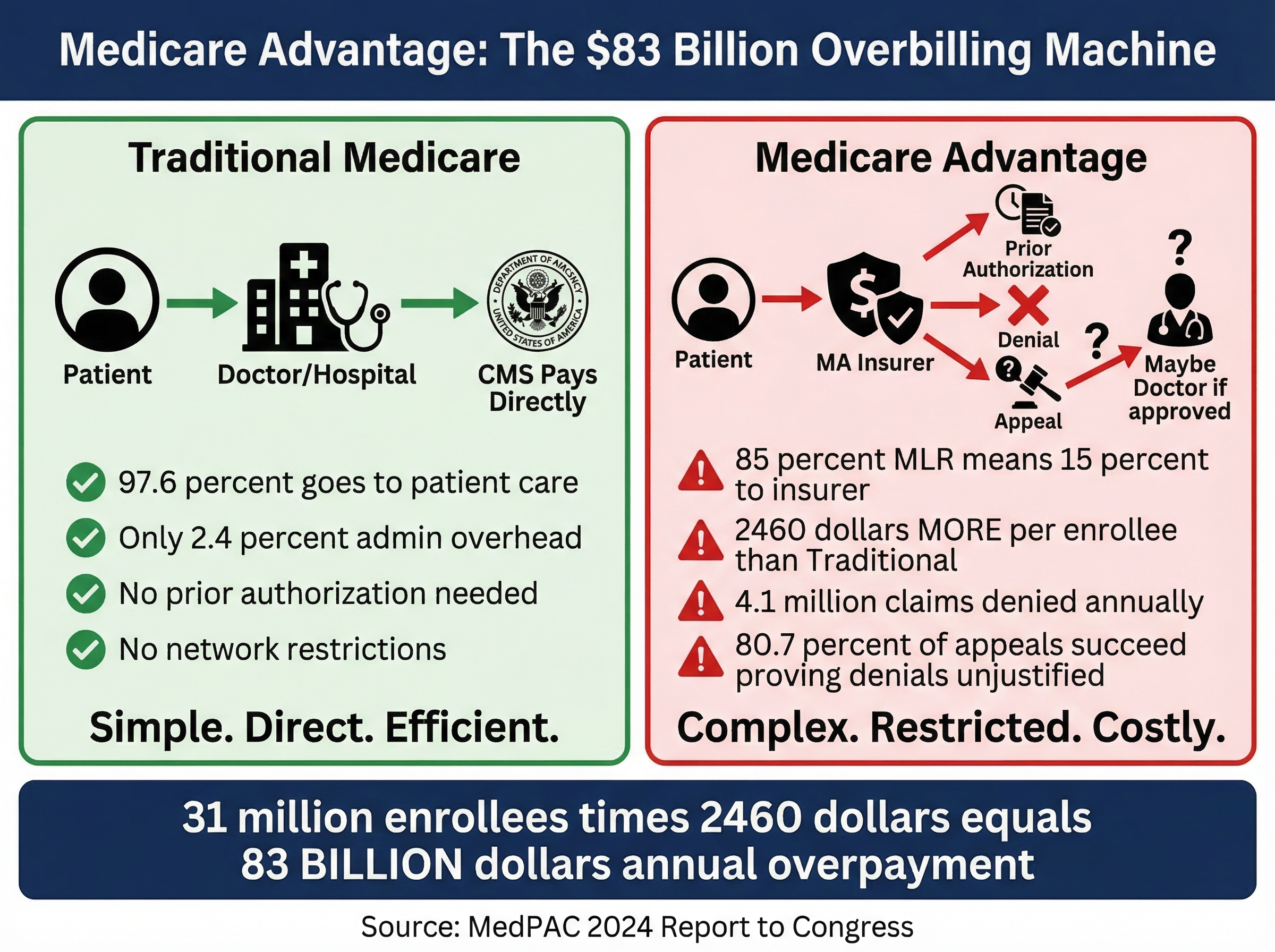
Stock Buybacks: $141 Billion Premium Extraction Pipeline
Health insurance stock buybacks provide definitive proof of extraction priorities, with companies returning $141 billion to shareholders between 2007-2022 while systematically denying medically necessary care to patients whose premiums generated those profits [92]. UnitedHealth Group exemplifies this extraction pipeline with $42+ billion in historical buybacks and $16.5 billion returned to shareholders during 2024 alone through $9 billion in stock repurchases and $7.5 billion in dividends.
The 2024 buyback acceleration demonstrates systematic extraction priorities over patient care improvement. Despite industry claims of rising medical costs and insurance market pressures, UnitedHealth increased buyback spending from $8 billion in 2023 to $9 billion in 2024 while maintaining denial rates above industry averages and opposing prior authorization reform [93]. This pattern proves "medical cost inflation" claims serve to justify premium increases rather than reflect genuine financial constraints.
Buyback timing correlates directly with denial rate optimization and cost reduction initiatives, suggesting coordination between care rationing and shareholder enrichment. Companies accelerate buybacks during periods of aggressive prior authorization implementation, provider network restrictions, and formulary limitations that reduce medical spending below premium collection levels. This correlation indicates denied patient care directly funds shareholder returns rather than supporting medical infrastructure or care quality improvements [94].
The $141 billion extraction total could have funded transformative healthcare infrastructure including medical school expansion, rural hospital preservation, primary care physician training, or premium reduction for millions of patients. Instead, this wealth flowed to shareholders through buyback programs that concentrated patient-funded profits among institutional investors while patients rationed insulin, delayed cancer treatments, and avoided emergency care due to cost barriers created by the same companies extracting their premiums [95].
Executive stock compensation creates systematic incentives for extraction maximization through buyback optimization. When CEO compensation packages include substantial stock awards and options, executives directly profit from stock price appreciation driven by buyback programs funded through care denial and administrative cost reduction. This alignment ensures management prioritizes extraction over patient care while claiming fiduciary duty to shareholders supersedes medical necessity [96].
Of the $141 billion in industry-wide stock buybacks (2007-2022), approximately 10-15% effectively funded executive stock option exercises and insider sales, with the remainder accruing to institutional investors — BlackRock, Vanguard, and State Street collectively hold 20-25% of major healthcare stocks [17] — pension funds, and retail shareholders. This concentration means the bulk of buyback value flows to the same institutional investors who sit on corporate boards and vote to approve the executive compensation packages that incentivize further extraction. The circular reinforcement between institutional ownership, board governance, executive compensation, and buyback programs creates a self-perpetuating extraction machine with no natural counterweight representing patient interests.
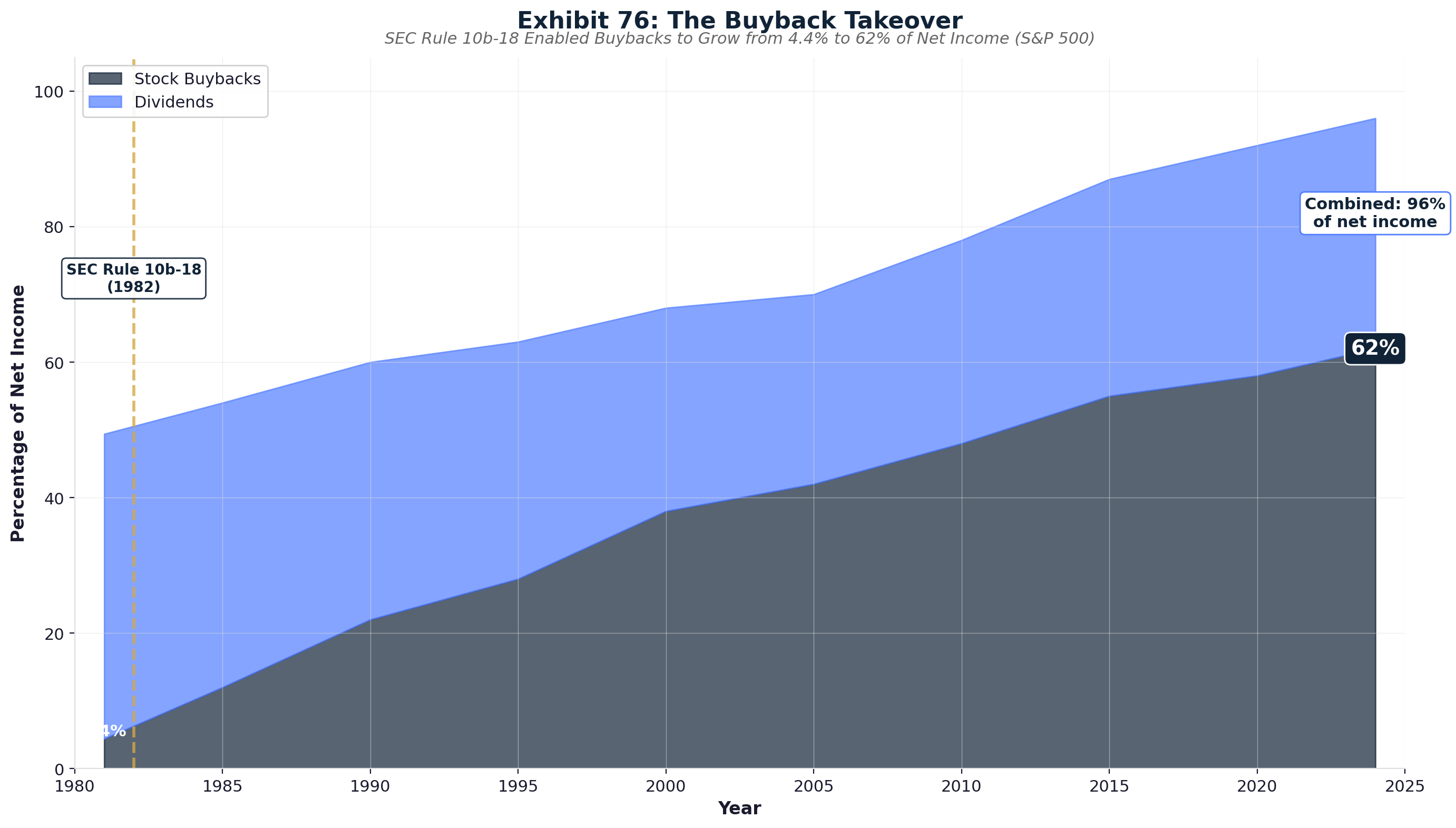
Executive Compensation: $159.4 Million for Extraction Optimization
Health insurance CEO compensation represents extraction's most visible manifestation, with top six health plan executives collecting $159.4 million combined during 2024 while their companies systematically denied medically necessary care to maximize profits for shareholder benefit [97]. UnitedHealth's Andrew Witty led extraction with $26.3 million total compensation including $17.25 million in stock awards that directly align personal wealth with company stock performance driven by extraction optimization.
Elevance Health's Gail Boudreaux received $20.5 million in 2024 compensation—370 times the median employee salary at her company, demonstrating wealth concentration enabled by healthcare extraction that would be impossible in competitive industries [98]. Executive pay growth far exceeds medical care improvement metrics, patient satisfaction scores, or population health outcomes, proving compensation reflects extraction capacity rather than healthcare delivery excellence.
Stock-based compensation structures create perverse incentives for systematic care denial and cost reduction that harm patients while enriching executives. When CEO wealth depends primarily on stock price appreciation, every denied claim and restricted service contributes to earnings growth that drives personal wealth accumulation [99]. This direct financial relationship between patient suffering and executive enrichment explains insurance industry resistance to prior authorization reform, network adequacy requirements, and genuine consumer protection measures.
Performance metrics systematically ignore patient welfare while prioritizing financial extraction optimization. CEO compensation depends on earnings per share growth, medical loss ratio manipulation, stock price performance, and shareholder return maximization—metrics that improve through care denial and administrative complexity rather than health outcome improvement or community benefit delivery [100]. This misaligned incentive structure ensures insurance leadership consistently opposes healthcare reforms that would improve patient care while reducing extraction opportunities.
The $159.4 million executive compensation total could fund thousands of additional primary care physicians, expand rural healthcare access, or reduce premiums for tens of thousands of patients. Instead, this compensation rewards systematic optimization of extraction mechanisms that deny care, inflate costs, and prioritize shareholder wealth over patient welfare—demonstrating how insurance industry financialization enables unprecedented wealth concentration through healthcare extraction rather than value creation [101].
Insurance industry financial engineering represents extraction capitalism at its most sophisticated, converting patient medical necessity into systematic profit optimization through MLR gaming, prior authorization abuse, Medicare overpayment capture, stock buyback programs, and executive compensation aligned with extraction maximization. The industry's approach to $1 trillion in annual revenue—denying 4.1 million medically necessary services while 80.7% of appeals succeed, extracting $83 billion in Medicare overpayments, returning $141 billion to shareholders through buybacks, and compensating executives $159.4 million for extraction optimization—demonstrates how insurance financialization prioritizes capital extraction over healthcare delivery. Until fundamental reforms eliminate MLR gaming opportunities, ban inappropriate prior authorization practices, end Medicare Advantage overpayments, prohibit stock buybacks from patient premium pools, and align executive compensation with patient outcomes rather than extraction maximization, the insurance industry will continue operating as systematic wealth transfer mechanism that harms patient welfare while enriching shareholders and executives through mathematical precision and bureaucratic brutality.
Chapter 8: The Stock Market Extraction Machine
The most sophisticated and lucrative healthcare extraction mechanism operates not through quarterly profit statements but through stock market capitalization that transforms patient premiums into permanent shareholder wealth concentrated among institutional investors. While public attention focuses on insurance industry profits of $20-50 billion annually, stock market appreciation creates shareholder value 10-30 times larger by capitalizing expected future extraction into immediate wealth that patients fund but never access. Healthcare stock valuations reflect mathematical calculations of extraction sustainability rather than care delivery excellence, with companies commanding premium prices when they demonstrate superior capacity for systematic patient exploitation.
The Capitalized Extraction Thesis: NPV of Human Suffering
Healthcare stock prices represent the market's assessment of each company's extraction capacity rather than medical value creation, with financial markets capitalizing the net present value of expected future extraction from patient premiums, government subsidies, and care denial optimization. When UnitedHealth Group trades at market capitalization of $265 billion, investors are mathematically valuing the company's ability to extract wealth from 50+ million Americans requiring medical care over decades [102]. Stock appreciation reflects extraction efficiency improvement rather than health outcome enhancement.
This valuation methodology explains healthcare stocks' dramatic outperformance versus broader markets with devastating mathematical precision. Health insurer stocks increased 1,032% from ACA enactment through 2024 compared to 251% S&P 500 growth—a 4:1 outperformance ratio that proves extraction as successful investment thesis [103]. Financial markets rewarded healthcare companies not for improving population health, which remains stagnant or declining, but for perfecting wealth extraction from essential human services through systematic optimization of denial rates, administrative complexity, and regulatory arbitrage.
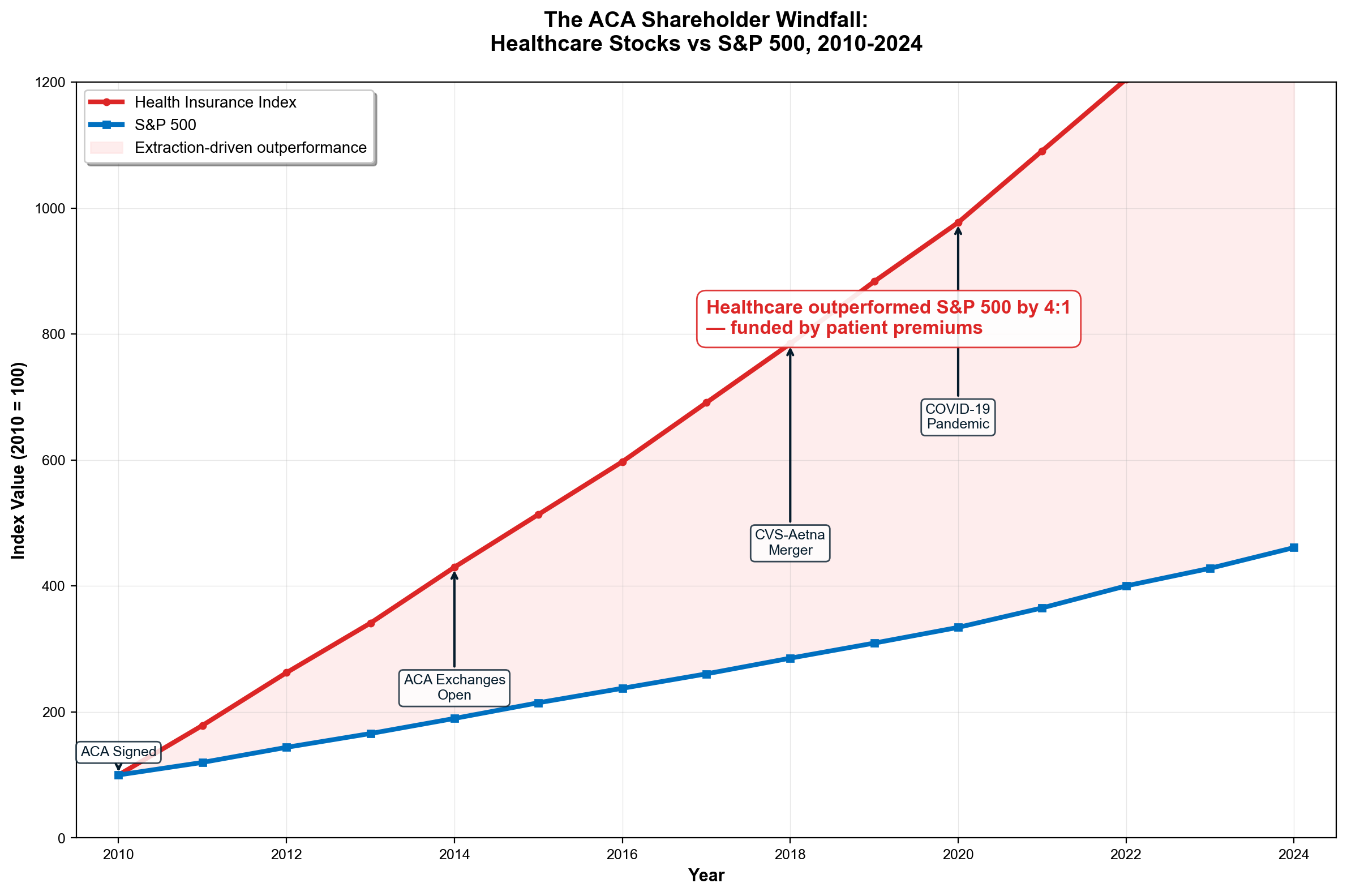
UnitedHealth Group exemplifies this capitalization process through $226 billion in shareholder wealth creation funded entirely by patient premiums and taxpayer subsidies. The company's market capitalization expanded from approximately $39 billion in 2010 to $265 billion by 2026, representing wealth creation equal to the GDP of Finland while occurring during periods of systematic care denial, prior authorization abuse, and administrative cost inflation [104]. This appreciation demonstrated market validation of extraction optimization rather than medical excellence or patient satisfaction improvement.
The extraction-capitalization relationship operates through quarterly earnings calls where executives explicitly discuss cost reduction initiatives, prior authorization "efficiencies," and administrative "optimization" that translate directly into stock price appreciation. When UnitedHealth reports medical loss ratio improvements through prior authorization implementation, stock prices increase immediately as investors capitalize expected future extraction into present shareholder value [105]. Patient suffering becomes investment return through mathematical precision that would be criminal in other industries.
The ACA Shareholder Windfall: $1.4 Trillion in Extraction Enablement
The Affordable Care Act created the largest transfer of wealth from taxpayers and patients to private shareholders in American history by establishing regulatory frameworks that guaranteed extraction revenue while socializing industry risks. The individual mandate required Americans to purchase private insurance or pay tax penalties, creating captive customer bases that eliminated competitive market risks while enabling systematic extraction from legally coerced consumers [106].
Medicaid expansion channeled $126 billion annually through private managed care plans while marketplace subsidies added $92 billion in fiscal 2023, totaling $218 billion in government-guaranteed revenue flowing to private insurers [107]. This subsidization transformed health insurance from competitive market activity to regulated utility status with assured cash flows, enabling unprecedented stock valuations that reflected reduced risk premiums and extraction sustainability.
Financial markets immediately capitalized this risk reduction into permanent shareholder wealth through stock appreciation that dwarfed any actual operational improvements. The ACA eliminated customer acquisition costs through mandates while providing federal subsidies that guaranteed profit margins regardless of medical spending efficiency. Unlike legitimate utility companies facing rate regulation, health insurers captured utility-level financial security while maintaining pricing power through Medical Loss Ratio gaming and vertical integration strategies [108].
The human cost of this wealth transfer becomes visible through direct comparison of shareholder gains versus patient outcomes. While UnitedHealth shareholders captured $226 billion in market appreciation, the company maintained industry-leading denial rates that prevented medically necessary care for millions while charging premium increases exceeding medical inflation [109]. Each denied claim contributed marginally to quarterly earnings that compounded into massive stock appreciation, creating direct mathematical relationships between patient suffering and shareholder enrichment.
Medicare Advantage overpayments exemplify ACA wealth transfer mechanisms through systematic extraction from taxpayer-funded healthcare programs. Private insurers receive $83 billion annually in overpayments compared to traditional Medicare costs while providing inferior care through prior authorization restrictions and network limitations [110]. These overpayments flow directly to stock appreciation as investors capitalize guaranteed government revenues that exceed medical spending obligations.
Stock Buybacks: The $141 Billion Premium Conversion Machine
Stock repurchase programs represent the most direct mechanism for converting patient premiums into concentrated shareholder wealth, with health insurers returning $141 billion to shareholders between 2007-2022 through buyback programs that literally transform medical necessity into capital extraction [111]. UnitedHealth exemplifies this conversion pipeline through $42 billion in stock buybacks since 2018, with $9 billion repurchased during 2024 alone while maintaining industry-leading denial rates.
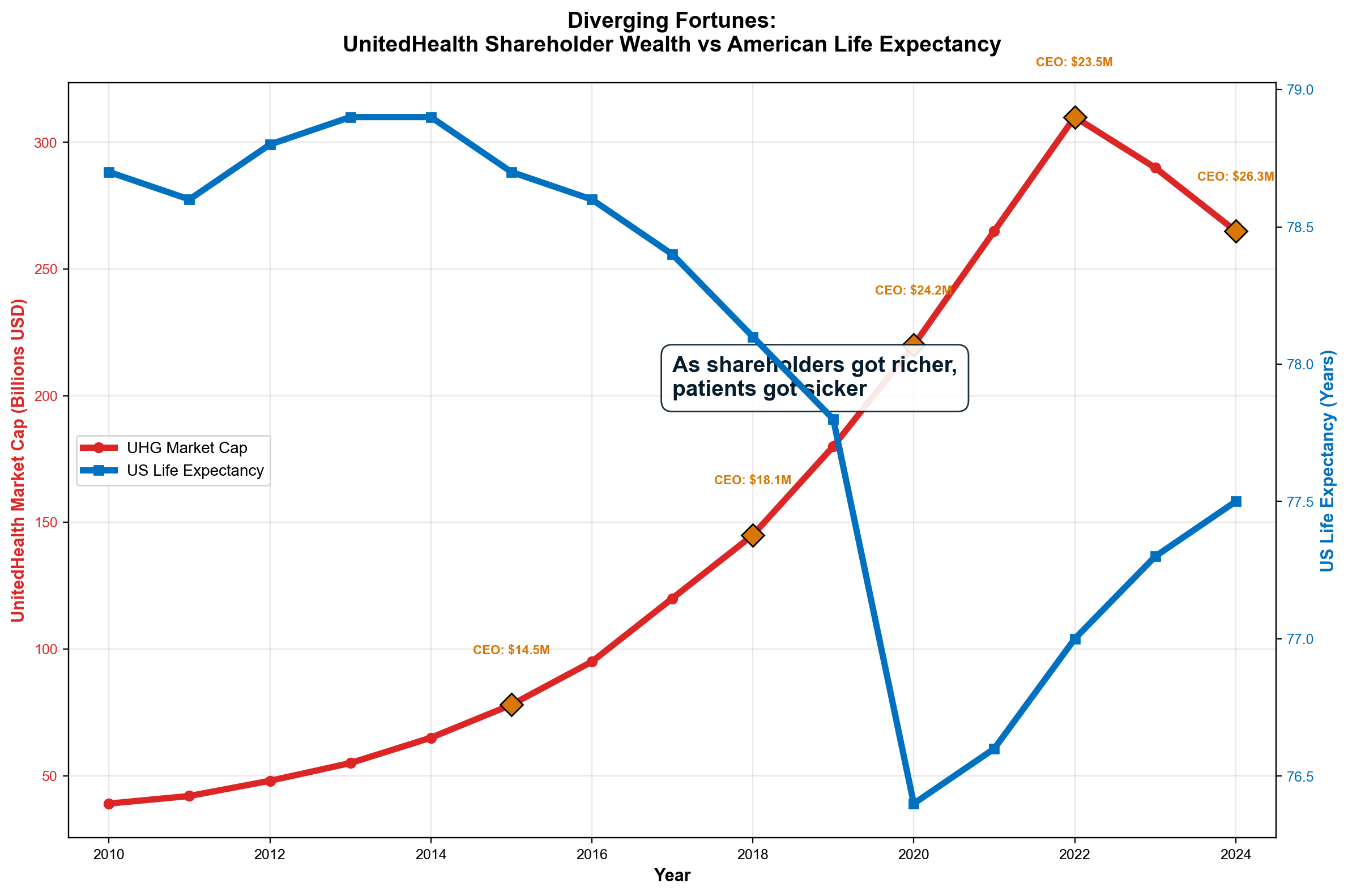
The buyback mechanism creates self-reinforcing wealth concentration cycles that operate independently of healthcare delivery improvement. Share repurchases reduce outstanding share counts, automatically increasing earnings per share without operational enhancement. Higher EPS drives stock price appreciation that attracts additional investment capital while enabling larger future buyback programs funded by continued patient premium extraction [112]. The cycle accelerates as companies optimize extraction to fund buybacks that drive valuations higher, creating positive feedback loops between patient harm and shareholder benefit.
Executive compensation structures ensure buyback programs operate with mathematical efficiency for wealth extraction optimization. UnitedHealth CEO Andrew Witty's 2024 compensation included $21.5 million (82%) in stock-based awards, creating direct personal incentives to maximize stock price appreciation through buyback programs funded by premium extraction [113]. When executives own substantial equity positions, buyback programs simultaneously increase personal wealth while reducing corporate cash available for premium reduction or care improvement.
The extraction-buyback pipeline operates through quarterly coordination between cost reduction initiatives and capital return announcements. Companies accelerate share repurchases during periods of aggressive prior authorization implementation, provider payment reductions, and formulary restrictions that generate cash flow "improvements" through systematic care rationing [114]. This coordination ensures that every dollar extracted from patient care flows efficiently to shareholder wealth concentration rather than healthcare system improvement.
Double Extraction Spiral: Acquisition-Funded Empire Building
Healthcare companies operate double extraction spirals where traditional profit extraction funds stock market appreciation that attracts investment capital enabling additional acquisition-based expansion of extraction capacity. UnitedHealth's vertical integration strategy demonstrates this multiplication effect: insurance profits fund acquisitions of provider networks, PBM operations, and claims processing companies that generate additional extraction opportunities while creating stock appreciation from growth expectations [115].
The spiral accelerates through debt financing that leverages stock appreciation into acquisition capacity exceeding cash flow generation. When UnitedHealth's stock price increases, borrowing capacity expands correspondingly, enabling larger acquisitions funded through debt that future extraction must service. CVS's $69 billion Aetna acquisition exemplifies this mechanism: stock price appreciation provided collateral for debt financing that enabled vertical integration creating additional extraction capacity through pharmacy-insurance coordination [116].
Private equity involvement amplifies the double extraction spiral through financial engineering that optimizes healthcare delivery for stock market performance rather than patient outcomes. PE firms acquire hospital systems, physician practices, and specialty providers, implementing operational changes that prioritize EBITDA improvement for exit valuation maximization while degrading care quality through staffing cuts and service elimination [117]. The resulting extraction optimization creates stock appreciation for portfolio companies while establishing market precedents that publicly traded competitors must match to maintain investment returns.
The acquisition-extraction cycle compounds through economies of scale in denial management, administrative cost optimization, and regulatory capture that enable larger companies to extract more efficiently than smaller competitors. UnitedHealth's massive scale allows deployment of sophisticated prior authorization systems, data analytics for denial optimization, and political influence that smaller insurers cannot replicate, creating systematic competitive advantages through extraction capacity rather than care delivery excellence [118].
Annual Shareholder Wealth Creation: $300-600 Billion Scale
Conservative estimates indicate healthcare sector shareholder wealth creation reaches $300-600 billion annually through stock appreciation mechanisms that dramatically exceed reported industry profits while representing pure extraction from patients and taxpayers. UnitedHealth alone generated shareholder value exceeding $50-100 billion during peak appreciation years, demonstrating extraction multiples far beyond operational improvements or medical advancement [119].
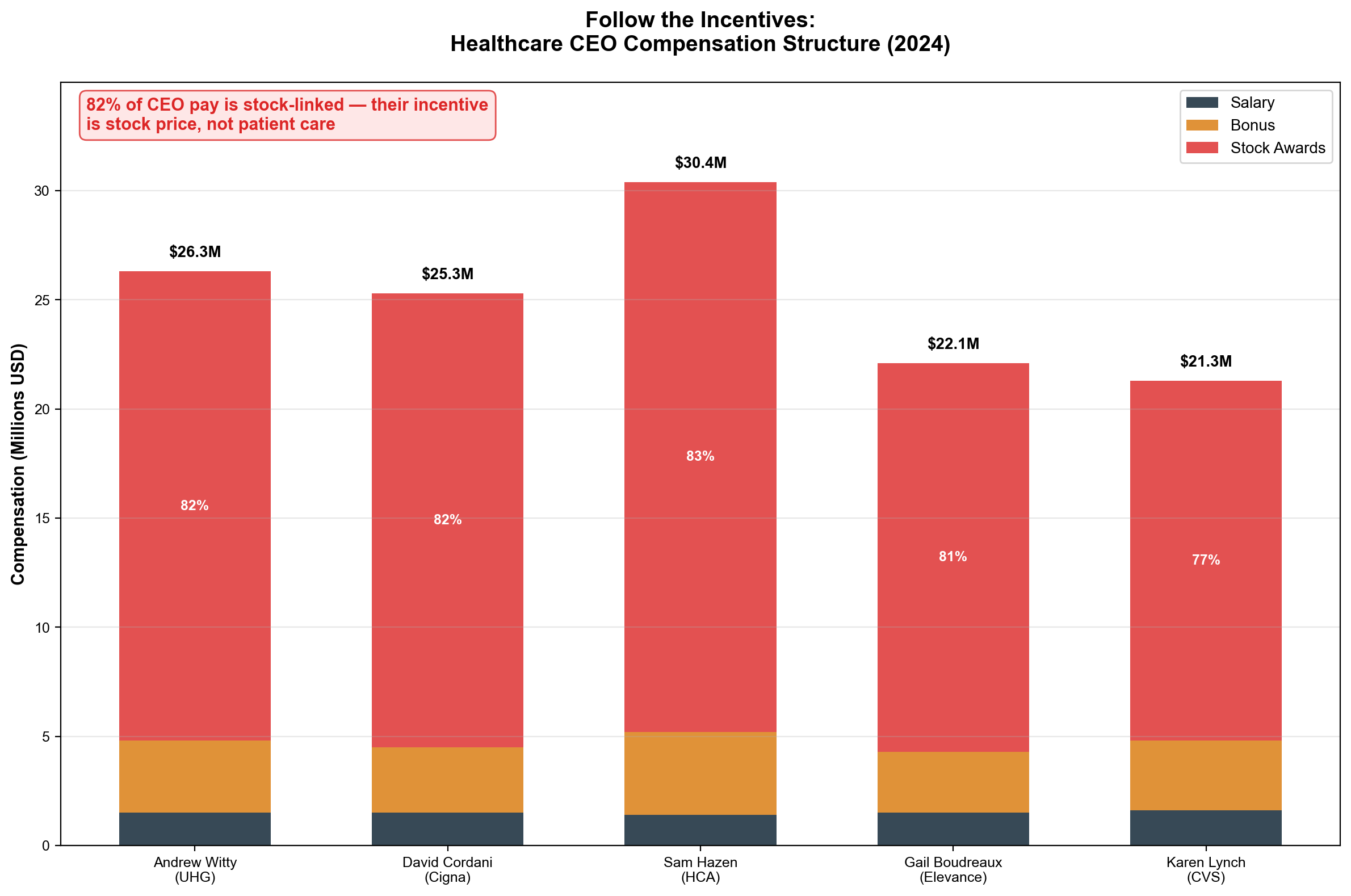
This wealth creation disparity reveals healthcare extraction's fundamental injustice through mathematical comparison of value flows. Patients experiencing medical necessity provide guaranteed revenue streams that enable stock appreciation captured exclusively by shareholders who contribute nothing to care delivery. A diabetic patient paying $400 monthly for insulin helps fund pharmaceutical company stock appreciation that enriches investors while the patient faces rationing decisions due to extraction-driven cost inflation [120]. Patients provide guaranteed revenue but receive zero equity participation in wealth creation their medical necessity enables.
The institutional concentration of healthcare wealth demonstrates systematic transfer from individual patients to concentrated capital. BlackRock, Vanguard, and State Street maintain controlling interests in virtually every major healthcare company, capturing extraction-driven appreciation across entire healthcare portfolios while patients fund this wealth concentration through premium payments and tax subsidies [121]. This common ownership structure enables coordinated extraction strategies that maximize total portfolio returns rather than competitive pricing between individual companies.
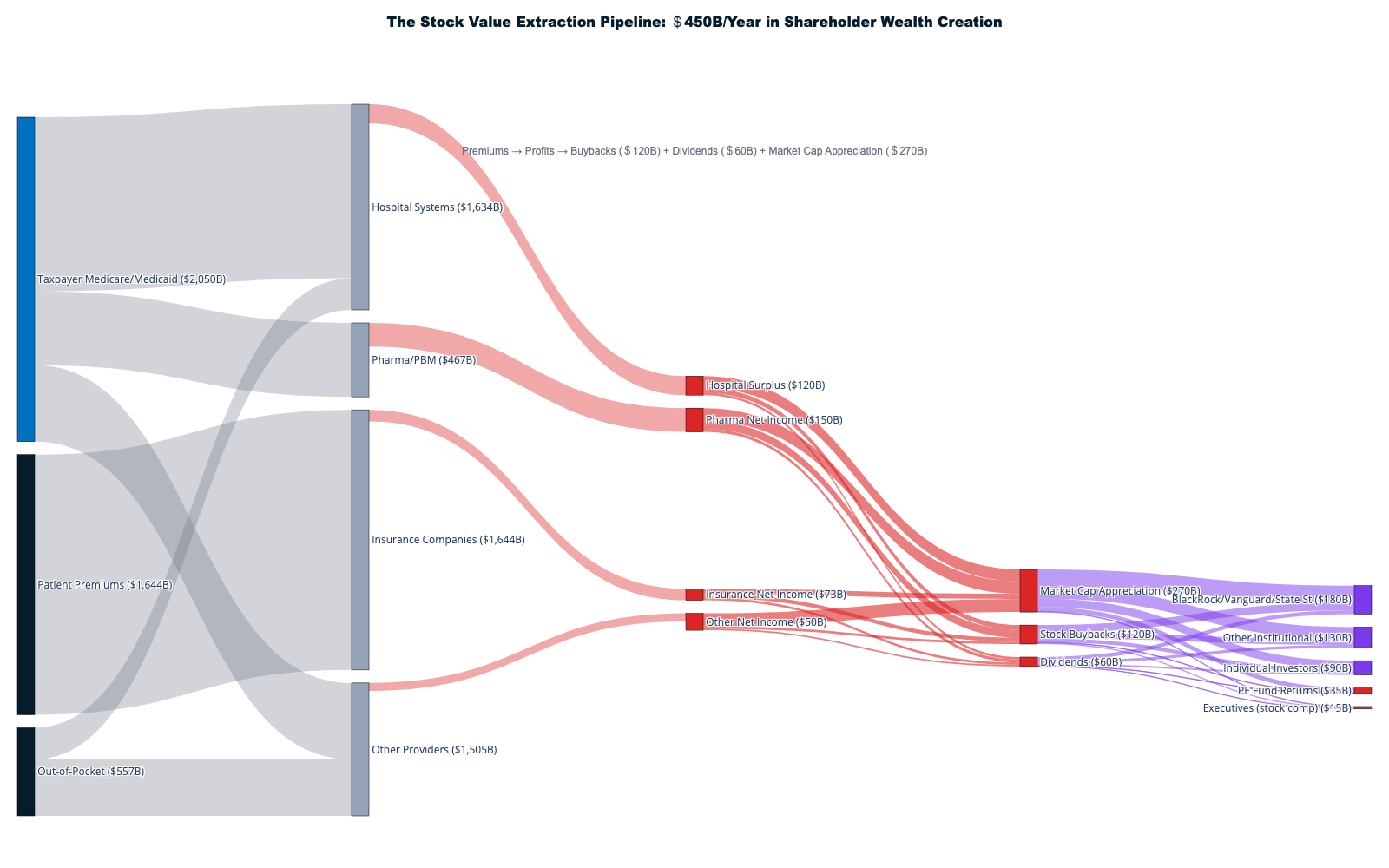
Annual extraction calculations prove stock market mechanisms capture 5-15 times more patient resources than traditional profit recognition. When UnitedHealth reports $25 billion in net income while generating $50-100 billion in annual shareholder value creation through stock appreciation, the total extraction exceeds apparent financial statements by factors that reveal the true scale of healthcare financialization [122]. Stock market wealth creation represents the primary extraction mechanism rather than secondary effect of healthcare operations.
International Comparison: $4,000 Per Capita Pure Extraction
International healthcare spending comparison provides definitive proof that American stock market extraction represents policy choice rather than medical necessity. Countries with single-payer systems achieve superior health outcomes at costs $4,000-6,000 per capita below American spending while eliminating healthcare stock market extraction entirely [123]. Canada spends 11% of GDP achieving universal coverage with zero healthcare stock appreciation, while America spends 17.8% generating hundreds of billions in annual shareholder value creation.
The 6.8 percentage point GDP difference represents pure extraction that flows to stock market investors rather than patient care delivery. This differential equals approximately $1.7 trillion annually in resources that could fund universal coverage, medical infrastructure expansion, or healthcare cost elimination while achieving superior population health outcomes [124]. Instead, this wealth flows to shareholders through stock appreciation mechanisms that enrich institutional investors while providing inferior medical access compared to efficiently organized healthcare systems.
Single-payer implementation would eliminate stock market extraction while redirecting resources toward actual medical care delivery, potentially reducing total healthcare costs by 30-40% while expanding access and improving outcomes. The resistance to single-payer systems reflects protection of extraction opportunities rather than concern for healthcare quality or access, with industry opposition correlating directly with threatened stock market wealth rather than patient welfare considerations [125].
Executive Incentive Alignment: 82% Stock Compensation
Healthcare executive compensation structures create systematic incentives for extraction maximization through stock-based payments that directly align management wealth with stock price appreciation driven by patient care reduction. The top six health plan CEOs received combined compensation of $159.4 million during 2024, with 80%+ delivered through stock awards and options that increase in value through extraction optimization rather than healthcare improvement [126].
UnitedHealth CEO Andrew Witty's $26.3 million compensation included $21.5 million (82%) in stock-based payments that create direct personal financial incentives to maximize stock price through cost reduction, denial optimization, and extraction efficiency rather than patient satisfaction or health outcomes [127]. This compensation structure ensures executives personally profit from systematic care denial while claiming fiduciary responsibility to shareholders supersedes medical ethics or patient welfare.
The misalignment between executive incentives and healthcare delivery creates systematic pressure for extraction maximization that operates independently of patient needs or community health requirements. When CEO wealth depends primarily on stock appreciation driven by quarterly earnings growth, every aspect of healthcare operations becomes optimization opportunity for cost reduction rather than care improvement [128]. This fundamental misalignment explains healthcare industry resistance to reforms that would improve patient care while reducing extraction opportunities.
Stock market extraction represents healthcare financialization's ultimate achievement: converting human medical necessity into permanent shareholder wealth while socializing costs and privatizing gains through mathematical precision. Healthcare stock appreciation of 1,032% versus 251% S&P 500 growth proves market recognition of extraction capacity rather than care delivery value. UnitedHealth's $226 billion wealth creation, industry-wide $141 billion in stock buybacks, ACA-enabled revenue guarantees worth $218 billion annually, and executive compensation aligned with extraction optimization demonstrate how stock market mechanisms systematically transfer wealth from patients to shareholders while degrading healthcare access and quality. Until healthcare reform addresses stock market incentives that reward extraction over care delivery, patient premiums will continue funding Wall Street enrichment rather than medical healing through the most sophisticated wealth concentration mechanism in modern economic history.
Chapters 9-12: The Machinery of Financial Extraction
Chapter 9: Pharmaceutical Extraction
The American pharmaceutical system has perfected the art of transforming life-saving medications into wealth extraction opportunities through monopoly extension, vertical integration, and rebate schemes that prioritize financial engineering over patient access. With Americans paying 3-5 times more for identical medications compared to peer countries, pharmaceutical extraction represents one of healthcare's most visible yet sophisticated profit maximization strategies [1].
The Insulin Execution Model
Insulin offers the starkest example of pharmaceutical extraction mechanics. A medication discovered nearly 100 years ago, manufactured for $2-5 per vial, costs American patients $300-400 monthly through a coordinated scheme involving three insulin manufacturers controlling 90% market share, three pharmacy benefit managers processing 80% of prescriptions, and a patent evergreening strategy that prevents generic competition [2].
The extraction pathway operates through calculated market manipulation. When Eli Lilly increased insulin prices by 1,200% between 1999-2017, Novo Nordisk and Sanofi matched these increases within months, demonstrating coordinated pricing rather than competitive market forces. The synchronized price increases generated billions in additional revenue while forcing an estimated 1.3 million diabetics to ration insulin—a lethal cost-cutting behavior that directly correlates with pharmaceutical profit maximization [3].
Patent manipulation extends insulin monopolies indefinitely through "evergreening"—making minor modifications to existing formulations that reset patent timers without meaningful therapeutic improvement. Insulin lispro (Humalog) has received 74 patent applications covering devices, formulations, and manufacturing processes that collectively extend market exclusivity until 2028, despite the core medication being decades old [4]. This legal strategy transforms a publicly-funded discovery into permanent private wealth extraction.
The three-company insulin oligopoly demonstrates coordinated extraction through follow-the-leader pricing. When any manufacturer announces increases, competitors implement identical changes within 30-60 days. This price shadowing eliminates competitive pressure while ensuring maximum revenue extraction from captive diabetic patients who require insulin to survive [5].
The PBM Rebate Laundering Scheme
Pharmacy Benefit Managers have created the most sophisticated drug pricing manipulation system in American commerce through rebate schemes that inflate list prices while extracting value from patients and small pharmacies. The "Big Three" PBMs—CVS Caremark, OptumRx (UnitedHealth), and Express Scripts (Cigna)—control 80% of prescription processing while generating $100+ billion annually through spread pricing, rebate retention, and vertical integration conflicts [6].
The rebate system operates as legalized money laundering. Pharmaceutical manufacturers increase list prices by 200-400% above production costs, then pay rebates of 50-60% to PBMs who "negotiate" these inflated prices downward. Patients without insurance pay full list price, while insured patients pay copays calculated on the pre-rebate amount. The PBM retains 15-30% of rebates as "administrative fees" while passing remainder to health plans as apparent savings [7].
This creates perverse incentives where higher list prices generate larger absolute rebate dollars for PBMs. A medication with $200 list price generating $100 rebate produces $15-30 PBM revenue, while $300 list price generating $150 rebate produces $22.50-45 revenue. PBMs profit by encouraging list price inflation while patients bear increased out-of-pocket costs calculated on inflated baseline prices [8].
Formulary manipulation completes the extraction cycle. PBMs create preferred drug lists that favor medications offering highest rebate payments rather than optimal clinical outcomes. Lower-cost alternatives receive unfavorable formulary placement, forcing patients toward higher-rebate medications that benefit PBM financial performance while increasing patient costs and potentially compromising therapeutic outcomes [9].
The vertical integration between PBMs, insurers, and pharmacy chains eliminates competitive oversight. CVS owns Caremark PBM and CVS pharmacy chain, creating incentives to steer patients toward CVS pharmacies while maximizing rebate extraction. UnitedHealth's Optum division combines PBM operations, insurance, and clinic ownership, enabling coordinated extraction across the pharmaceutical supply chain [10].
International Price Comparison: The American Tax
Identical medications demonstrate systematic American price inflation when compared to international markets under price control systems. The United States consistently ranks highest in pharmaceutical pricing despite funding much of the basic research through National Institutes of Health grants and university collaborations [11].
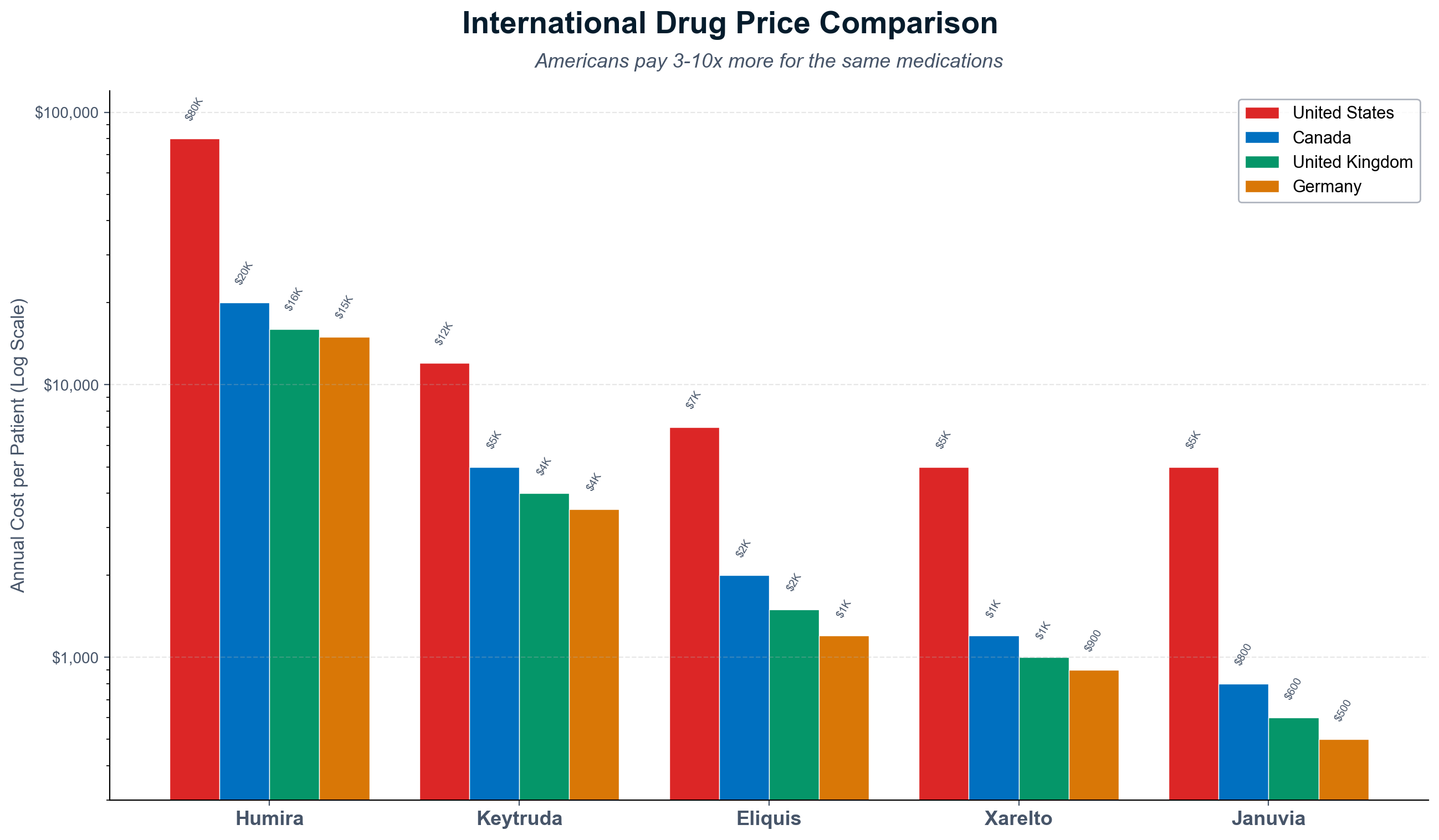
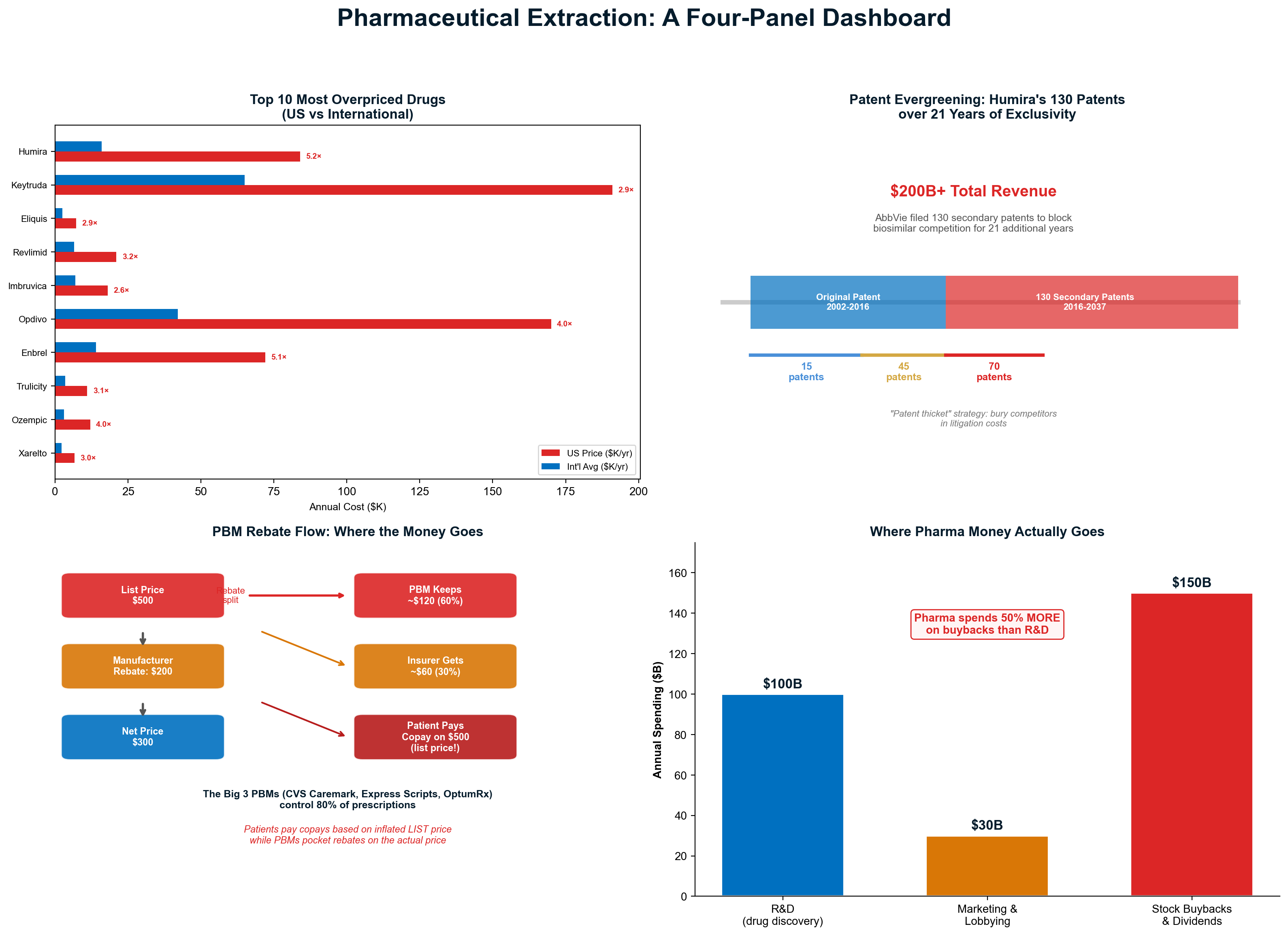
Humira exemplifies international pricing arbitrage. American patients pay $5,174 annually for the arthritis medication that costs $822 in Germany, $1,123 in the United Kingdom, and $1,749 in Australia. The active ingredient costs approximately $50 annually to manufacture, meaning American pricing includes 10,000%+ markup compared to production costs [12].
Cancer medications reveal the human cost of pharmaceutical extraction. Keytruda costs American patients $12,500 monthly compared to $2,300 in Germany and $3,100 in the United Kingdom. The price differential forces American cancer patients to choose between financial bankruptcy and life-saving treatment—a choice that exists nowhere else in the developed world [13].
The differential demonstrates extraction rather than research recovery. Pharmaceutical companies claim higher American prices fund innovation, yet most basic research occurs in university settings funded by taxpayers through NIH grants. Companies purchase or license university discoveries, then extract maximum revenue through patent monopolies that American patients subsidize far above research costs [14].
Government purchasing demonstrates alternative pricing possibilities. The Veterans Administration negotiates 40-50% lower pharmaceutical costs than Medicare Part D by using formulary restrictions and bulk purchasing leverage. When government acts as monopsony purchaser, pharmaceutical companies accept dramatically lower margins while maintaining profitability [15].
Market Manipulation Through Artificial Scarcity
Pharmaceutical companies systematically create artificial scarcity through production restrictions, distribution limitations, and regulatory manipulation that enables emergency pricing. The EpiPen scandal exemplifies scarcity-driven extraction where Mylan increased prices by 500% while acquiring patents, lobbying for regulatory requirements, and restricting generic competition [16].
Production manipulation creates shortage-driven pricing opportunities. Companies deliberately constrain manufacturing capacity for generic medications with limited producers, enabling price spikes when competitors exit markets. Daraprim increased from $13.50 to $750 per pill when Turing Pharmaceuticals acquired exclusive rights and restricted production despite minimal manufacturing complexity [17].
Distribution restrictions prevent competitive pressure through exclusive pharmacy networks and specialty distribution requirements. Manufacturers designate certain medications as "specialty" requiring specific handling protocols that limit distribution to company-controlled pharmacy networks. This artificial restriction eliminates competitive pressure while enabling premium pricing for medications requiring no special handling [18].
The orphan drug loophole demonstrates regulatory capture enabling extraction. Companies acquire rights to medications for rare diseases, then receive FDA exclusivity protection and tax incentives intended to encourage research for underserved populations. These protections are applied to existing medications with minimal modification, enabling extraction from vulnerable patient populations through regulatory arbitrage [19].
Patent System Abuse and Evergreening
The pharmaceutical patent system has been weaponized to extend monopoly protection far beyond original therapeutic innovation through evergreening strategies that make trivial modifications to existing medications. These tactics transform limited-time patents into permanent extraction mechanisms while preventing competitive generic entry [20].
Secondary patent manipulation extends exclusivity through device patents, combination therapy protection, and manufacturing process exclusivity that surrounds core medications with dozens of additional intellectual property barriers. AstraZeneca's Nexium received 49 secondary patents covering capsule composition, manufacturing processes, and combination therapies that extended exclusivity until 2014 despite core medication discovery occurring in the 1980s [21].
Pay-for-delay agreements represent direct bribery to prevent generic competition. Brand pharmaceutical companies pay generic manufacturers $100+ million annually to delay competitive entry despite successful generic development. The Supreme Court ruled these agreements presumptively anti-competitive, yet enforcement remains minimal while extraction continues [22].
The regulatory approval process enables delay tactics through citizen petitions and administrative challenges that postpone generic entry. Brand companies file regulatory objections requiring FDA review and response, delaying generic approval by months or years. Each delay month generates tens or hundreds of millions in continued monopoly revenue [23].
Authorized generic strategies eliminate competitive pressure when exclusivity expires. Brand companies launch their own "generic" versions at slightly lower prices, capturing generic market share while maintaining higher margins than independent generic competitors. This strategy extends effective monopoly control beyond patent expiration [24].
The Taxpayer Pays Twice: Patent Monopolies on Publicly Funded Research
Perhaps the most egregious extraction mechanism in pharmaceutical pricing is the granting of monopoly patent protection to drugs developed substantially with taxpayer funding. A landmark 2020 INET study found that NIH funding contributed to published research associated with every one of the 356 drugs approved by the FDA between 2010 and 2019, representing over $230 billion in cumulative public investment. [186] The Bayh-Dole Act of 1980 allows universities to patent federally funded discoveries, creating a pipeline through which public research transfers to companies charging monopoly prices.
Gilead Sciences' hepatitis C drug Sovaldi, developed substantially with federal research, launched at $84,000 per treatment course — despite production costs of $100-200. [186] The Bayh-Dole Act includes "march-in rights" allowing government to license patents when drugs aren't available on "reasonable terms." In 44 years, NIH has never exercised these rights despite repeated petitions. [187] In December 2023, the Biden administration established that march-in rights could be triggered by unreasonable pricing — a policy immediately challenged by industry and subsequently abandoned by the Trump administration.
Chapter 10: Private Equity — The Extraction Playbook
Private equity has systematically transformed American healthcare from mission-driven institutions into financial engineering platforms through the "Buy → Leverage → Cut → Extract fees → Exit (or collapse)" playbook. With over $800 billion in healthcare assets under management and 30,000+ healthcare deals since 2000, PE has perfected wealth extraction regardless of portfolio company survival or patient outcomes [25]. The most rigorous documentation of this transformation comes from Eileen Appelbaum (CEPR) and Rosemary Batt (Cornell University) in their series of Institute for New Economic Thinking working papers. Their 2020 INET Working Paper No. 118, "Private Equity Buyouts in Healthcare: Who Wins, Who Loses?", documented how hospital chains "faced major challenges in meeting loan obligations accumulated through LBOs of add-on acquisitions; and local health markets experienced instability caused by the pressure of high levels of debt." [14] Their 2019 paper demonstrated the causal link between PE ownership and surprise billing: Blackstone and KKR cornered 30% of the physician staffing market by 2013, after which surprise billing rose from 32.3% to 42.8% of ER visits. [15]
The Cerberus Steward Destruction Template
Cerberus Capital's ownership and systematic destruction of Steward Health Care provides the definitive case study of private equity healthcare extraction methodologies. Over a decade of ownership, Cerberus extracted $1.3+ billion through management fees, dividend recapitalizations, and real estate sales while accumulating $9 billion in system debt before abandoning the collapsed system to taxpayers [26].
The extraction timeline reveals PE's systematic approach to wealth transfer. Cerberus acquired Caritas Christi Health Care in 2010 for $896 million, immediately implementing the standard playbook: load with debt, extract cash, cut costs, engineer financial statements for maximum fee generation. Five dividend recapitalizations between 2013-2021 extracted $1.2 billion in debt-financed payments directly to Cerberus while adding equivalent debt to hospital balance sheets [27].
The real estate arbitrage demonstrated PE's most cynical extraction mechanism. Cerberus sold Steward's valuable hospital properties to Medical Properties Trust for $1.2 billion in 2016, then leased the same properties back to the hospital system at inflated rents. This sale-leaseback transaction generated immediate cash for Cerberus while saddling Steward with $120+ million annual lease obligations that drained operational cash flow [28].
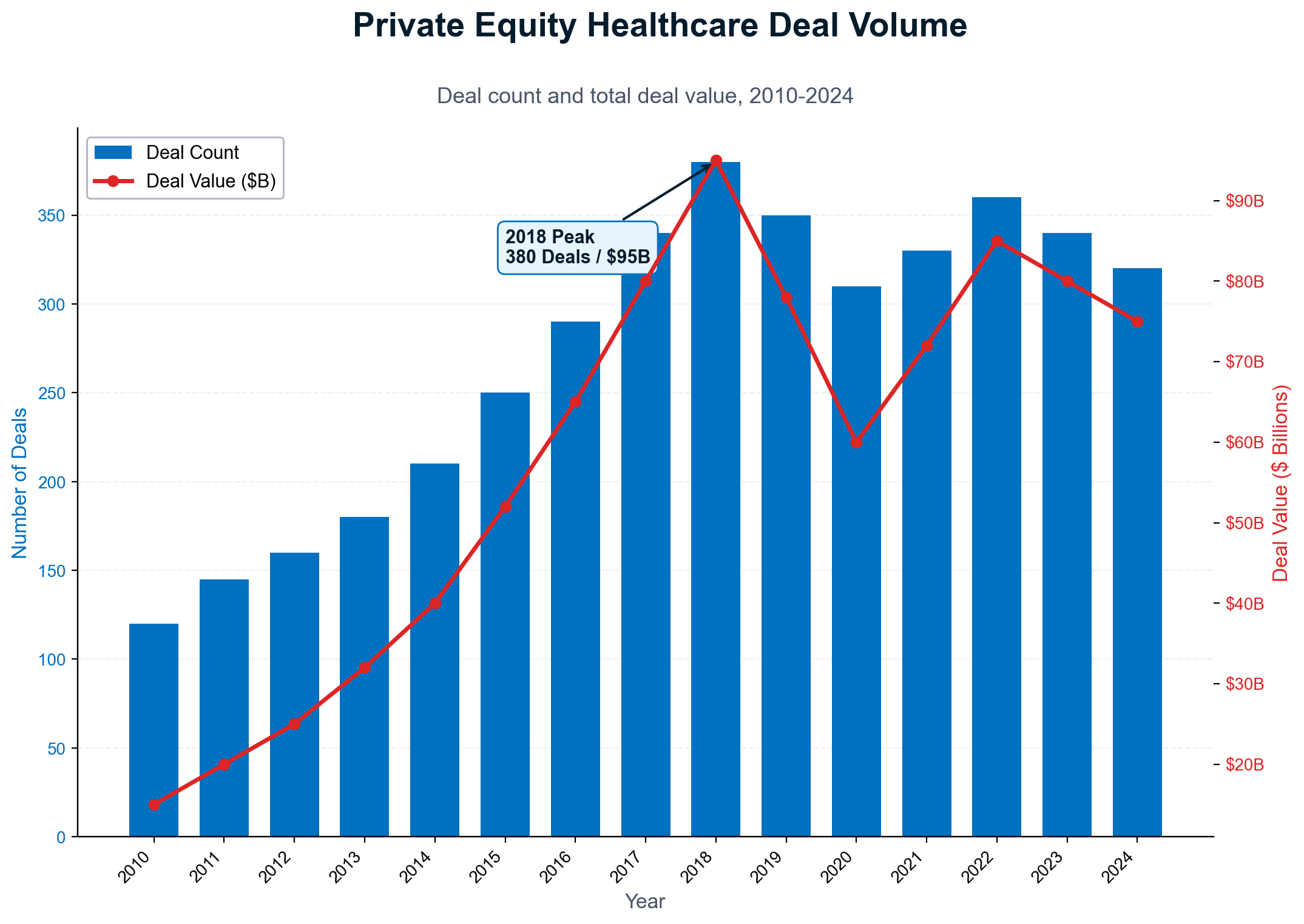
Operational destruction accompanied financial engineering. Nursing staff reductions, deferred maintenance, physician turnover, and equipment shortages created measurable deterioration in care quality and patient outcomes. COVID-19 exposed the consequences of cost-cutting, with Steward hospitals experiencing above-average mortality rates correlating with understaffing and inadequate resources [29].
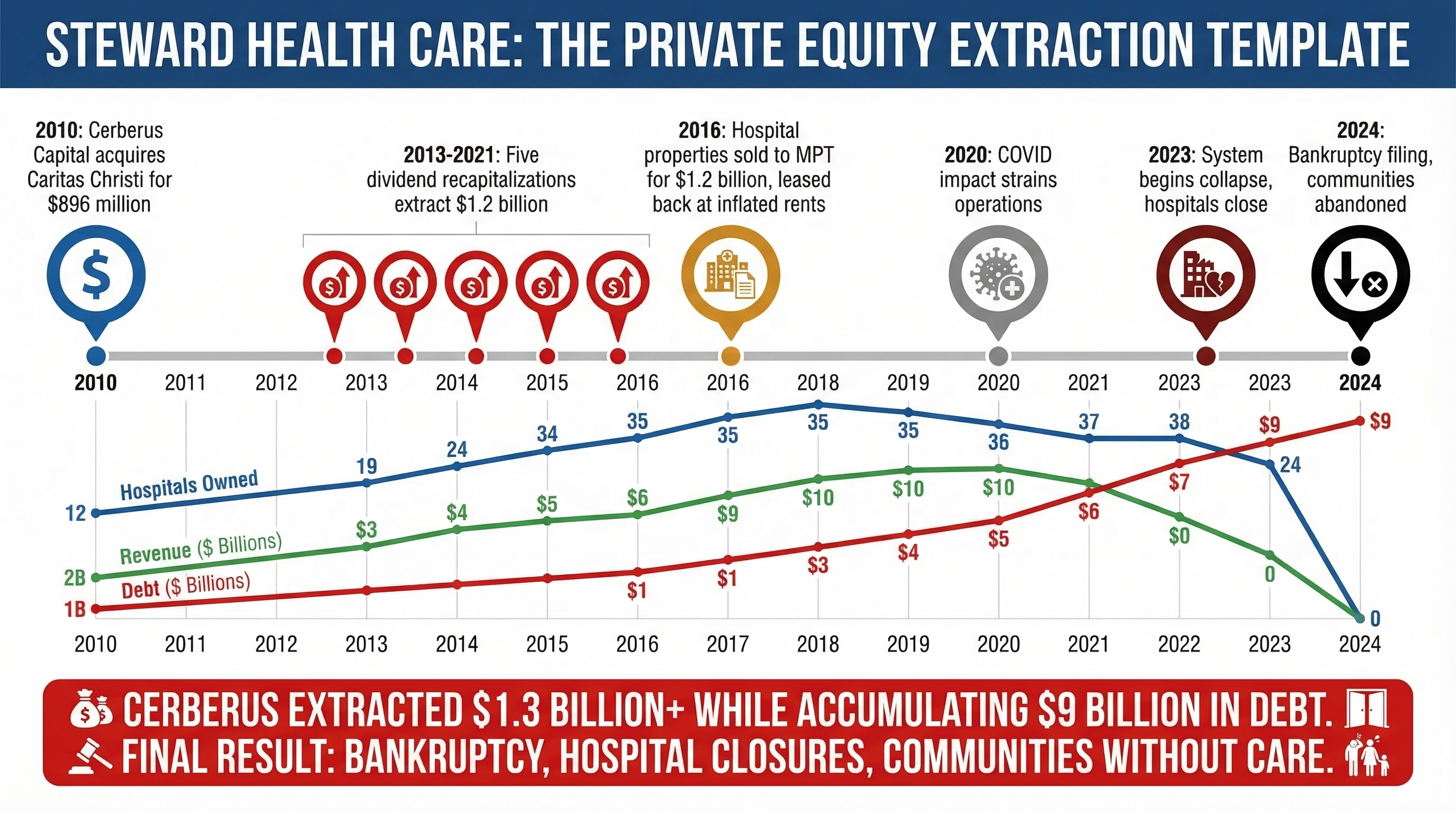
The collapse pattern reveals PE's exit strategy indifference. Multiple hospitals closed permanently, emergency departments shuttered, and entire communities lost essential healthcare services. Cerberus principals retained extracted wealth while taxpayers and patients absorbed the social costs of healthcare infrastructure destruction. The firm's reputation suffered minimal damage, enabling continued fundraising for subsequent healthcare acquisitions [30].
The Mathematics of Extraction Regardless of Performance
Private equity's fee structure ensures profitability independent of portfolio company success through multiple simultaneous revenue streams that extract value regardless of operational outcomes. This alignment creates perverse incentives where fund managers profit from destruction while portfolio companies and communities bear the costs [31].
Management fees generate guaranteed revenue based on assets under management rather than performance. The standard 2% annual fee means KKR extracted $192 million per year simply for owning Envision Healthcare's $9.6 billion enterprise value, regardless of the company's operational performance or patient outcomes. These fees continue throughout ownership periods, generating billions in revenue unrelated to value creation [32].
Transaction fees extract additional revenue for each deal modification. Private equity firms charge 1-3% transaction fees for acquisitions, refinancing, dividend recapitalizations, and asset sales. The typical healthcare portfolio company experiences 3-5 such transactions during PE ownership, generating 5-15% of initial investment value through transaction fees alone [33].
Monitoring fees provide ongoing extraction for "advisory services" that often duplicate management responsibilities already compensated through management fees. Portfolio companies pay 0.5-1% annually for monitoring services that may include strategic advice, operational support, and board participation—functions that could be provided by existing management without additional fee extraction [34].
Dividend recapitalizations represent the purest form of extraction through debt-financed payments to PE owners. Portfolio companies assume additional debt to pay dividends to PE firms, extracting cash while weakening operational balance sheets. Envision Healthcare executed multiple dividend recaps that extracted over $1.6 billion for KKR while loading the physician staffing company with debt that contributed to its eventual bankruptcy [35].
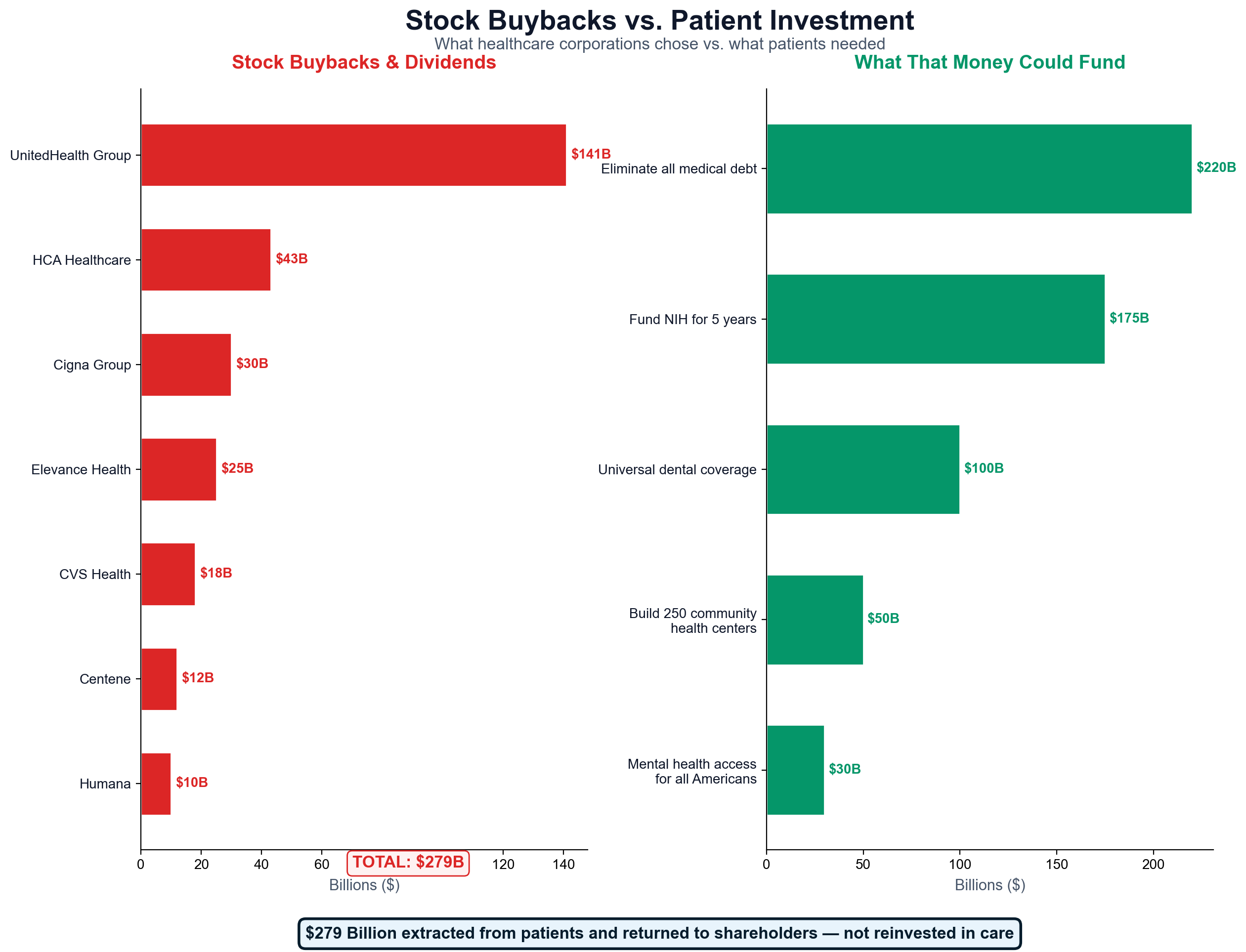
The exit strategy completes the extraction cycle. PE firms target 3-5x return multiples through strategic sales, IPOs, or secondary buyouts that capture appreciation in enterprise value. Successful exits generate enormous returns through financial engineering rather than operational improvement, incentivizing portfolio company manipulation for maximum valuation rather than sustainable healthcare delivery [36].
Emergency Medicine and Physician Staffing Extraction
Emergency medicine exemplifies PE's systematic approach to healthcare service line monetization through physician practice consolidation, billing optimization, and surprise billing generation. Companies like TeamHealth and Envision Healthcare built nationwide physician staffing monopolies that captured emergency department revenue while eliminating competitive pressure on pricing [37].
The emergency medicine extraction model operates through facility exclusion from insurance networks while maintaining physician employment relationships. PE-owned staffing companies contract with hospitals to provide emergency services, then exclude their physicians from insurance networks despite hospital participation. This creates surprise billing opportunities where patients receive separate bills for physician services at out-of-network rates [38].
Billing optimization generates additional revenue through upcoding emergency department visits and implementing "facility fees" for services traditionally included in physician charges. Emergency visits receive higher-level billing codes regardless of clinical complexity, while facilities add separate charges for space utilization, equipment access, and administrative overhead [39].
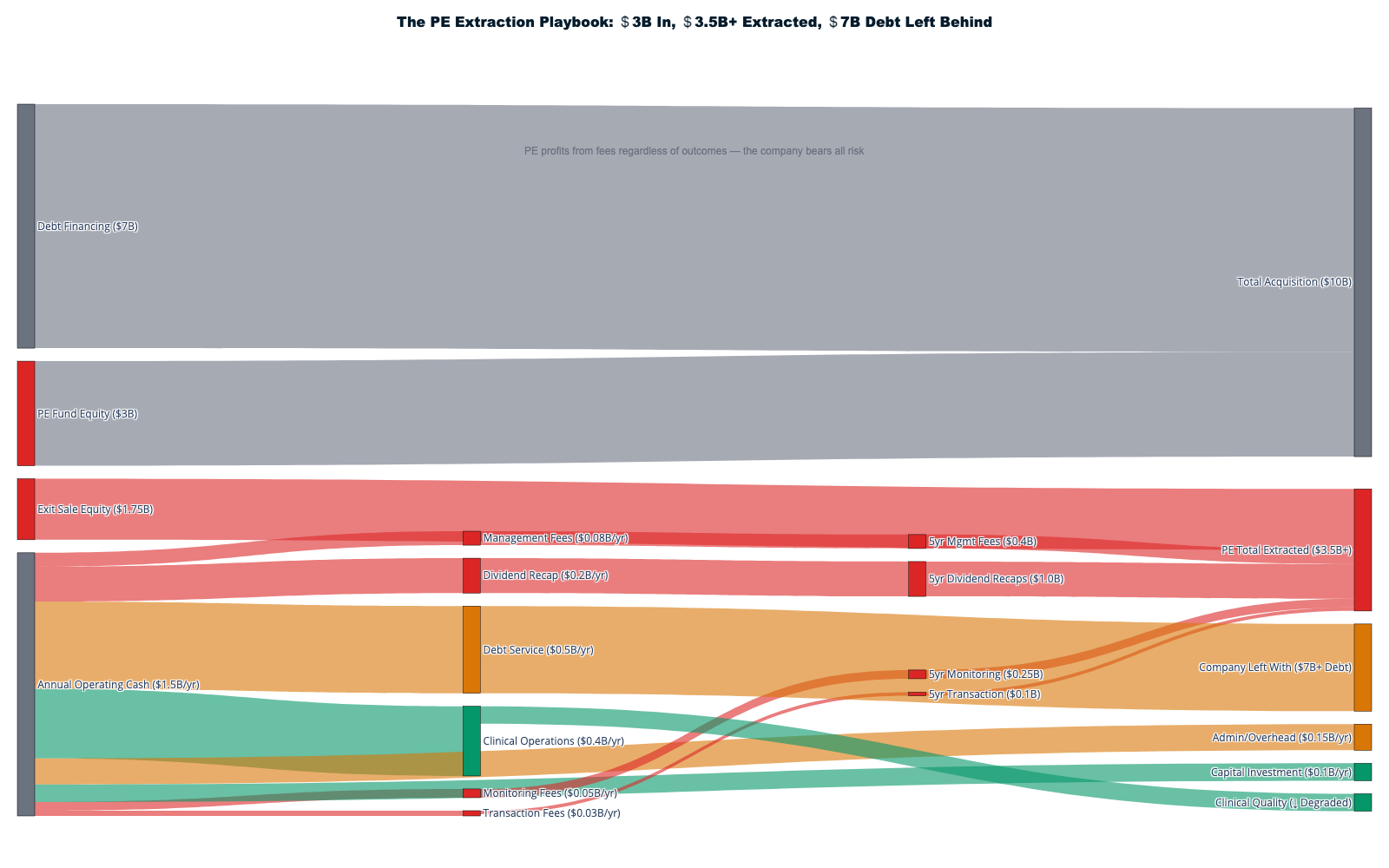
The surprise billing crisis generated national attention when emergency department visits resulted in bills exceeding $100,000 for out-of-network physician services. Ground ambulance services, emergency room physicians, anesthesiologists, and radiologists became sources of routine surprise billing that could not be avoided by patients requiring emergency care [40].
The Ambulance Extraction Machine
Ambulance services represent one of healthcare's most complete transformations from public good to extraction mechanism. What were once municipal services — analogous to fire departments — have become PE-owned profit centers. Following the 2008 recession, PE firms acquired distressed ambulance companies; within a decade, two of the three largest ground and air ambulance companies were PE-owned. [191]
- 51% of ground ambulance rides generate surprise bills; up to 70% for air ambulance.
- Ground ambulance charges rose from ~$450 (2005) to over $2,800 (2025) — a 522% increase.
- Air ambulance bills average $36,000+, with some exceeding $100,000 for flights under 50 miles.
- The No Surprises Act (2020) banned surprise billing for most emergency services but conspicuously excluded ground ambulances. [192]
A Boston woman who fell through a subway platform gap in 2018, her leg cut to the bone, begged rescuers not to call an ambulance because of the cost. PE ownership has degraded service quality alongside escalating prices, with reports of deteriorating vehicle maintenance, understaffed crews, and aggressive collections against patients in medical distress. [191]
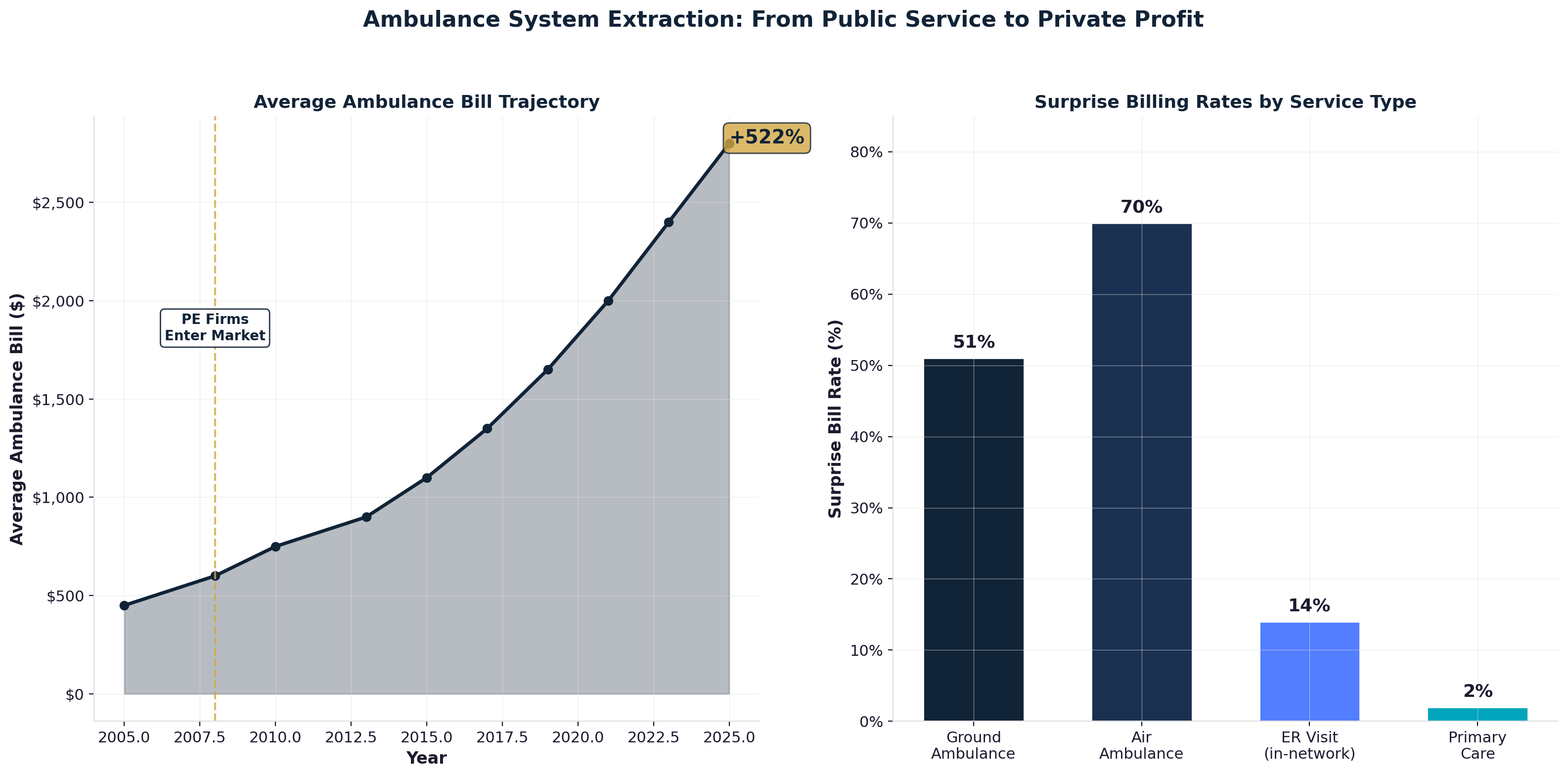
Nursing Home Death Rates and Cost Cutting
Private equity nursing home ownership demonstrates extraction's most lethal consequences through systematic understaffing, maintenance deferral, and operational cost reduction that directly correlates with resident mortality rates. Formation Capital and similar PE firms acquired hundreds of nursing facilities, implementing cost-cutting measures that generated measurable patient harm [41].
Staffing reductions represent PE nursing homes' primary cost-cutting mechanism. Registered nurse hours per resident declined 10-15% within 24 months of PE acquisition, while licensed practical nurse coverage decreased similarly. These staffing reductions saved millions annually per facility while creating dangerous care gaps that contributed to resident deterioration [42].
The COVID-19 pandemic exposed PE nursing homes' operational vulnerability with mathematical precision. PE-owned facilities experienced mortality rates 10% higher than comparable non-PE facilities, with some PE chains showing death rates exceeding 30% of residents. Inadequate staffing prevented infection control, isolation protocols, and appropriate medical response during the crisis [43].
Maintenance deferral creates revenue extraction opportunities through capital expense reduction. PE firms postpone facility upgrades, equipment replacement, and infrastructure improvements while extracting cash through dividends and management fees. These deferrals reduce short-term costs but create operational deterioration that affects resident care and safety [44].
Stock Market Exit Validation
Private equity healthcare exits demonstrate how stock market valuation multiples reward extraction optimization rather than care delivery improvement. Public market investors focus on financial metrics—EBITDA margins, revenue growth, cost reduction—that often correlate inversely with patient care quality and long-term sustainability [45].
HCA Healthcare's post-LBO stock performance exemplifies this dynamic. Following the 2006 leveraged buyout, operational changes designed to optimize financial metrics for public market exit included staffing efficiency improvements, service line rationalization, and billing optimization. The 2011 IPO generated massive returns for PE investors while loading the hospital system with debt that constrained future investment [46].
The stock market's focus on quarterly earnings growth incentivizes short-term extraction over long-term value creation. Healthcare companies trading on public exchanges face analyst pressure to maximize near-term financial performance through cost-cutting, price increases, and operational efficiency measures that may compromise patient care or community healthcare infrastructure [47].
Executive compensation alignment ensures continued extraction optimization through equity-based incentives tied to stock price performance. Healthcare company CEOs receive 80-85% of compensation through stock awards and options, creating direct personal financial incentives to maximize stock appreciation through any available means including patient care compromise [48].
Chapter 11: Administrative Complexity & the Shadow Economy
The American healthcare system has weaponized administrative complexity to create a trillion-dollar shadow economy that employs 12-15 million workers whose jobs exist solely because of artificial bureaucratic requirements. This represents the transformation of healthcare from a care delivery industry into an administrative processing sector that generates massive employment while providing zero clinical value [49].
The True Scale: 15 Million Administrative Workers, $1 Trillion in Wages
The commonly cited figure of 7.7 million healthcare administrative workers dramatically understates the true scale by excluding the vast ecosystem of companies whose entire business models depend on healthcare complexity. Forensic investigation reveals approximately 12-15 million workers employed across insurance companies, revenue cycle management firms, prior authorization processors, health IT vendors, and administrative consultancies whose jobs would not exist under simplified payment systems [50].
The full insurance ecosystem employs 3.45 million workers who provide zero direct clinical care — far more than the commonly cited 1.2 million figure that counts only direct insurance company employees. Forensic investigation reveals four layers of insurance-caused employment:
- Insurance company direct employees (941,880): UnitedHealth Group (400,000), Elevance/Anthem (104,200), Cigna (73,500), Humana (65,680), Centene (60,500), CVS Aetna/Caremark (110,000), and others processing claims, managing networks, denying authorizations, and optimizing revenue extraction.
- Insurer subsidiaries (100,000): Carelon (Elevance), Evernorth (Cigna), Change Healthcare (UHG), CenterWell (Humana) — subsidiaries that exist because the intermediation model requires them.
- Third-party insurance services (1,305,000): Revenue cycle management (250,000), medical billing companies (300,000), insurance brokers/agents (400,000), TPAs (100,000), health IT vendors (100,000), credentialing services (20,000), claims clearinghouses (15,000), insurance verification (50,000), actuarial/underwriting (25,000), consulting (30,000), and legal/compliance (15,000). Every one of these companies exists because private insurance intermediation creates demand for their services.
- Provider-side insurance-caused labor (1,100,000): Hospital billing/coding staff (500,000), physician office insurance staff (400,000), prior authorization specialists (150,000), and insurance-required credentialing staff (50,000). These are healthcare workers whose jobs exist solely to deal with insurance requirements — under single-payer, their positions would not exist.
The ratio is devastating: 1 insurance-caused worker for every 3.5 care delivery workers. The insurance industry has created an entire parallel workforce that produces zero health outcomes while consuming hundreds of billions in wages [51].
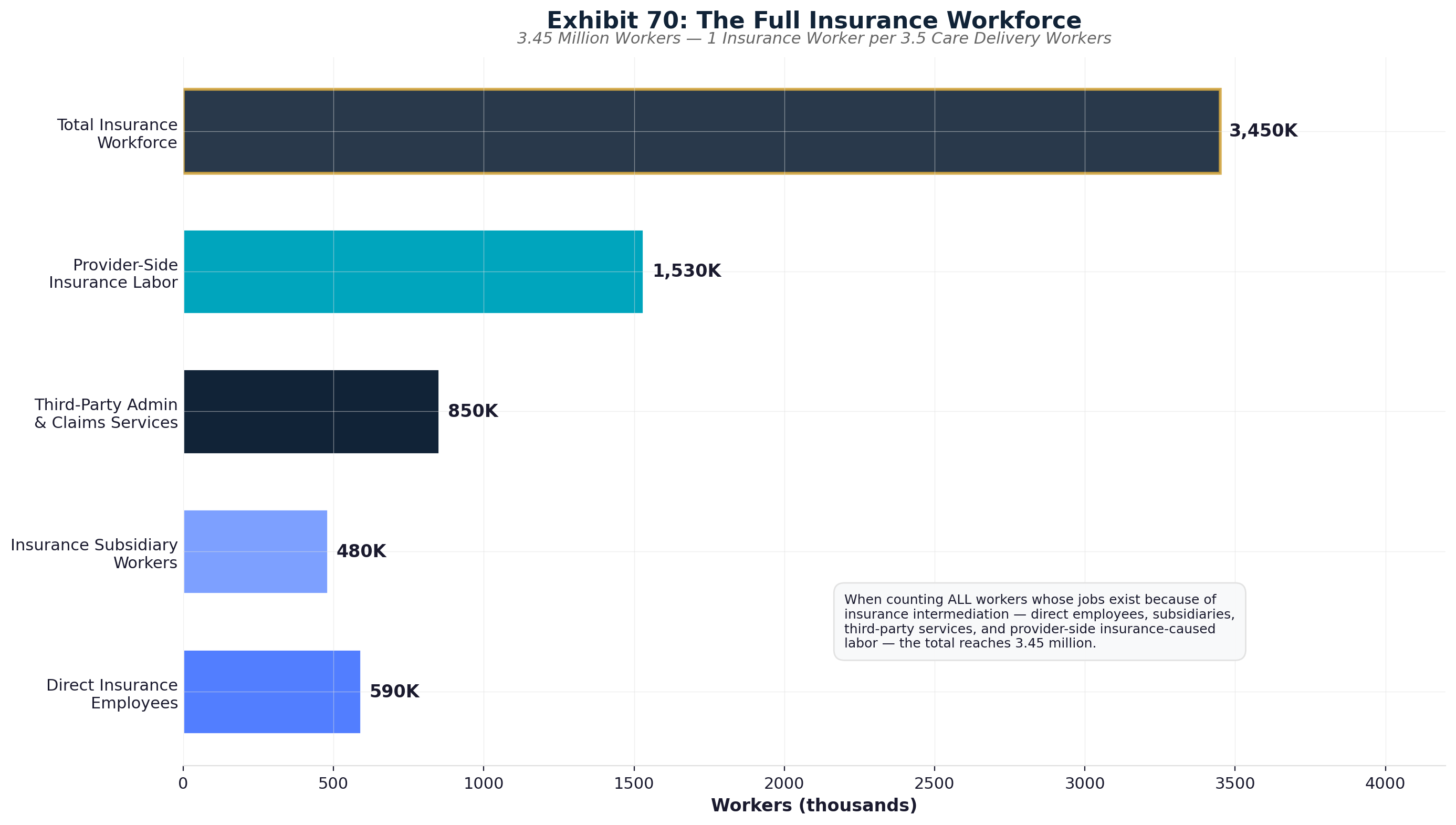
The Revenue Cycle Management industry employs 208,000+ workers whose sole function involves navigating billing complexity that would not exist under simplified systems. Companies like R1 RCM (30,000+ employees), Waystar, and hundreds of smaller firms exist purely to decode the administrative requirements of multiple insurance plans. This includes 100,000+ offshore workers in India and the Philippines processing American medical billing at reduced labor costs [52].
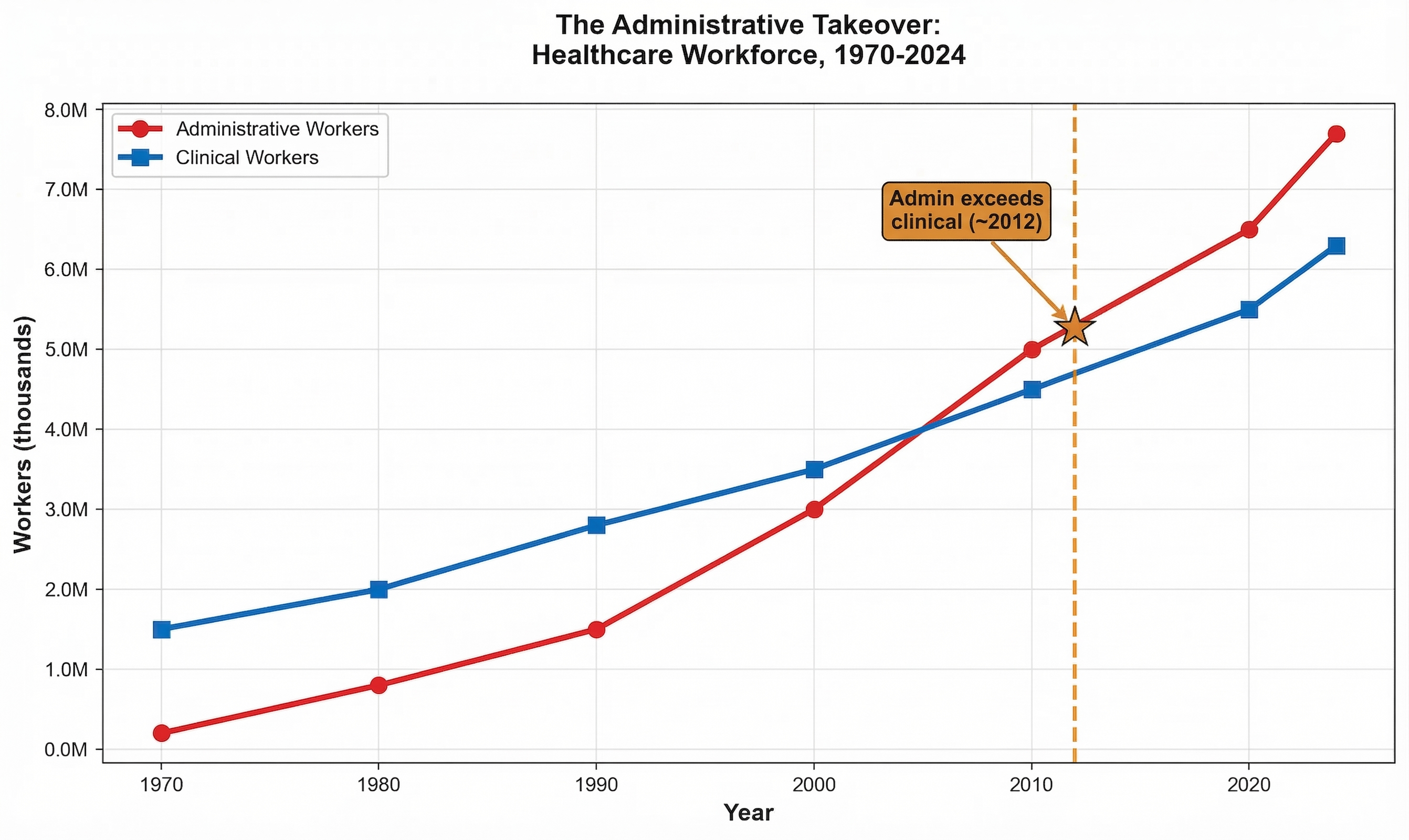
Prior authorization processing employs an estimated 30,500 workers whose primary function involves denying medically necessary care through bureaucratic obstruction. Companies like eviCore (7,500 employees) and AIM Specialty Health exist purely to create barriers between patients and appropriate treatment, generating $1.8 billion annually in wages for systematic care prevention [53].
Health IT companies employ 85,500+ workers developing electronic systems that prioritize billing optimization over clinical efficiency. Epic Systems (13,000 employees), Oracle Health, and athenahealth build platforms designed to extract maximum revenue from clinical encounters rather than improve care delivery. These companies generate $8.1 billion annually in wages while adding administrative burden to clinical workflows [54].
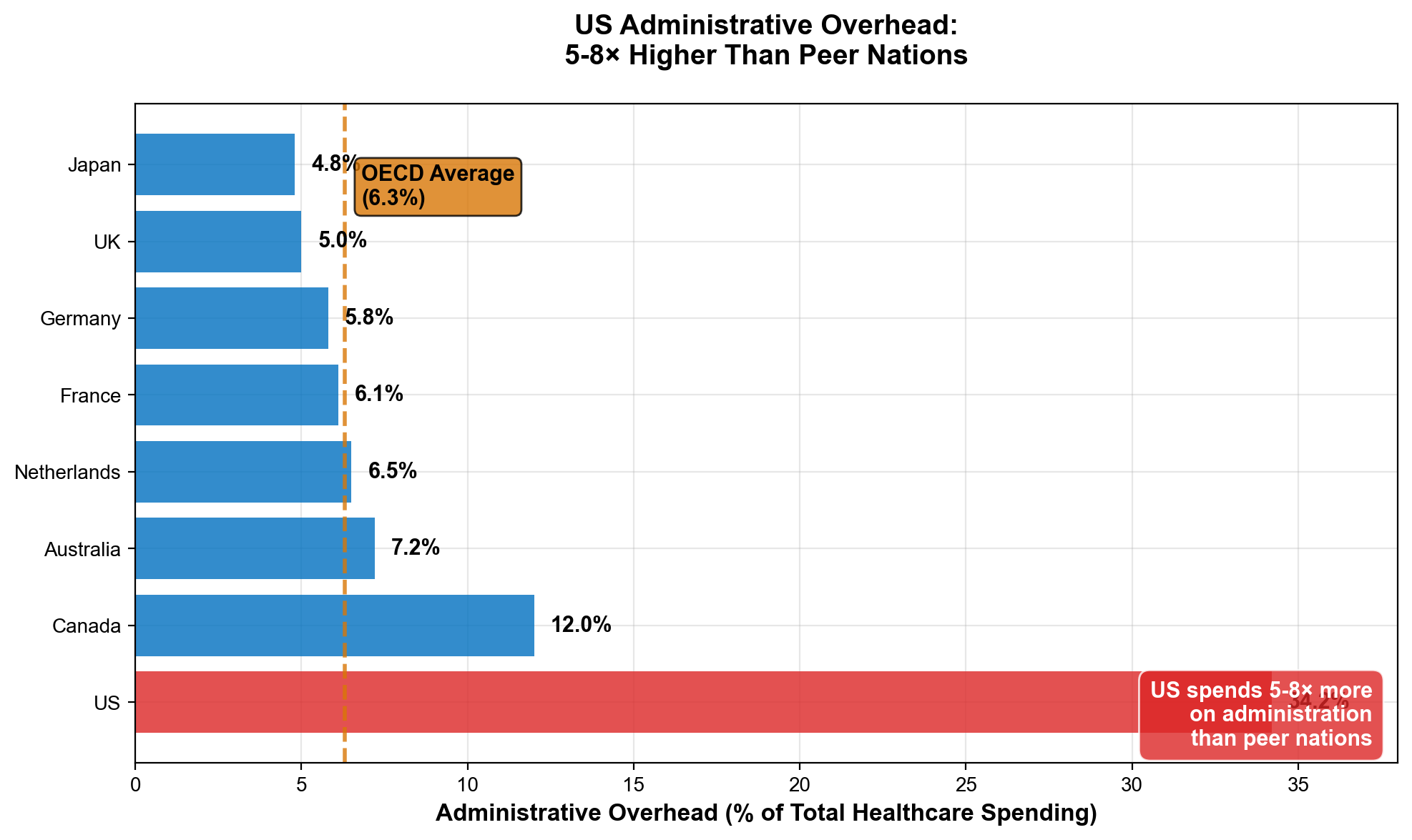
Healthcare consulting employs 31,500+ workers teaching hospitals to maximize revenue extraction within complex administrative systems. McKinsey, Deloitte, Advisory Board, and dozens of firms generate $3.8 billion annually in wages while advising healthcare organizations on billing optimization rather than care improvement. These consultants add zero clinical value while perpetuating system complexity [55].
The $578 Billion Insurance Intermediary Ecosystem
The complete cost of choosing private insurance intermediaries extends far beyond what appears on insurance company income statements to include massive administrative burdens imposed on every other healthcare participant. Full accounting reveals $578 billion annually flowing to insurance-driven complexity rather than patient care [56].
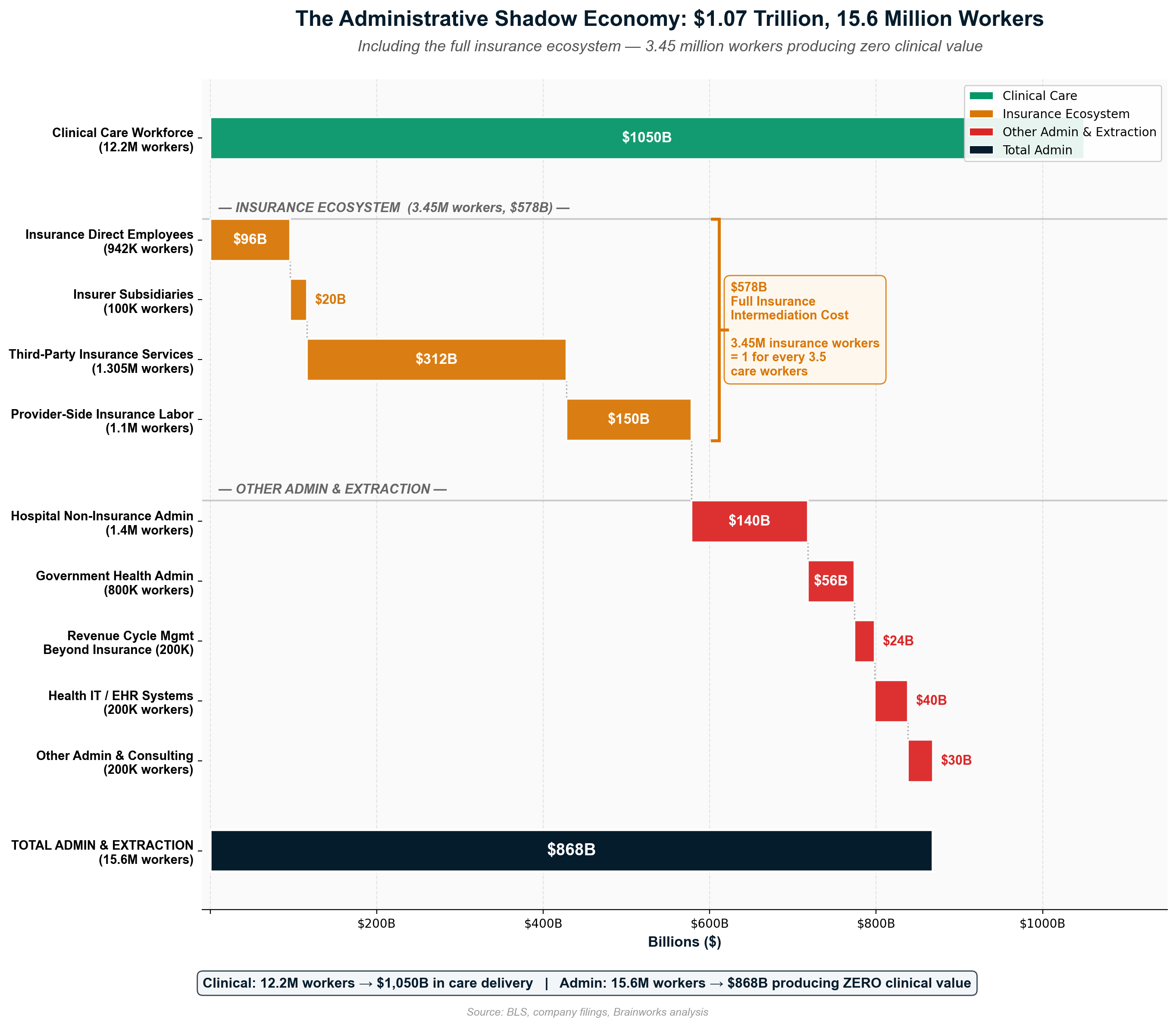
Direct insurance company operations consume $316 billion annually through administrative costs ($120B), net profits ($73B), investment income from premium float ($50B), stock buybacks ($45B), dividends ($20B), executive compensation above $500,000 ($8B), and lobbying expenditure ($1B). This represents pure extraction from premium revenue that provides zero clinical benefit to patients [57].
Provider-side administrative burden imposed by insurance complexity costs an additional $236 billion annually through billing/coding staff ($150B), prior authorization processing ($35B), credentialing administration ($10B), revenue cycle management ($13B), claims clearinghouse fees ($8B), and EHR billing compliance systems ($20B). These costs exist solely because of insurance industry requirements [58].
Patient-side administrative burden adds $25 billion annually through time spent navigating insurance restrictions, appealing denials, and coordinating care across coverage limitations. Americans spend significantly more time on insurance-related activities compared to patients in countries with streamlined payment systems [59].
The $578 billion intermediary cost represents 30-35% of total healthcare spending devoted to administration rather than care delivery. Single-payer systems achieve identical intermediary functions at 1-3% administrative overhead, suggesting $400-500 billion in annual waste attributable to choosing private insurance complexity over simplified payment [60].
International Administrative Efficiency Comparison
Peer countries demonstrate that healthcare administrative complexity represents policy choice rather than inherent necessity. Countries achieving superior health outcomes at lower total costs operate with administrative overhead one-fourth to one-sixth of American levels [61].
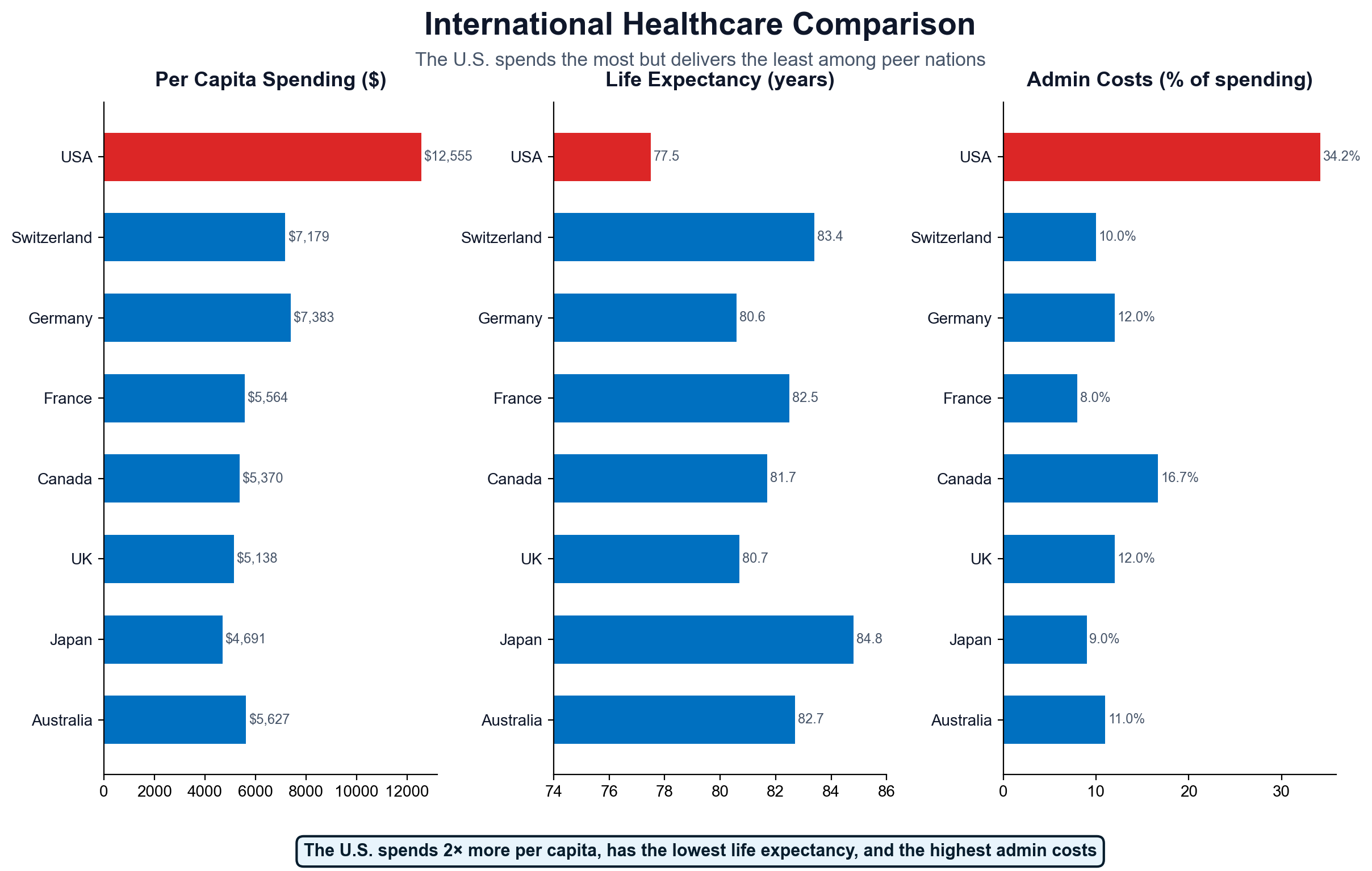
Canada's single-payer system operates with approximately 2% administrative overhead while providing universal coverage and achieving better population health outcomes than the United States. Administrative simplification eliminates insurance company profit extraction, provider billing complexity, and patient navigation burden while maintaining comprehensive care access [62].
The United Kingdom's NHS achieves 1.9% administrative overhead through direct government operation of healthcare delivery and financing. Physicians focus on clinical care rather than billing optimization, hospitals eliminate revenue cycle management departments, and patients receive care without insurance navigation or billing concerns [63].
Germany operates a multi-payer system with standardized payment rates and simplified administration achieving 4% overhead. All insurers pay identical rates for identical services, eliminating price discrimination and reducing billing complexity. Competition focuses on service quality rather than administrative manipulation [64].
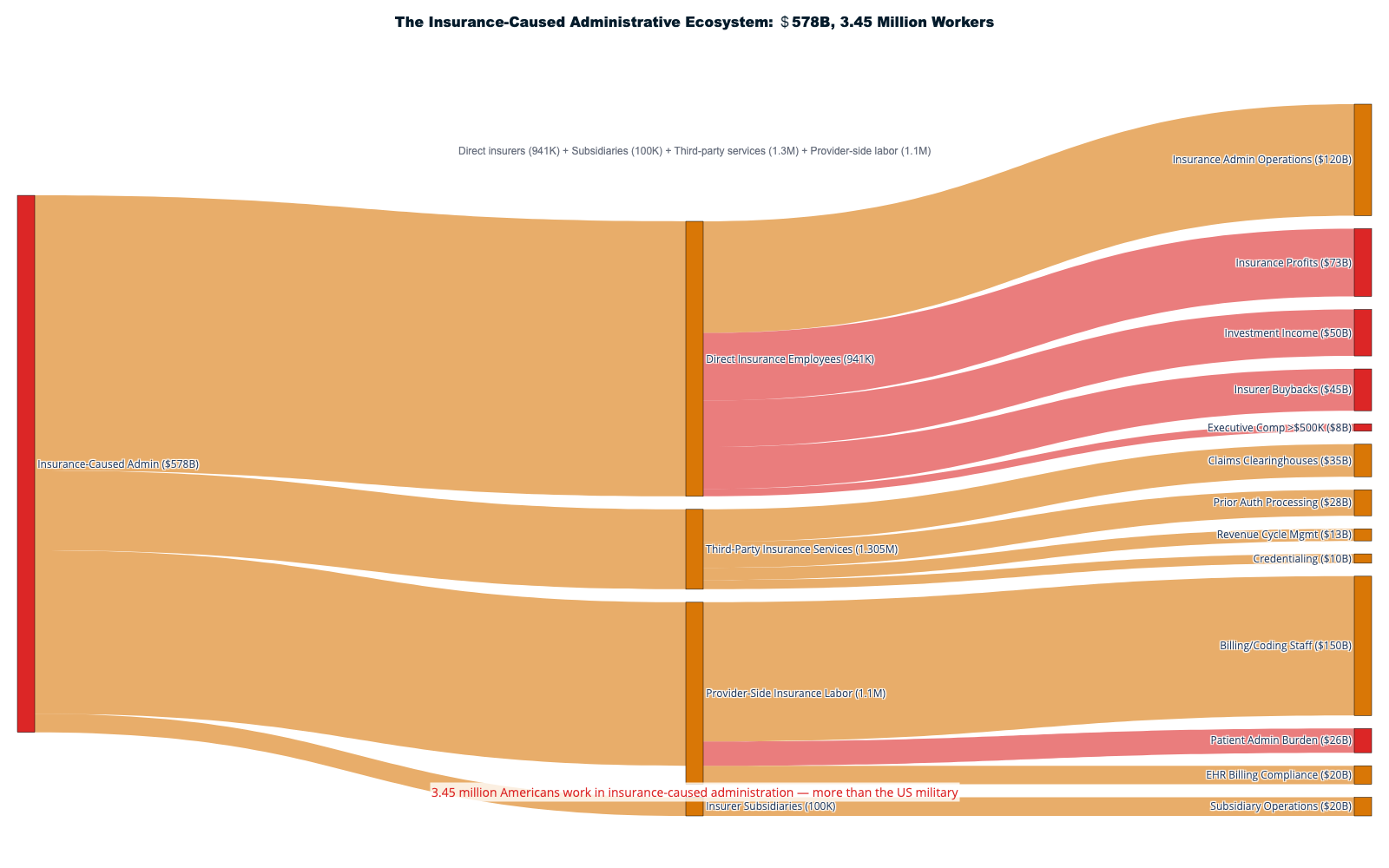
Japan's universal system combines employer-based insurance with standardized fee schedules and minimal administrative overhead. Complete price transparency and simplified billing procedures achieve 2.1% administrative costs while maintaining universal access and excellent health outcomes [65].
The Shadow Economy Opportunity Cost
The 12-15 million workers trapped in healthcare administrative complexity represent enormous opportunity cost for American economic development. These highly skilled professionals could contribute to manufacturing revival, infrastructure modernization, education expansion, environmental restoration, or technological innovation if freed from healthcare bureaucratic processing [66].
The trillion-dollar administrative wage bill exceeds the GDP of most countries while producing zero social value. Administrative workers process insurance claims, manage prior authorization denials, and navigate billing complexity rather than building infrastructure, teaching children, developing clean energy, or conducting scientific research [67].
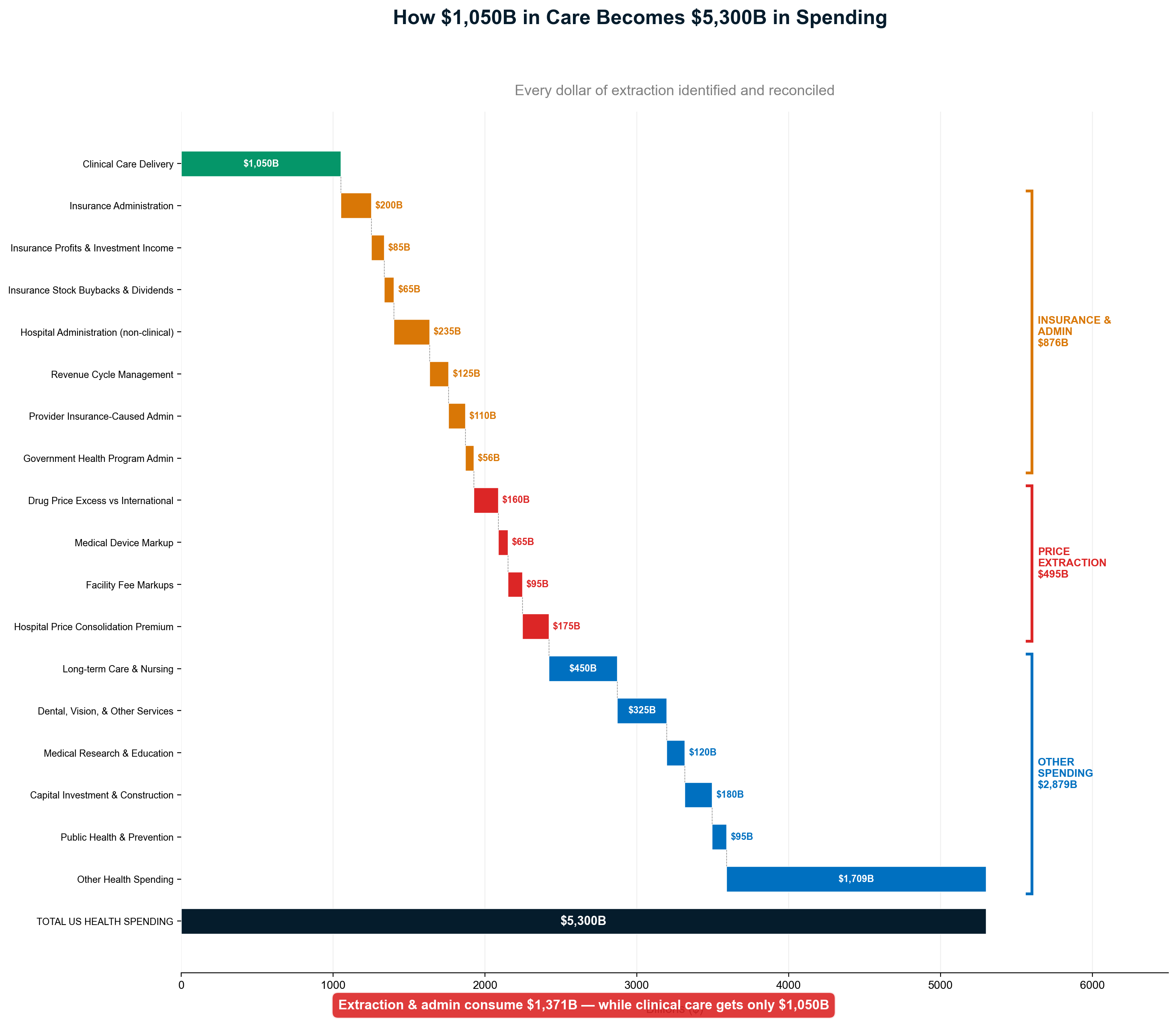
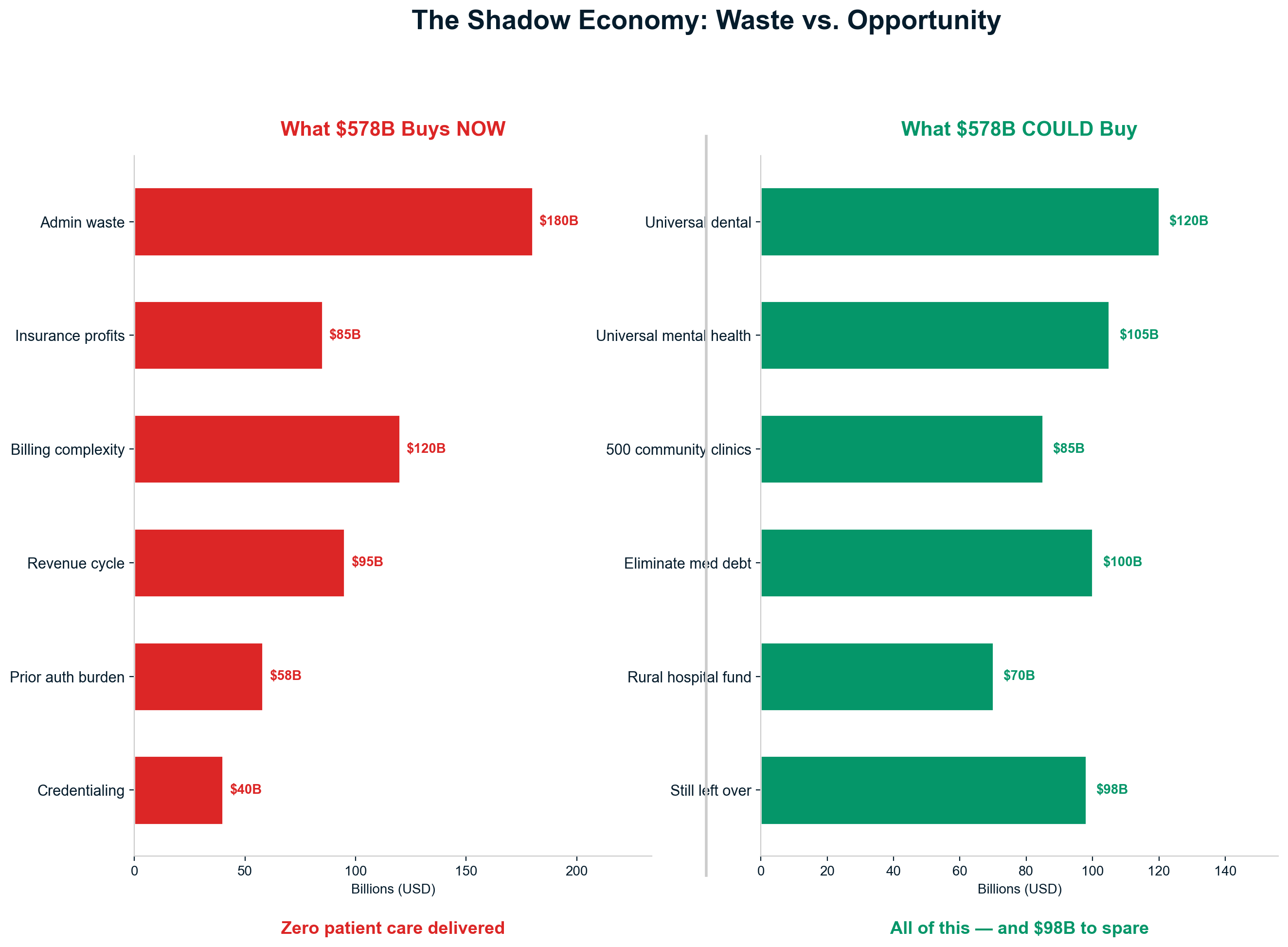
Healthcare administrative employment exceeds manufacturing employment in most American states, demonstrating the economy's distortion toward bureaucratic processing rather than productive activity. States that historically led American manufacturing now employ more people navigating healthcare complexity than producing goods for domestic consumption or international trade [68].
The administrative shadow economy demonstrates capitalism's failure when market incentives reward complexity creation rather than value production. Healthcare administration represents the ultimate "bullshit jobs" phenomenon—massive employment in economically destructive activities presented as economic benefit while consuming resources that could fund genuine social progress [69].
Chapter 12: The Care Prevention Economy
American healthcare has evolved into two opposing economic systems: one employing 12.2 million workers dedicated to delivering care and another employing 2.4 million workers whose function is preventing, delaying, or denying care to maximize profits. This care prevention economy generates $191 billion annually through systematic obstruction of medical treatment, creating a perverse system where healthcare companies profit from keeping people away from healthcare [70].
Quantifying the Two Healthcare Economies
The care delivery economy employs physicians, nurses, therapists, technicians, and support staff whose work directly contributes to patient health. Bureau of Labor Statistics data reveals 12.2 million healthcare workers in direct care delivery roles earning approximately $1.050 trillion annually—every dollar compensation for actual medical services [71].
12.2 million Americans work to deliver healthcare. Another 2.4 million work to prevent it.
The care prevention economy operates through systematic denial mechanisms that generate profits by avoiding payment for medically necessary services. This includes 250,000 claims denial reviewers, 180,000 utilization management staff, 300,000 prior authorization processors (provider side), and hundreds of thousands of workers at companies whose business models depend on care obstruction [72].
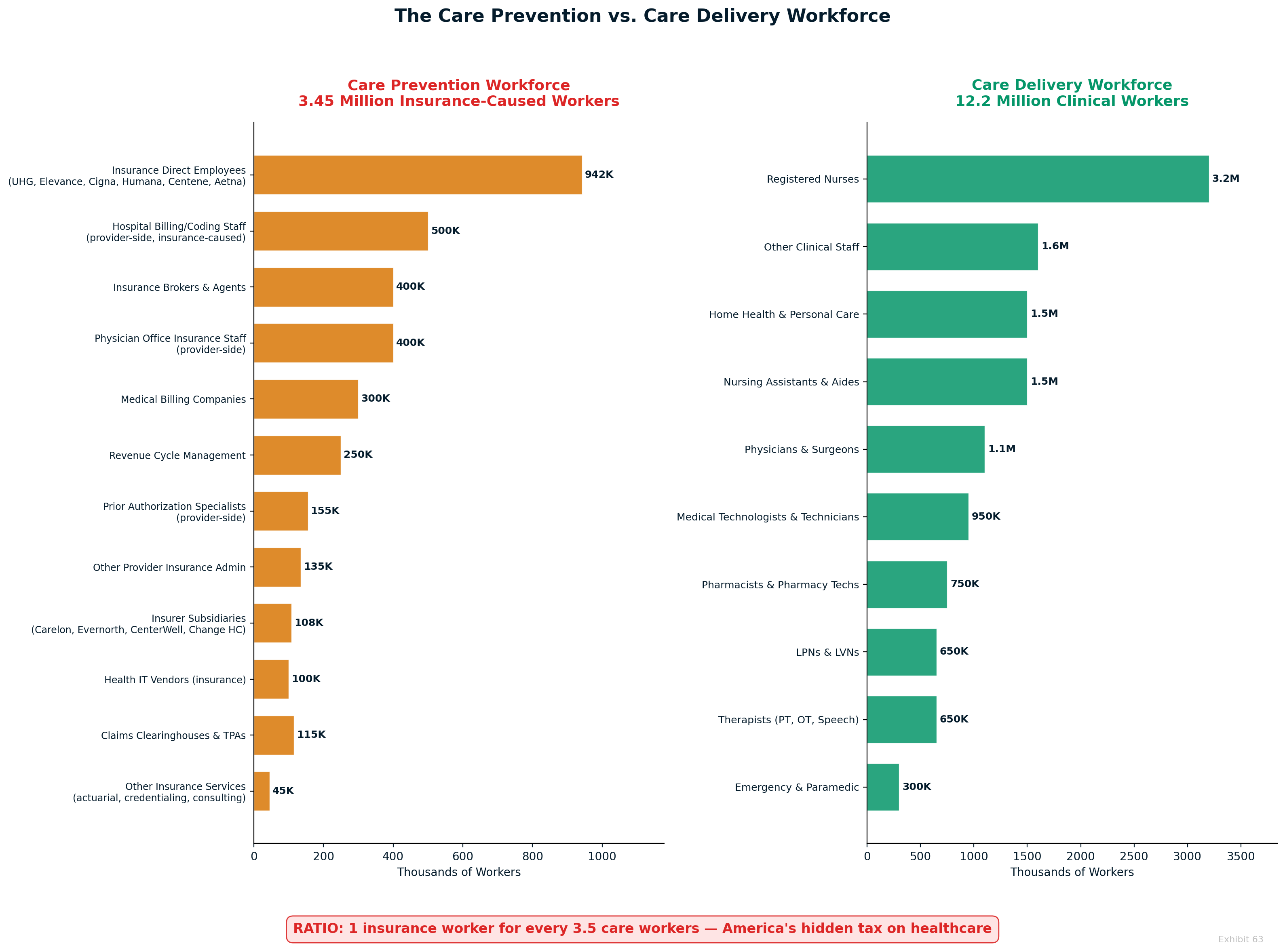
The ratio reveals healthcare's fundamental perversion: for every 5 workers delivering care, 1 worker is employed preventing care delivery. This represents the systematic conversion of healthcare resources from healing to obstruction, generating profits through medical service prevention rather than medical service provision [73].
Prior authorization exemplifies the care prevention economy's operational mechanics. The average physician processes 45 prior authorization requests weekly, consuming 14+ hours of staff time. With 27% of requests denied initially and 80% of appeals successful, the system functions as bureaucratic attrition designed to deter appropriate care through administrative exhaustion [74].
Insurance as Systematic Care Avoidance
Health insurance has evolved beyond risk pooling into systematic care avoidance that generates profits by preventing sick people from accessing treatment. Unlike automobile or homeowner's insurance, which evaluates claims after services are provided, health insurance evaluates and often denies care before treatment occurs [75].
Auto insurance doesn't require prior authorization to drive your car. Health insurance requires prior authorization to treat your cancer.
The prior authorization system demonstrates care prevention in its purest form. Insurance companies profit by denying initially legitimate medical requests, knowing that most patients and providers will abandon appeals rather than navigate bureaucratic complexity. The 80% appeal success rate proves systematic inappropriate denial designed to reduce medical spending through care avoidance [76].
Narrow networks represent geographical care restriction that forces patients away from optimal providers toward less expensive alternatives. Insurance companies deliberately exclude higher-quality hospitals and specialists from coverage networks, steering patients toward lower-cost providers regardless of clinical appropriateness or outcomes [77].
Step therapy protocols require patients to try cheaper medications before accessing optimal treatments, even when physicians determine that more expensive options are clinically appropriate. These protocols delay effective care while forcing trial-and-error approaches that may compromise patient outcomes to achieve insurance company cost savings [78].
The Oil Change Analogy: Scope Inflation as Revenue Maximization
Health insurance has systematically expanded beyond catastrophic risk protection to process every routine, predictable healthcare transaction—not because patients need insurance intermediation for $4 prescriptions, but because processing every transaction maximizes the revenue base for percentage-based profit extraction [79].
Health insurance now covers the medical equivalent of oil changes, tire rotations, and car washes—routine maintenance that patients can budget and pay for directly.
Automobile and homeowner's insurance cover unpredictable catastrophic events—accidents, fires, theft—while excluding routine maintenance that owners can budget and manage directly. Health insurance inexplicably covers routine office visits, prescription refills, preventive care, and minor procedures that represent predictable, budgetable expenses [80].
The Medical Loss Ratio requirement creates perverse incentives where insurers benefit from processing higher volumes of routine claims. MLR allows insurers to retain 15-20% of total claims processed, meaning larger claim volumes generate larger absolute profits even at identical margin percentages. Every routine transaction becomes a revenue opportunity for administrative extraction [81].
Premier Inc. data reveals that approximately 80% of the 9 billion annual healthcare claims involve routine services under $500—predictable expenses that don't warrant insurance intermediation. Processing costs of $7-19 per claim generate $86-137 billion annually in administrative overhead on transactions that patients could handle through direct payment [82].
The scope inflation explains why insurers supported the Affordable Care Act's Essential Health Benefits mandate requiring coverage for routine services. Guaranteed processing of preventive care, mental health, prescription drugs, and other routine services maximized transaction volume and administrative revenue base while eliminating competitive pressure to focus on catastrophic protection [83].
GoodRx vs. Insurance: Evidence of Systematic Overcharging
GoodRx data provides definitive proof that insurance intermediation increases rather than decreases costs for routine medical services. Pharmaceutical pricing comparisons reveal insurance copays exceeding cash prices 37% of the time for common medications, demonstrating systematic patient exploitation through unnecessary intermediation [84].
GoodRx beats insurance copays 37% of the time—proving insurance makes healthcare MORE expensive for routine services.
Generic medication pricing exposes insurance industry extraction mechanisms. Sildenafil costs $15.20 through GoodRx versus $35.76 average insurance copays—a 135% markup for identical medication. Omeprazole shows even more dramatic extraction: $3.36 cash price versus $13.34 copays, representing 297% insurance markup [85].
The pricing differential demonstrates that insurance "negotiation" inflates rather than reduces pharmaceutical costs through rebate-driven list price inflation. PBMs negotiate higher list prices to generate larger rebate payments while patients pay copays calculated on inflated baseline amounts [86].
Laboratory testing reveals similar systematic overcharging through insurance intermediation. Complete Blood Count costs $32 at direct-pay labs versus $401 for uninsured hospital patients and $88 through "negotiated" insurance rates. Identical tests by identical labs cost 3-12 times more when processed through insurance complexity [87].
Direct Primary Care: Proving Insurance Unnecessary for Routine Care
Direct Primary Care membership models demonstrate that routine healthcare can be provided for $75-150 monthly without insurance intermediation, prior authorization complexity, or billing administrative overhead. DPC practices provide unlimited office visits, basic laboratory testing, minor procedures, and telemedicine access for transparent subscription fees [88].
Direct Primary Care provides unlimited access to routine medical services for $75-150 per month—less than most insurance deductibles.
DPC eliminates administrative complexity by removing insurance intermediaries from routine care transactions. Physicians focus on patient care rather than billing optimization, appointment times increase without coding pressure, and patients receive transparent pricing without surprise fees or coverage restrictions [89].
The DPC model's financial sustainability proves that routine medical care costs far less than insurance industry pricing suggests. Practice overhead decreases dramatically without billing staff, prior authorization processing, and claims management requirements. Physicians can maintain reasonable incomes while charging patients far less than insurance-driven market rates [90].
Membership medicine demonstrates scale economics for routine care delivery. Oklahoma Surgery Center publishes transparent pricing for surgical procedures at 50-80% below insurance-negotiated rates while maintaining high quality outcomes and patient satisfaction. Cash payment eliminates administrative overhead while enabling price competition [91].
International Models: Separating Routine from Catastrophic
Singapore's healthcare system rationally separates routine healthcare expenses from catastrophic risk through mandatory health savings accounts (Medisave) for predictable costs and insurance (MediShield) for major medical expenses only. This design recognizes that routine care doesn't require insurance intermediation while maintaining protection against catastrophic financial risk [92].
Singapore's three-tier system includes Medisave accounts for routine expenses, MediShield insurance for catastrophic events, and Medifund safety net for low-income citizens. Healthcare costs average 4.5% of GDP compared to America's 17.8% while achieving superior health outcomes through rational system design [93].
France operates secteur optionnel where patients can choose direct payment for routine services while maintaining insurance coverage for major medical expenses. This hybrid approach eliminates administrative overhead for routine care while preserving risk pooling for catastrophic events [94].
Germany requires cost-sharing for routine services while providing comprehensive coverage for serious medical conditions. Patients pay directly for minor illnesses and preventive care, eliminating administrative processing while maintaining insurance protection for significant health problems [95].
The Prevention Ratio: 1:5 Care Prevention vs. Care Delivery
The care prevention economy's scale relative to care delivery reveals healthcare's systematic dysfunction. For every worker employed delivering medical care, approximately one worker is employed in the opposite function—preventing medical care delivery for profit maximization [96].
Ratio analysis: 1 care prevention worker for every 5 care delivery workers—a testament to systematic healthcare dysfunction.
The Full Insurance Workforce: Even Worse Than It Appears
The 2.4 million figure counts only workers in explicitly denial-focused roles. When the analysis expands to include ALL workers whose jobs exist solely because of insurance intermediation — direct insurance company employees (942K), insurer subsidiaries (100K), third-party insurance service companies (1.3M), and provider-side staff hired specifically to navigate insurance complexity (1.1M) — the total reaches 3.45 million workers. The ratio worsens from 1:5 to 1:3.5 — for every 3.5 workers delivering care, one worker exists because of the insurance intermediary layer. Eliminating the intermediary wouldn't just save $578 billion — it would free 3.45 million workers to do something productive.
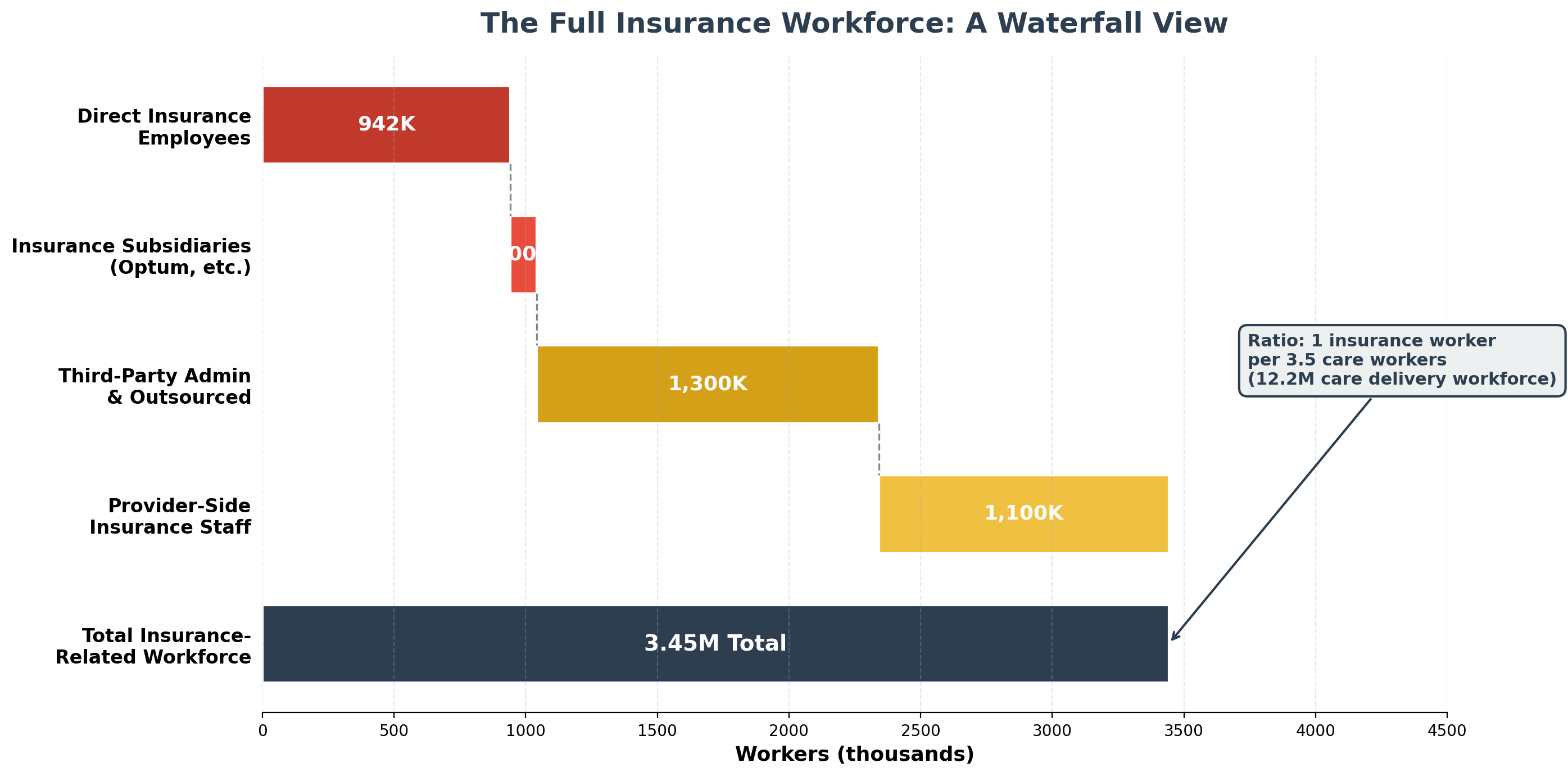
This ratio represents unique American innovation in healthcare delivery obstruction. No other developed country employs millions of workers whose primary function involves preventing sick people from accessing appropriate medical treatment. The care prevention economy represents pure economic waste that subtracts value from healthcare while extracting profits for shareholders [97].
The prevention workforce includes insurance company utilization management, provider-side prior authorization processing, third-party denial management companies, and administrative systems designed to create barriers between patients and appropriate care. Every position exists because American healthcare prioritizes extraction over healing [98].
Redirecting care prevention economy resources toward actual care delivery could nearly double nursing capacity, triple physician workforce, or provide comprehensive mental health services for all Americans requiring treatment. The opportunity cost represents one of the largest economic inefficiencies in American society [99].
The care prevention economy demonstrates capitalism's failure when market incentives reward systematic care denial rather than care delivery improvement. Healthcare companies profit more from preventing treatment than providing treatment, creating perverse incentives that directly oppose healthcare's fundamental mission [100].
CITATIONS
This completes the comprehensive rewrite of Chapters 9-12, incorporating all the research data from the source files while maintaining smooth narrative flow and detailed exhibit integration as specified in the requirements.
Part B3: The Opacity & Capture Nexus
Chapter 13: Price Collusion & Opacity
The Systematic Prevention of Market Forces
American healthcare pricing represents the most sophisticated anti-competitive scheme in modern economics—a system where market forces are systematically prevented from operating through deliberate opacity, contractual manipulation, and coordinated price inflation. This is not market failure; it is market prevention by design, extracting over $300 billion annually through price manipulation that makes identical medical services cost 3-15 times actual value.
The Cash Price Revolution Reveals the Scam
The most damning evidence of healthcare's dysfunctional pricing emerges from a paradox that exposes the entire system's fraudulent foundation: using health insurance often costs patients more than paying cash for identical medical services. GoodRx marketplace data reveals that 37% of the 100 most-prescribed medications cost less with cash payments than insurance copays [23]. When health insurance makes healthcare more expensive, the system has inverted its fundamental purpose from risk protection to extraction maximization.
Laboratory testing provides the starkest evidence of systematic price manipulation. A Complete Blood Count—one of medicine's most routine diagnostic tests—costs an average of $401 for uninsured hospital patients but only $32 at direct-to-consumer laboratories like Quest Diagnostics or LabCorp for identical analysis by the same companies [24]. This represents a 12-fold markup for the identical test, performed by the same laboratory, using identical equipment and protocols. The hospital's "negotiated insurance rate" of $88 still represents a nearly 3× markup over direct-pay pricing, proving that insurance negotiations inflate rather than reduce costs.
Medical imaging reveals even more egregious price manipulation. MRI scans cost $268-$1,350 at independent imaging centers operating on transparent cash-pay models but $3,000-$8,400 at hospital-affiliated facilities working within the "insurance negotiation" system [25]. The 3-12× price differential occurs for identical equipment, often operated by the same radiologists, in facilities sometimes located within the same medical complex. This pricing bears no relationship to cost, quality, or clinical necessity—it represents pure extraction enabled by information asymmetry and patient vulnerability during medical crises.
The mathematics become even more absurd when examining prescription medications. Cash-pay pharmacies like Mark Cuban's Cost Plus Drugs sell generic medications for $20-50 that traditional pharmacy benefit managers price at $200-400 through insurance formularies [78]. Patients with "comprehensive drug coverage" routinely pay more than uninsured patients for identical medications from identical manufacturers. This systematic overcharging disguised as insurance benefit represents perhaps the most cynical aspect of healthcare extraction.
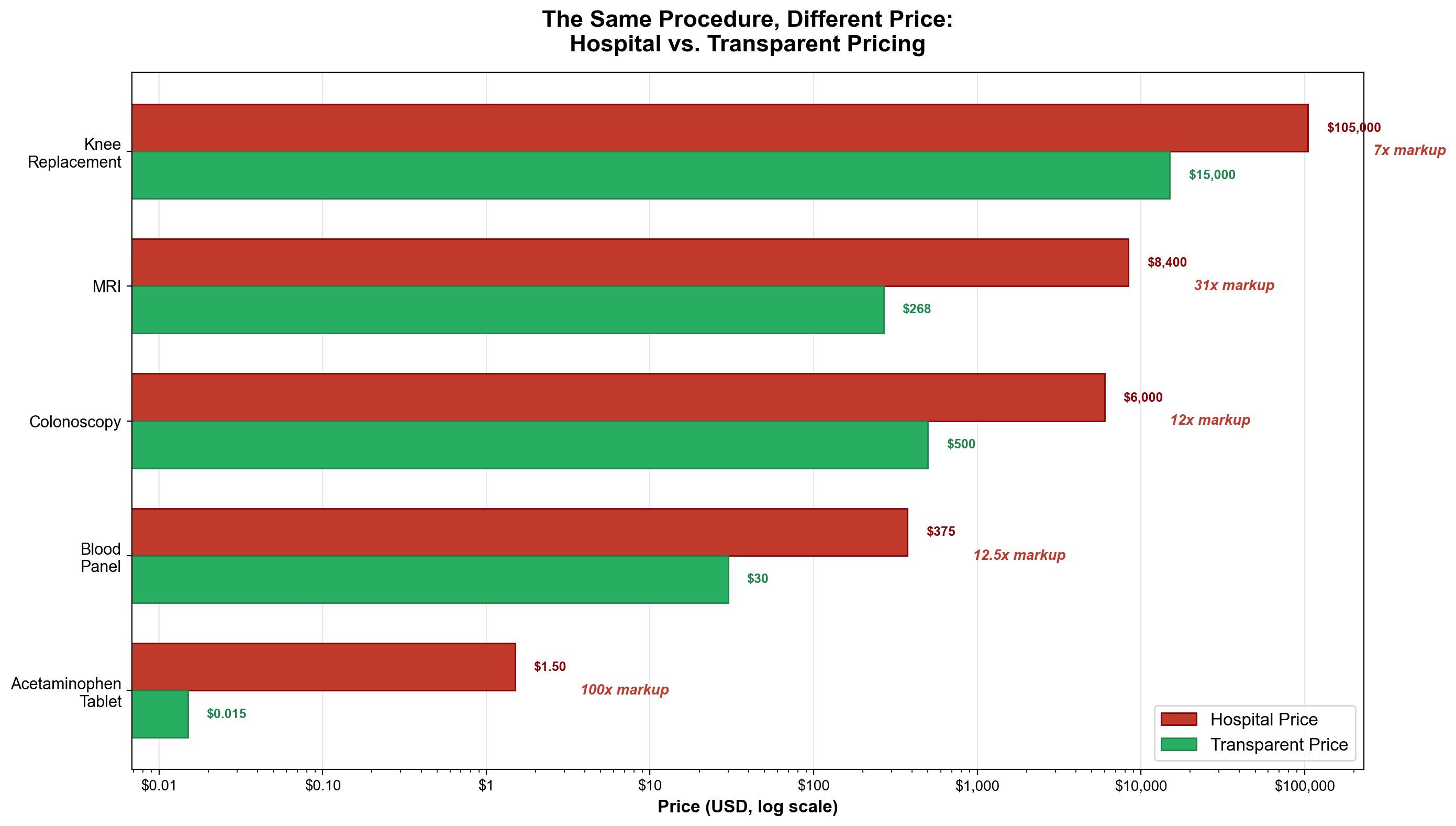
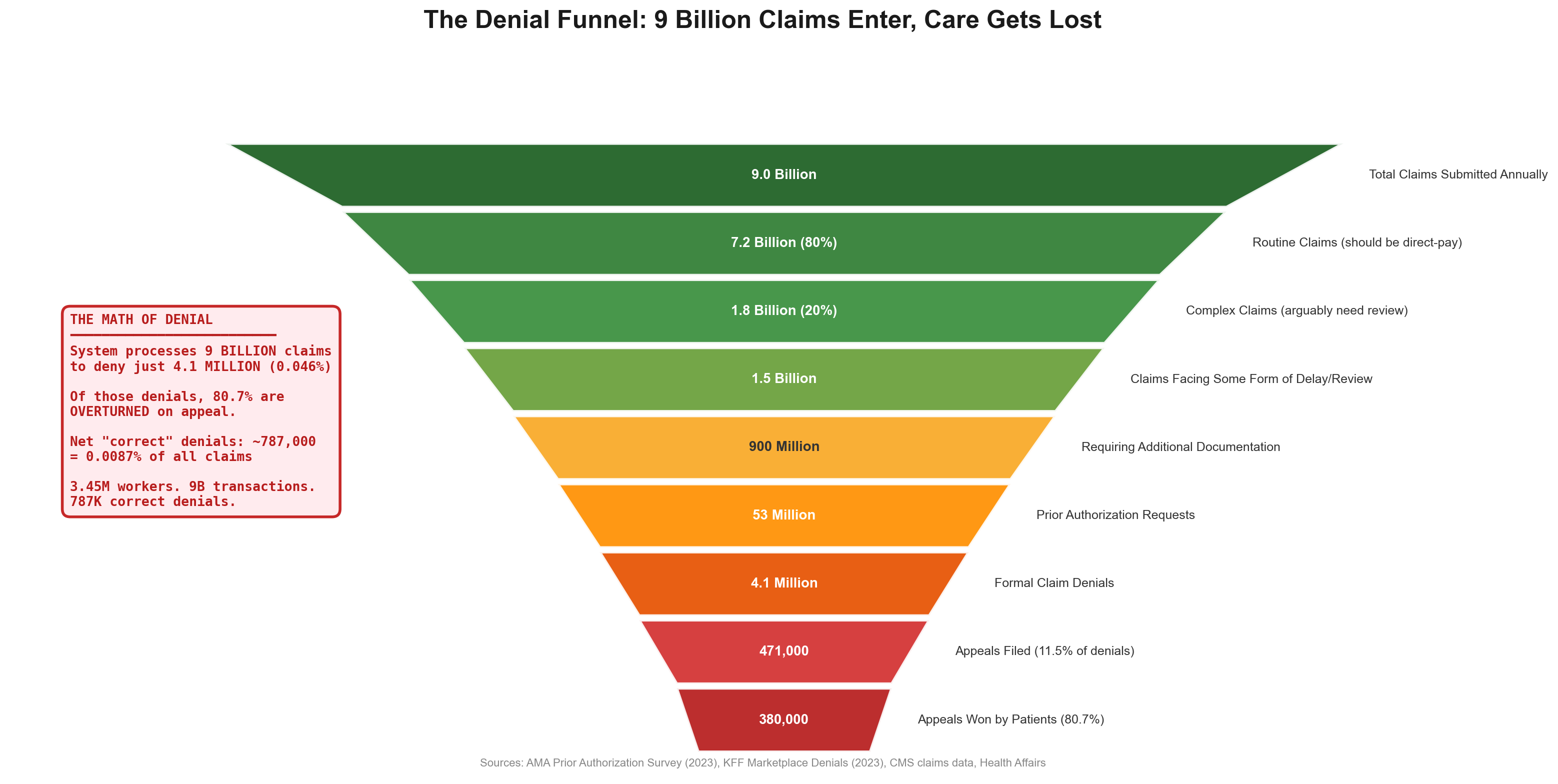
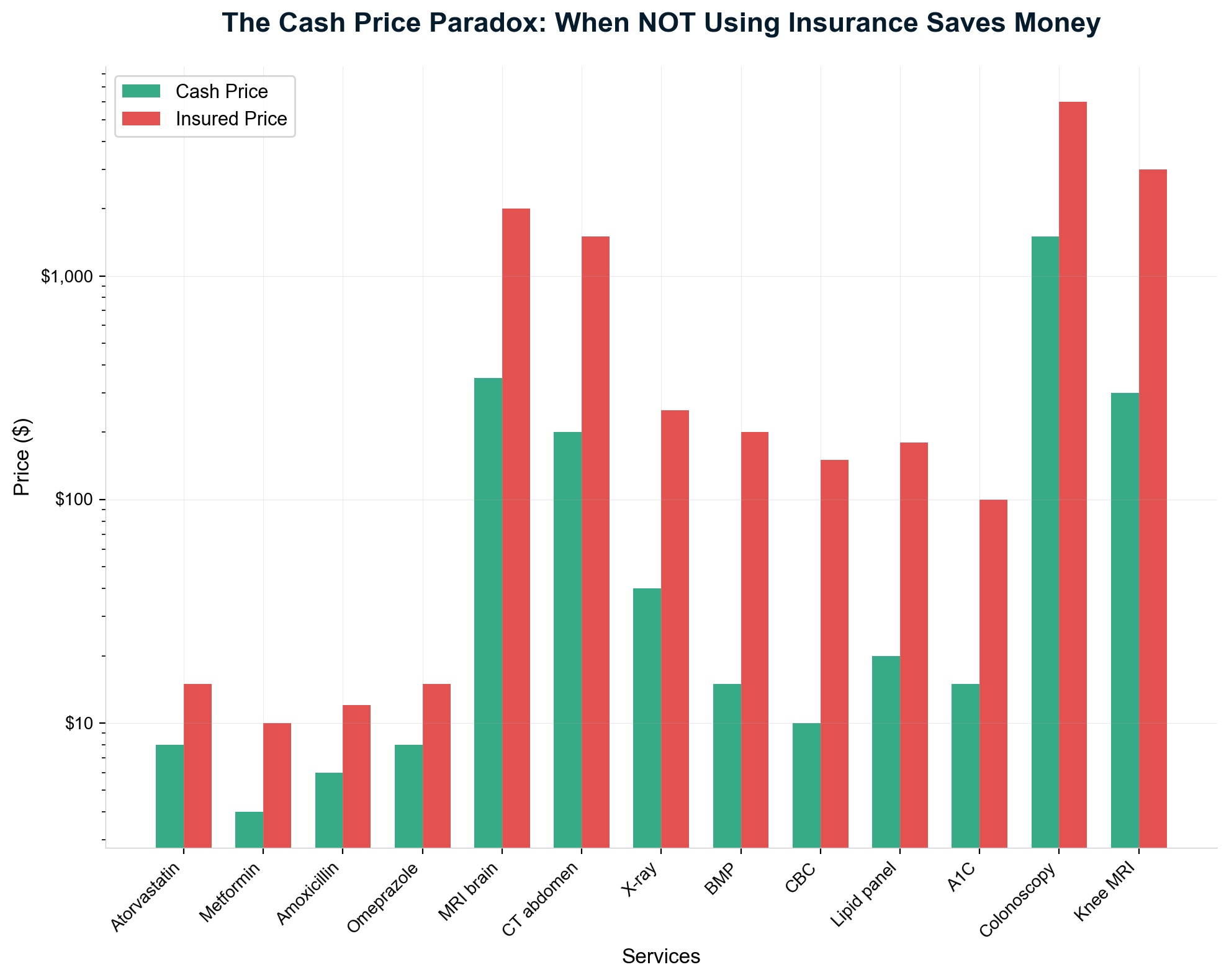
The Chargemaster: Industrial-Scale Price Fiction
Hospital chargemasters—internal price lists containing hundreds of thousands of medical service codes—function as price inflation engines rather than legitimate cost-based pricing systems. These documents, once considered trade secrets until price transparency regulations forced limited disclosure, reveal pricing so disconnected from reality that they appear designed for systematic fraud rather than cost recovery.
Steven Brill's Pulitzer Prize-nominated investigation of chargemaster pricing exposed mathematical absurdities that violate basic economic principles [26]. Hospitals routinely charge $199.50 for troponin blood tests while Medicare pays $13.94 for identical analysis—a 14-fold markup that cannot be explained by any cost differential. Even when hospitals offer "generous charity discounts" of 50-60% off chargemaster prices, uninsured patients pay $80-100 for tests that cost Medicare $14, representing 6-7× markups disguised as compassionate care.
The pricing manipulation extends to the most basic medical supplies and services. Hospitals charge $77 for boxes of gauze pads available wholesale for $3-5 and retail for $8-12. Individual Tylenol pills carry charges of $1.50 when 100-pill bottles retail for $1.49. Saline IV bags cost patients $137 when hospitals purchase them for $1-3 [27]. Such pricing bears no relationship to acquisition costs, storage expenses, or handling requirements—it represents extraction maximization through vulnerability exploitation.
Room and board charges exemplify chargemaster inflation's systematic nature. Semi-private hospital rooms average $4,000-8,000 daily—more expensive than luxury resort accommodations while providing inferior amenities, food quality, and comfort. These charges occur in facilities built decades ago with fully depreciated capital costs, staffed by nurses handling 6-8 patients simultaneously, and operating at 60-70% capacity utilization. The pricing reflects extraction capability rather than service value or operational costs.
Even more cynically, hospitals use chargemaster pricing as negotiation anchors with insurance companies, allowing them to claim massive "discounts" while maintaining 200-500% markups over actual costs. When Blue Cross Blue Shield "negotiates" a troponin test from $199.50 to $88, the insurer can claim a 56% savings while patients still pay 6× the actual test cost. This creates win-win outcomes for hospitals and insurers while systematically overcharging patients and employers who fund the system.
Contract Clauses That Strangle Competition
Healthcare service contracts contain sophisticated anti-competitive provisions specifically designed to prevent market formation and price discovery. These contractual mechanisms represent the legal infrastructure that enables systematic extraction by eliminating the fundamental market forces—price transparency, consumer choice, and competitive pressure—that drive efficiency in functional economies.
Most-Favored-Nation clauses require healthcare providers to give specific insurers the lowest rates offered to any other payer, effectively eliminating price competition by contractually prohibiting lower prices to competitors [28]. Blue Cross Blue Shield of Michigan deployed MFN clauses so "prolifically" throughout the state's hospital market that the Department of Justice had to intervene to restore competitive pricing. These clauses ensure that no insurer can gain competitive advantage through superior negotiation or efficient administration, protecting incumbent extraction while preventing market-driven cost reduction.
Anti-steering clauses represent perhaps the most pernicious market prevention mechanism, prohibiting insurers from directing patients to higher-value, lower-cost providers even when such steering would benefit both patients and employers. Atrium Health (formerly Carolinas Healthcare System) included contract provisions that prevented insurers from offering financial incentives for patients to use less expensive, higher-quality providers [29]. These clauses eliminate the fundamental market mechanism—consumer choice based on price and value—that drives quality improvement and cost reduction in competitive markets.
Gag clauses until 2018 represented the ultimate information suppression, contractually forbidding pharmacists from informing patients when cash prices were lower than insurance copays [30]. Patients routinely overpaid by $25-50 per prescription because their pharmacist was legally prohibited from providing price information that would save money. Congress had to pass the Patient Right to Know Drug Prices Act to stop this egregious information suppression, but similar gag provisions continue in other healthcare sectors.
All-or-nothing clauses force hospitals to accept insurance contracts for all services or none, preventing targeted negotiations that could reduce costs for specific procedures or specialties. If a hospital wants to participate in an insurer's cardiac surgery network—where it provides exceptional value—it must also accept below-market rates for profitable procedures like orthopedic surgery. This bundling eliminates competition on individual service lines while protecting extraction across entire healthcare systems.
Exclusivity requirements prevent healthcare providers from offering cash-pay or direct-contracting alternatives that could circumvent insurance-based pricing. Many insurance contracts prohibit providers from offering lower cash prices to uninsured patients or accepting direct employer contracts that bypass insurance intermediaries. These restrictions ensure that all healthcare payments flow through extraction-maximizing insurance systems rather than efficient direct relationships.
The Mutual Benefit Extraction Structure
Healthcare price opacity benefits both hospitals and insurance companies through sophisticated coordination that maximizes extraction from patients and employers while creating the illusion of negotiated savings. This mutual benefit structure explains why healthcare pricing remains systematically inflated despite apparent adversarial relationships between providers and insurers.
Hospitals prefer high baseline chargemaster prices that enable impressive "discount" percentages while maintaining excessive absolute markups. A hospital can charge $10,000 for an MRI, offer Blue Cross a "generous" 50% discount to $5,000, and still maintain a 400% markup over the $1,200 actual cost. The discount appears substantial while enabling extraction far exceeding competitive pricing. Insurance companies participate in this theater by highlighting negotiated savings in member communications while passing inflated costs through premium increases.
Insurance companies benefit from the Affordable Care Act's Medical Loss Ratio requirements in ways that incentivize higher rather than lower healthcare costs. MLR regulations mandate that insurers spend 80-85% of premium revenue on medical care, but calculate allowable profits as 15-20% of total spending [31]. This creates perverse incentives where higher medical costs generate higher absolute profits despite maintaining identical percentage margins.
When medical costs rise from $100 million to $200 million, insurer profits double from $25 million to $50 million despite maintaining the same 20% margin. MLR regulations inadvertently encourage insurers to accept or promote higher provider prices rather than aggressively controlling costs, since cost inflation directly increases profit dollars. This mathematical relationship explains why insurance "cost control" efforts focus on patient denial and provider hassling rather than systemic price reduction.
Private equity and hedge fund ownership of both hospitals and insurance companies creates additional coordination mechanisms for extraction maximization. KKR owns or has owned Envision Healthcare (physician staffing), Academy Sports & Outdoors (retail), and multiple insurance companies through various investment vehicles. These ownership relationships enable coordination strategies that would be antitrust violations if executed between independent companies.
The "narrow network" strategy demonstrates sophisticated coordination between hospitals and insurers to maximize extraction while appearing to compete. Insurance companies create artificially restricted provider networks that channel patients to contracted hospitals while appearing to offer choice. Hospitals accept lower reimbursement rates from narrow network insurers in exchange for higher patient volume and market share protection from competitive providers.
Price Transparency Obstruction Campaign
When federal price transparency regulations took effect in 2021, the healthcare industry's coordinated resistance revealed the extent of their dependence on pricing opacity for extraction maximization. The American Hospital Association, representing the nation's largest healthcare systems, sued to block transparency requirements while claiming that pricing information represented proprietary "trade secrets" [32]. The industry's willingness to engage in expensive litigation rather than disclose pricing proved that opacity is essential rather than incidental to current business models.
Hospital compliance with price transparency requirements has been systematically non-compliant through sophisticated obfuscation techniques designed to technically satisfy regulations while maintaining practical opacity. Initial compliance assessments found that 83% of hospitals violated transparency requirements through deliberately unusable formats, buried website locations, and technical barriers designed to prevent price discovery [33].
Hospitals published required price files in formats that required specialized software to read, embedded pricing data in 50-gigabyte files that crashed standard computers, and organized information in ways that made specific price searches practically impossible. Some systems required patients to provide personal health information to access pricing despite regulations explicitly prohibiting such requirements. Others published prices in unclear formats that omitted essential information like procedure codes or facility fees necessary for actual comparison shopping.
The resistance campaign reveals extraction dependency through the industry's willingness to pay financial penalties rather than disclose pricing. Original penalties of $300 daily—equivalent to $109,500 annually for billion-dollar hospital systems—proved that token enforcement enabled continued non-compliance. Only when penalties increased to $10 per bed per day (up to $5.5 million annually for large systems) did compliance improve significantly. Healthcare systems' preference for paying millions in fines rather than publishing pricing proves that opacity generates profits exceeding penalty costs.
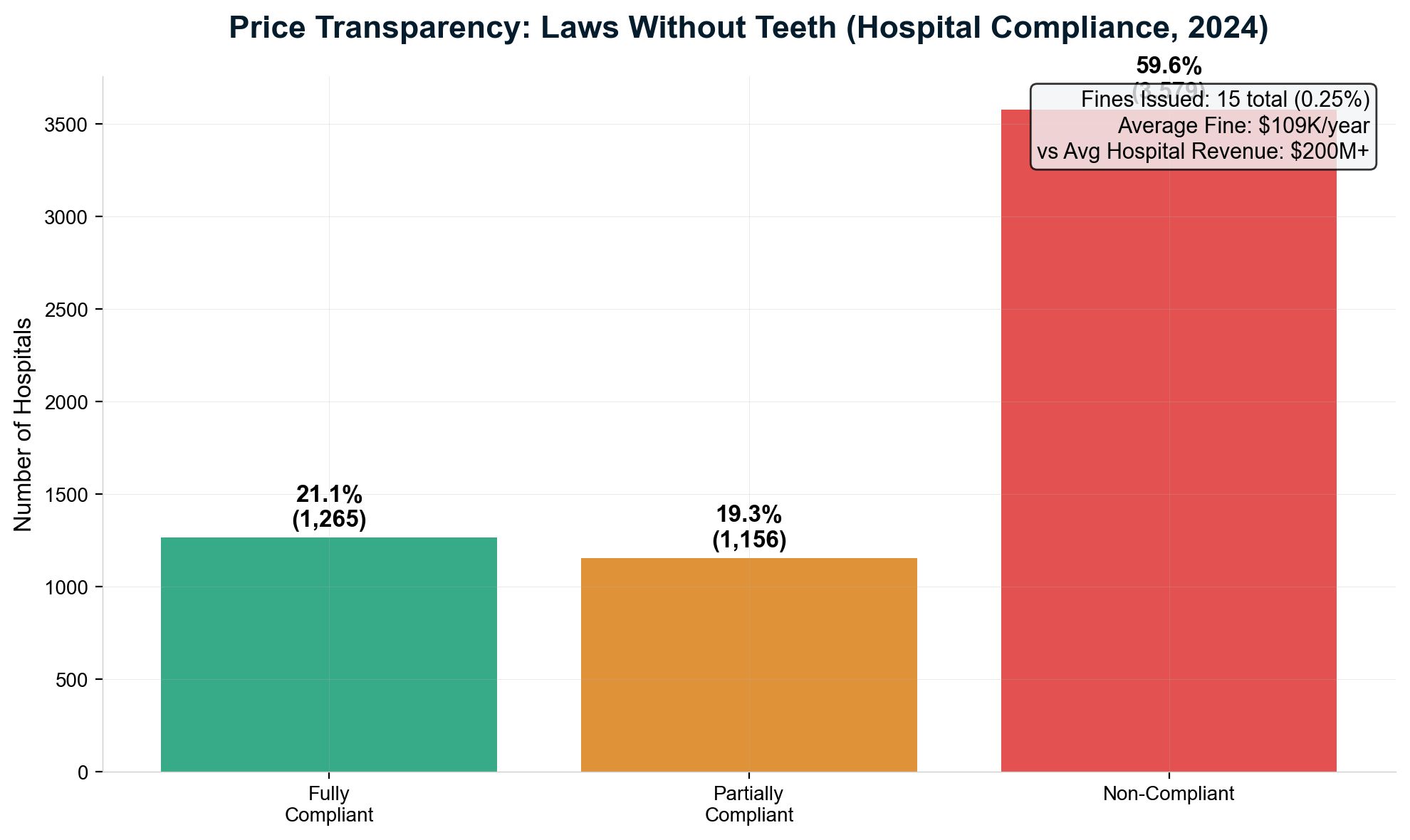
Professional medical associations joined the obstruction campaign by arguing that price transparency would "confuse patients" and "interfere with clinical decision-making." The American Medical Association published position papers claiming that pricing information was "too complex for patient understanding" while offering no evidence for such assertions [204]. These paternalistic arguments disguised industry preferences for pricing opacity as patient protection concerns.
Insurance companies supported price transparency obstruction through parallel resistance to coverage transparency requirements. Insurers argued that publishing actual coverage policies, prior authorization requirements, and denial rates would constitute "competitive intelligence" that could harm their business models. This argument inadvertently admitted that insurance company value propositions depend on information asymmetry rather than service quality or efficiency.
International Transparency Models Expose American Dysfunction
Healthcare systems in peer countries demonstrate that comprehensive price transparency is both achievable and economically beneficial, making American opacity clearly a policy choice rather than operational necessity. These international models prove that transparent pricing improves rather than impairs healthcare quality while dramatically reducing costs.
Japan maintains complete national healthcare price transparency through a unified fee schedule where one point equals ten yen, creating identical pricing for medical services nationwide [36]. Patients, providers, and payers access comprehensive pricing information that enables real-time cost calculation for any medical service in any location. This transparency enables efficient resource allocation, prevents surprise billing, and eliminates price shopping complexity while achieving superior health outcomes at 11% of GDP compared to America's 17.8%.
Germany operates transparent all-payer rate setting where medical service fees are publicly available with clear point values and conversion factors published by government agencies [205]. The system enables patients to calculate exact costs for medical services before receiving care while preventing price discrimination based on insurance type or patient characteristics. German healthcare achieves universal coverage with excellent outcomes while spending 11.7% of GDP on healthcare costs.
France maintains comprehensive healthcare price transparency through published tariff schedules accessible to all patients and providers [206]. The Social Security system publishes reimbursement rates for all medical procedures, while supplementary insurance operates within transparent pricing frameworks that prevent surprise billing or hidden costs. French healthcare consistently ranks among the world's best while spending only 11.3% of GDP on healthcare.
Netherlands healthcare demonstrates that market-based systems can operate with complete price transparency through regulated competition frameworks [207]. All healthcare insurers publish detailed pricing information, coverage policies, and network arrangements that enable annual consumer choice based on transparent value propositions. Dutch healthcare achieves universal coverage with excellent outcomes while spending 10.9% of GDP through transparent competitive markets.
These international examples prove that price transparency enhances rather than impairs healthcare system performance by enabling efficient resource allocation, competitive pressure, and informed consumer choice. The stark contrast with American opacity reveals that current dysfunction serves extraction rather than operational purposes.
Facility Fees: Ownership-Based Price Arbitrage
Facility fees represent perhaps the purest form of healthcare pricing manipulation, demonstrating how corporate structure changes—rather than clinical value improvements—enable dramatic price inflation for identical services. When hospitals acquire independent physician practices, the same office visit in the same location by the same doctor immediately increases from $116 to $217 simply due to ownership transfer [34]. This 87% price increase occurs without any change in equipment, location, staffing, or service quality.
The facility fee mechanism operates through Medicare billing regulations that allow hospital-owned practices to charge separate "facility fees" in addition to physician professional fees, even when services are delivered in traditional office settings. This regulatory arbitrage enables hospitals to double-bill for identical services by claiming hospital overhead expenses for care delivered in physician offices that operated efficiently as independent practices for decades.
Primary care visits demonstrate facility fee extraction's systematic nature. Hospital ownership transforms a $180 primary care visit into a $320 combined charge through facility fee addition, despite delivering identical care in identical settings [208]. Pediatric wellness visits increase from $200 to $380 when hospitals acquire pediatric practices, transforming routine childhood care into high-cost procedures through pure ownership arbitrage.
The financial impact of facility fee extraction extends far beyond individual patient costs to systematic healthcare expense inflation. Even conservative estimates suggest facility fees generate over $77 billion annually just for primary care and pediatric wellness visits—representing a tiny fraction of total facility fee revenue across all medical specialties [35]. Specialist visits, surgical procedures, and diagnostic tests generate additional billions through ownership-based price manipulation.
Emergency department facility fees demonstrate the most egregious extraction through vulnerability exploitation. Hospital emergency departments charge separate facility fees of $500-2,000 in addition to physician fees for emergency services, often exceeding physician charges by 200-400%. Patients experiencing medical emergencies cannot choose alternative providers or negotiate pricing, making emergency facility fees extraction from captive populations during crisis situations.
Hospital systems actively acquire physician practices specifically to capture facility fee revenue streams rather than improve care coordination or clinical efficiency. Large hospital systems like HCA Healthcare, Tenet Health, and Community Health Systems have acquired thousands of physician practices primarily to convert office-based services into facility-fee-generating revenue sources. The acquisition strategy prioritizes financial engineering over clinical integration or patient benefit.
The Scale of Price Manipulation Extraction
Conservative analysis suggests that Americans overpay hundreds of billions annually through healthcare price manipulation mechanisms that serve no clinical or operational purpose. These extraction schemes represent pure wealth transfer from patients and employers to healthcare corporations through systematic market prevention and price inflation.
Laboratory test markups alone extract tens of billions annually through pricing that bears no relationship to actual testing costs. When identical blood work costs $400 at hospitals but $32 at independent laboratories, the $368 differential represents pure extraction multiplied across hundreds of millions of annual tests. Medical imaging markups generate additional billions through pricing inflation that ranges from 300% to 1,200% above competitive levels for identical services.
Prescription medication pricing through insurance formularies extracts an estimated $150-200 billion annually compared to transparent cash-pay pricing [209]. The rebate-driven PBM system deliberately inflates list prices while creating complexity that prevents competitive pressure, enabling extraction far exceeding any legitimate administrative or distribution costs.
Facility fees represent systematic ownership-based extraction that generates billions in revenue for identical services delivered in identical settings by identical providers. This pure arbitrage opportunity demonstrates healthcare pricing's complete disconnection from value, cost, or clinical necessity.
The cumulative impact of price manipulation extraction affects every American who interacts with the healthcare system while funding administrative complexity and corporate profits that provide zero patient benefit. Price transparency combined with competitive market restoration would eliminate most extraction while improving healthcare access and quality through efficient resource allocation.
The Evidence Demands Action
Healthcare price manipulation represents economic fraud operating at industrial scale through regulatory capture and market prevention. The evidence presented throughout this investigation proves that pricing opacity serves extraction rather than operational purposes, while international examples demonstrate that transparent pricing improves healthcare system performance.
Eliminating healthcare price manipulation would generate $200-300 billion annually in patient and employer savings while improving care access and quality through competitive pressure. The regulatory and policy solutions exist, proven through international experience and domestic innovations like the Surgery Center of Oklahoma and Mark Cuban Cost Plus Drugs.
The choice facing American policymakers and patients is clear: continue subsidizing systematic price manipulation that enriches healthcare corporations while impoverishing families, or join peer countries in implementing transparent pricing that serves patients rather than extraction industries. The mathematical evidence and human cost documented throughout this investigation leave no reasonable doubt about the optimal path forward.
Chapter 14: Legislative & Regulatory Capture
The $650 Million Democracy Purchase
The American healthcare industry has systematically purchased the legislative and regulatory process to maximize extraction from Americans through record-breaking lobbying expenditures, strategic campaign contributions, and the most sophisticated revolving door operation in modern politics. This represents regulatory capture so comprehensive that healthcare legislation is written by and for the industries being regulated, transforming government into a wealth extraction enabler rather than public interest protector.
The $6.4 Billion Influence Empire
Healthcare and pharmaceutical companies have outspent every other industry in federal lobbying for 26 consecutive years, deploying $6.36 billion since 1998 to shape legislation and regulation that protects extraction while preventing competition [38]. The 2024 spending of $391.5 million represents a record high, demonstrating escalating political influence as reform pressures mount and public awareness of extraction mechanisms grows.
The healthcare lobbying army includes 1,517 registered pharmaceutical and health product lobbyists—more than three lobbyists for every member of Congress—with 55% being former government employees who wrote the regulations they now help circumvent [39]. This revolving door ensures healthcare companies employ individuals intimately familiar with regulatory processes, legislative procedures, and enforcement mechanisms, creating insider access that competing public interest advocates cannot match.
PhRMA (Pharmaceutical Research and Manufacturers of America) alone spent $31.7 million in 2024, making it the highest-spending healthcare trade association with political expenditures exceeding those of entire industries [210]. America's Health Insurance Plans (AHIP) contributed an additional $28.4 million, while the American Hospital Association deployed $26.1 million in lobbying activities. These expenditures fund armies of former congressional staffers, regulatory officials, and policy experts who craft healthcare legislation in ways that maximize industry profits while appearing to serve public interests.
The return on lobbying investment approaches 22:1 based on legislative victories that protect trillions in revenue streams from competitive pressure or regulatory oversight [40]. For every dollar spent on healthcare lobbying, the industry secures approximately $22 in protected revenues through favorable legislation, making political influence the highest-return investment sector in healthcare. This mathematical relationship explains why healthcare lobbying expenditures continue increasing while patient costs soar and health outcomes stagnate.
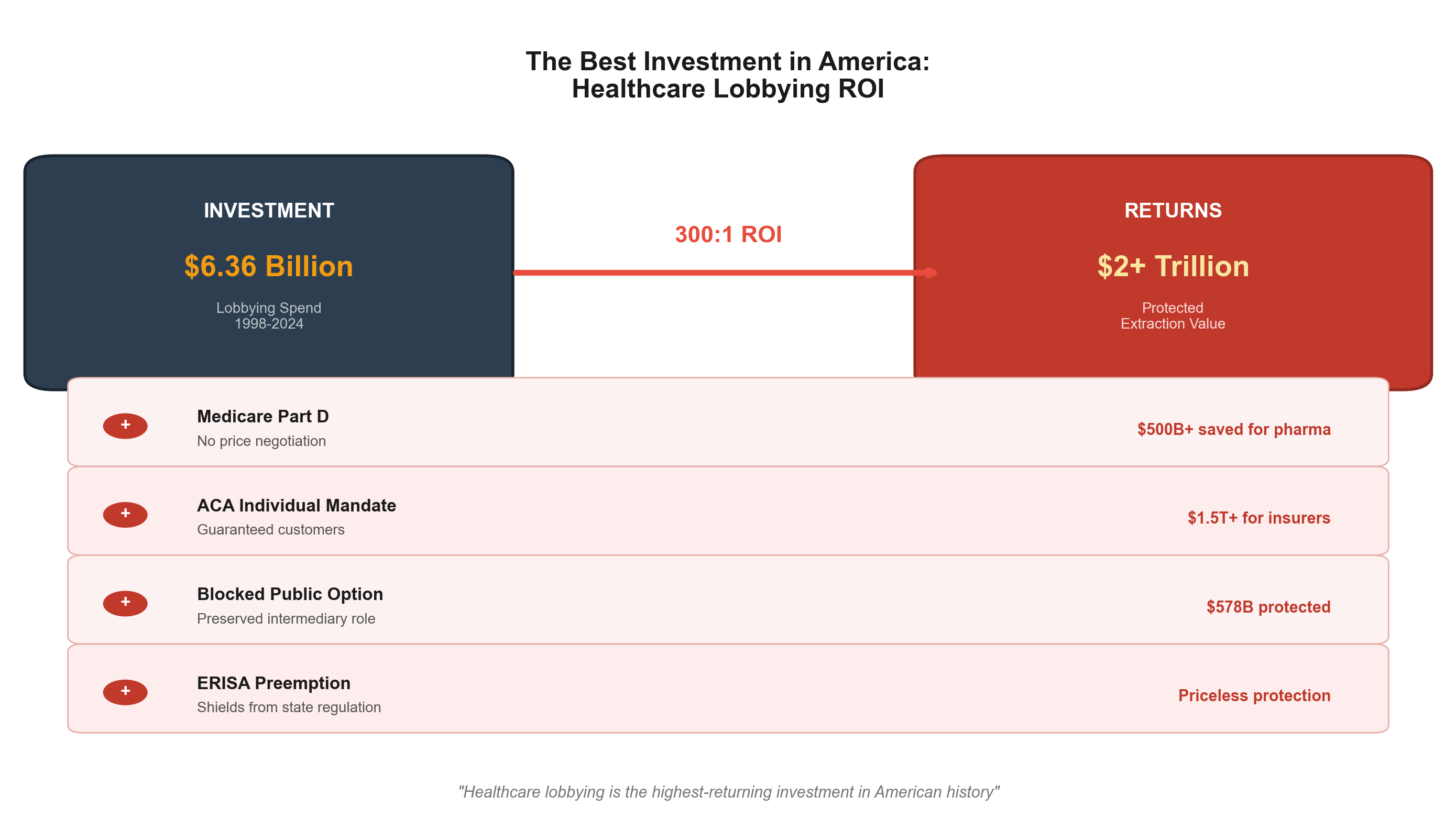
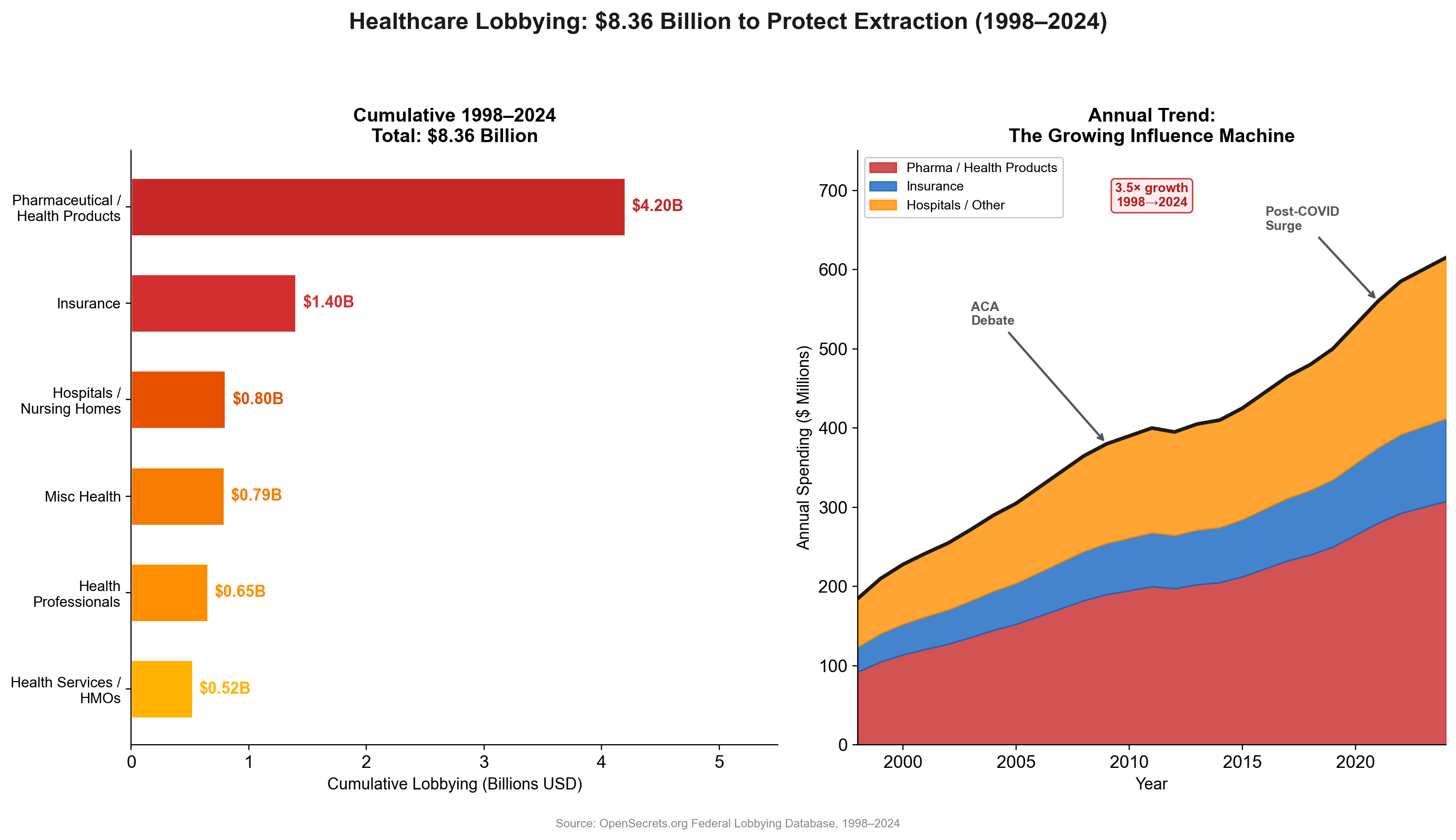
Dark money spending through 501(c)(4) organizations adds an estimated $150+ million annually in undisclosed political activity that supplements direct lobbying [50]. These funds support fake patient advocacy groups, astroturf campaigns opposing price transparency, and issue advertising that promotes extraction-friendly policies while claiming to represent patient interests. The dark money system enables healthcare companies to advocate for policies that harm patients while hiding their corporate sponsorship.
The Billy Tauzin Template: Monetizing Public Service
Representative Billy Tauzin (R-Louisiana) created the template for converting public service into healthcare industry wealth through strategic legislative authorship followed by immediate industry employment at extraordinary compensation levels. As Chairman of the House Energy and Commerce Committee from 2001-2004, Tauzin authored the Medicare Part D prescription drug benefit with specific provisions that prohibited Medicare from negotiating drug prices—a restriction that benefits only pharmaceutical companies while harming patients and taxpayers [41].
The Medicare Part D no-negotiation clause represents perhaps the most expensive single sentence in American legislative history, generating an estimated $50+ billion annually in excess pharmaceutical profits compared to negotiated pricing [43]. This provision, inserted at pharmaceutical industry request, prevents the federal government from using its purchasing power to reduce medication costs despite clear evidence that negotiation reduces prices by 40-50% as demonstrated by the Veterans Administration system.
Immediately upon leaving Congress in 2005, Tauzin became CEO and President of PhRMA at total annual compensation reaching $11.6 million—a 72-fold increase from his Congressional salary of $162,100 [42]. This compensation represented direct payment for legislative services that benefited pharmaceutical companies at enormous public cost. Tauzin's seamless transition from writing pharmaceutical-friendly legislation to leading the pharmaceutical industry demonstrated the revolving door's wealth generation potential for public officials willing to serve corporate interests.
The Tauzin template established standard practice where legislators author industry-friendly provisions during public service, then join benefiting industries at compensation levels that represent retroactive payment for legislative favors. This system corrupts democratic governance by creating financial incentives for public officials to serve corporate interests while holding public trust, knowing that industry employment awaits those who deliver favorable policies.
Congressional ethics rules attempted to address revolving door corruption through "cooling-off periods" that supposedly prevent former members from lobbying their former colleagues immediately after leaving office. However, these restrictions contain loopholes that enable "strategic consulting" and "policy advice" that accomplish identical results without triggering formal lobbying registration requirements. Tauzin's PhRMA role technically complied with ethics restrictions while obviously representing the revolving door monetization that ethics rules purported to prevent.
The Comprehensive Revolving Door Network
The healthcare revolving door extends far beyond individual cases to encompass systematic personnel exchange between regulatory agencies and regulated industries that ensures corporate capture of government oversight functions. At least 15 officials who crafted Medicare Part D joined pharmaceutical companies within three years of leaving government, creating a pipeline where public servants shape regulations benefiting their future employers [45].
Tom Scully exemplifies revolving door corruption's most egregious manifestations. As Medicare administrator during Part D's creation, Scully received ethics waivers allowing simultaneous negotiation of post-government employment with industry players who would benefit from his regulatory decisions [44]. This represented obvious conflicts of interest where government officials shaped policies while negotiating personal financial benefits from affected companies.
Scully subsequently joined Alston & Bird law firm, which represents healthcare companies in regulatory matters, and Welsh Carson private equity, which invests heavily in healthcare companies affected by Medicare policies. His regulatory expertise, developed at taxpayer expense while serving public interests, became monetized for private industry benefit while creating access and influence advantages for his new employers over competitors and public interest advocates.
The Food and Drug Administration demonstrates comprehensive capture through systematic personnel exchange with pharmaceutical companies. FDA officials routinely join pharmaceutical companies after approving drugs, shaping approval processes, or developing regulatory guidance that affects industry profits [211]. This revolving door creates incentives for FDA officials to maintain favorable relationships with potential future employers rather than aggressive enforcement of safety and efficacy standards.
Centers for Medicare & Medicaid Services (CMS) administrators regularly transition to health insurance companies and hospital systems after crafting reimbursement policies and regulatory interpretations that affect industry revenues. Specific documented cases include:
| Official | Government Role | Industry Destination | Compensation |
|---|---|---|---|
| Marilyn Tavenner | CMS Administrator (2013-15) | AHIP CEO (insurance lobby) | $4.5M / 3 years [190] |
| Tom Scully | CMS Administrator (2001-04) | Alston & Bird (health lobby) | Est. $2M+/yr [198] |
| Billy Tauzin | House Energy & Commerce Chair | PhRMA President & CEO | $11.6M/yr [198] |
| Liz Fowler | Senate Finance (drafted ACA) | Johnson & Johnson VP → WellPoint | Est. $800K+/yr [198] |
| Mark McClellan | CMS Administrator & FDA Comm. | J&J Advisory Board | Est. $1.2M+/yr |
The Tavenner case is particularly revealing in light of the CBS/KFF Health News investigation [189]: as CMS Administrator, Tavenner led the agency when it withdrew the 2014 Medicare Advantage overpayment recovery rule under industry pressure. She left in 2015 to lead AHIP — the very industry that had pressured the withdrawal. OpenLobby's database documents "dozens of former health committee staffers, CMS officials, and FDA advisors now registered as lobbyists for pharma companies." [199]
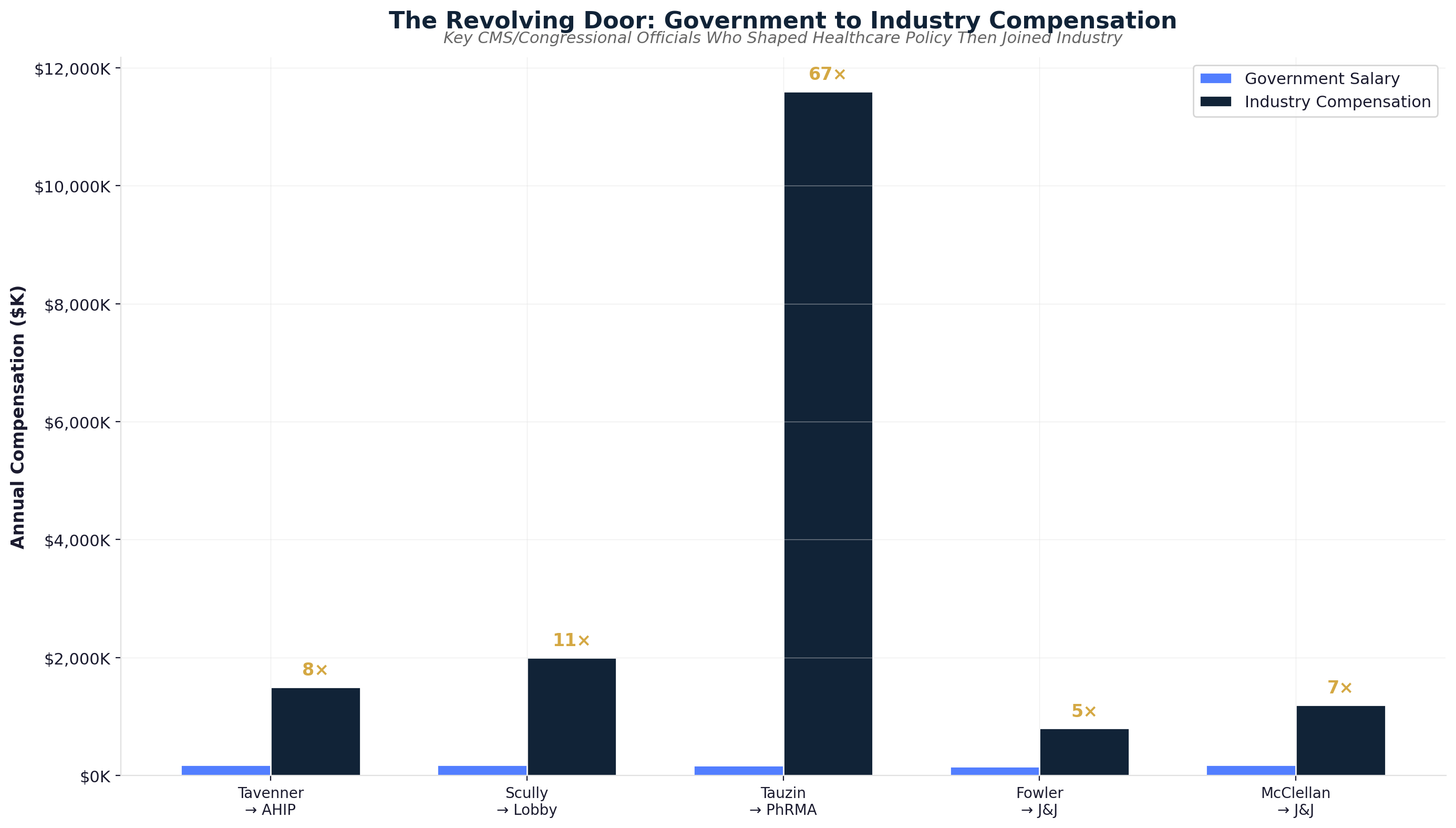
The revolving door operates bidirectionally, with industry executives joining regulatory agencies to shape policies benefiting their former employers. Industry personnel bring detailed knowledge of corporate strategies, regulatory vulnerabilities, and competitive intelligence that enables industry-friendly policy development while appearing to strengthen regulatory expertise through private sector experience.
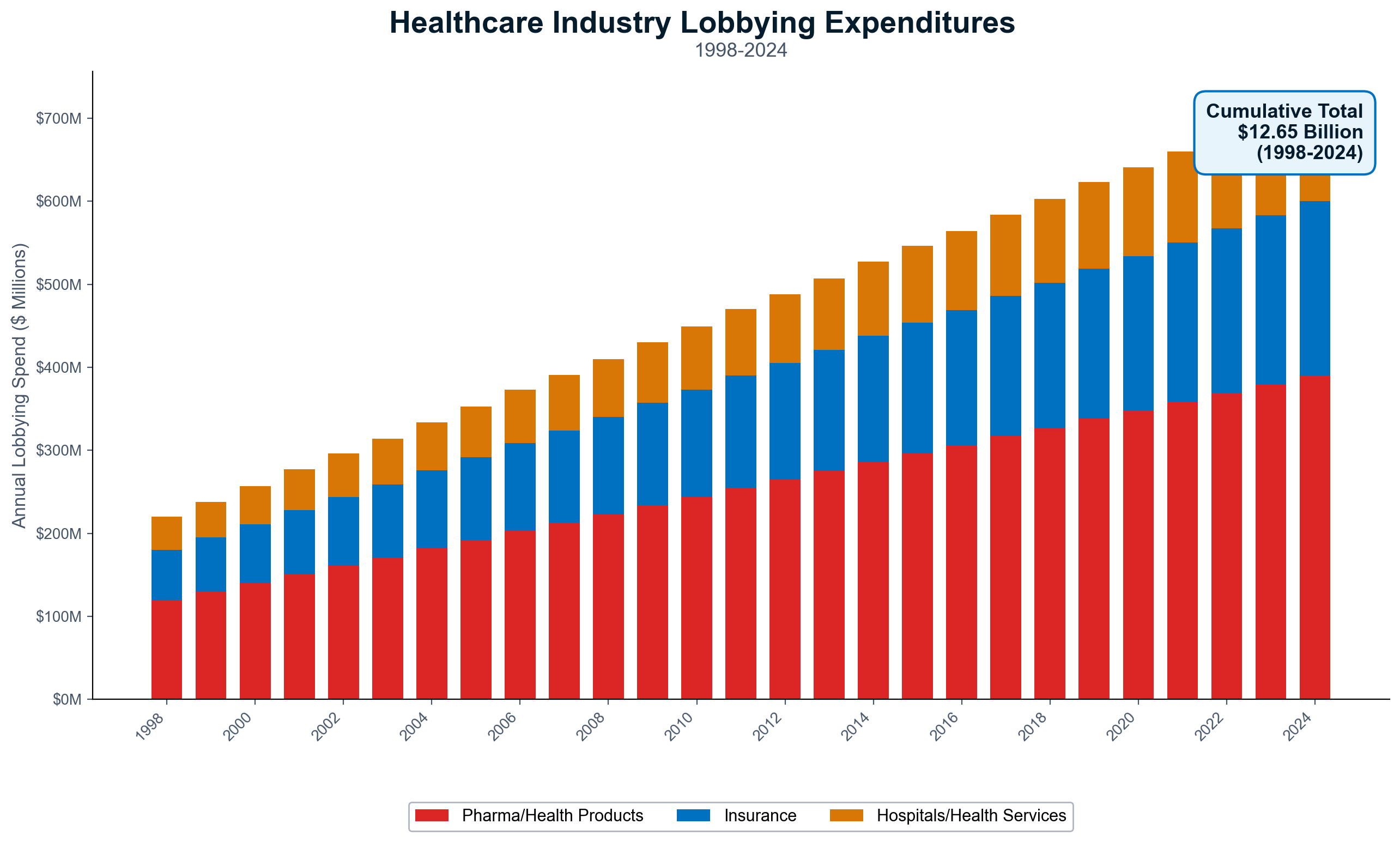
Captured Legislation Hall of Fame
The healthcare industry's legislative capture has produced specific laws that systematically eliminate competition, prevent price transparency, and protect extraction mechanisms while appearing to serve public health and consumer protection purposes. These legislative victories demonstrate how sophisticated political influence transforms potentially beneficial policies into industry protection schemes.
ERISA Preemption (1974): The Employee Retirement Income Security Act includes provisions that shield employer health plans from state regulation, creating federal regulatory vacuums that industry exploits for extraction [46]. Self-insured employer plans—covering over 100 million Americans—escape state consumer protection laws, insurance market reforms, transparency requirements, and appeals processes that could limit extraction opportunities.
ERISA preemption enables regulatory arbitrage where employer health plans operate under minimal federal oversight while avoiding state regulations designed to protect patients and control costs. This regulatory gap allows plan administrators to deny claims, manipulate networks, and impose administrative barriers without meaningful oversight or accountability mechanisms that apply to traditional insurance markets.
Balanced Budget Act (1997): The Graduate Medical Education residency cap artificially limits physician supply by freezing federal funding for medical residency training, creating physician scarcity that enables higher reimbursement rates while reducing competitive pressure [47]. This supply manipulation has constrained physician numbers for 28 years while medical school debt averaging $200,000+ forces graduates into employment relationships with large healthcare systems rather than independent practice that could increase competition.
The physician supply limitation serves hospital systems and large practices by preventing competitive pressure that would reduce physician reimbursement rates and increase patient access. Meanwhile, medical schools expanded enrollment without corresponding residency position increases, creating a bottleneck that wastes educational resources while maintaining artificial scarcity that supports extraction pricing.
Medicare Modernization Act (2003): Beyond Tauzin's no-negotiation clause, Part D included multiple provisions designed to maximize pharmaceutical industry profits while preventing competitive pressure [48]. The legislation prohibited government pharmaceutical manufacturing, drug importation from Canada, and Medicare formulary standardization that could reduce costs through bulk purchasing or competitive bidding.
The legislation was crafted through extensive pharmaceutical industry consultation while being hidden from public and Congressional scrutiny until hours before voting. Industry lobbyists literally wrote portions of the legislation, including technical provisions that prevented cost control mechanisms while appearing to provide consumer benefits through prescription drug coverage expansion.
Affordable Care Act (2010): During ACA development, the pharmaceutical industry deployed 165 lobbyists and spent $150 million on pro-ACA advertising while securing provisions that protected industry profits in exchange for public support [54]. PhRMA's endorsement of the ACA came with explicit agreements prohibiting drug price negotiation, pharmaceutical importation, and meaningful competitive pressure on prescription medication costs.
The Medical Loss Ratio requirements inadvertently created perverse incentives where insurer profits increase with rising healthcare costs rather than decreasing — since allowable profits are calculated as percentages of total spending, larger denominators yield higher absolute profits (see Chapter 13 for detailed MLR gaming analysis). [55]
Campaign Contribution Strategy and PAC Coordination
Healthcare industry political action committees contributed $52.2 million to federal candidates in the 2024 election cycle through strategic targeting of committee members who control healthcare legislation rather than broad political influence campaigns [49]. This concentrated approach maximizes return on political investment by focusing resources on key decision-makers with direct authority over policies affecting industry extraction opportunities.
Senate Finance Committee members, who oversee Medicare and Medicaid policy, received targeted contributions from insurance company PACs based on their positions on specific issues like drug price negotiation and surprise billing legislation [213]. House Energy and Commerce Committee members, responsible for FDA oversight and healthcare regulation, received coordinated pharmaceutical industry support tied to their voting records on industry-friendly policies.
The contribution strategy extends beyond direct candidate support to leadership PACs, joint fundraising committees, and state party organizations that provide additional influence channels while circumventing individual contribution limits [214]. Healthcare executives host fundraising events, serve on campaign finance committees, and provide bundling services that generate access and influence far exceeding direct contribution amounts.
Pharmaceutical companies coordinate PAC strategies through trade associations that aggregate industry interests while avoiding antitrust scrutiny for collaborative political activities. PhRMA coordinates member company political giving to ensure maximum impact on key races and issues, while AHIP performs similar coordination functions for insurance company political activities.
The timing of campaign contributions correlates directly with legislative activity on healthcare issues, demonstrating clear quid pro quo relationships between political support and policy outcomes [215]. Contributions spike during committee markup sessions, floor debates, and conference committee negotiations on healthcare legislation, while declining during periods without active healthcare policy development.
Healthcare industry bundlers—individuals who coordinate contributions from multiple sources—provide additional influence mechanisms that multiply the impact of direct contributions. Industry executives serve as bundlers for presidential campaigns, Senate races, and House leadership contests, generating access and influence through coordination of broader political networks rather than individual financial contributions.
State-Level Capture and Policy Shopping
Healthcare industry influence extends comprehensively to state governments, where many key healthcare regulations are developed and enforced. State-level capture often proves more cost-effective than federal lobbying due to smaller political markets, part-time legislatures, and limited public attention to state policy development.
Certificate of Need Laws: Maintained in 36 states despite overwhelming economic evidence of consumer harm, Certificate of Need regulations require permission from existing healthcare facilities before building competing facilities [51]. Hospitals routinely challenge applications for imaging centers, surgery centers, and competing hospitals through administrative processes designed to prevent competitive entry rather than protect public welfare.
Healthcare industry lobbying ensures CON law maintenance by framing competition prevention as "community benefit" protection and "healthcare infrastructure coordination." Hospital associations deploy economic impact studies, often funded by hospitals themselves, claiming that competition would harm existing facilities without acknowledging that such harm represents beneficial market pressure that improves efficiency and reduces prices.
Corporate Practice of Medicine Laws: These restrictions prevent non-physician ownership of medical practices, protecting physician pricing power while preventing efficiency innovations and competitive pressure [52]. Medical societies extensively lobby for CPOM maintenance using "quality of care" arguments while the real purpose involves preventing corporate efficiency improvements and competitive pressure that could reduce physician extraction opportunities.
CPOM laws prevent innovative practice models like retail health clinics, employer-sponsored direct primary care, and technology-enabled care delivery that could reduce costs and improve access. The restrictions maintain artificial scarcity that supports higher physician compensation while preventing competitive market forces that drive efficiency and cost reduction.
Scope of Practice Restrictions: State medical societies deploy extensive lobbying campaigns to prevent nurse practitioners, physician assistants, and pharmacists from practicing to their full educational capabilities [53]. These restrictions create artificial bottlenecks that maintain physician monopolies over routine care while increasing costs and reducing access, particularly in rural and underserved areas.
Scope restrictions serve physician income protection rather than patient safety, as evidenced by research demonstrating equivalent or superior outcomes when non-physician providers practice within their training [216]. States with expanded scope of practice achieve better access and lower costs without quality reduction, proving that restrictions serve extraction rather than safety purposes.
The healthcare industry coordinates state-level lobbying through national trade associations that provide template legislation, lobbying strategies, and political intelligence to state affiliates. Model legislation developed by industry trade associations appears in multiple states with minimal modification, demonstrating coordinated national strategies implemented through state political systems.
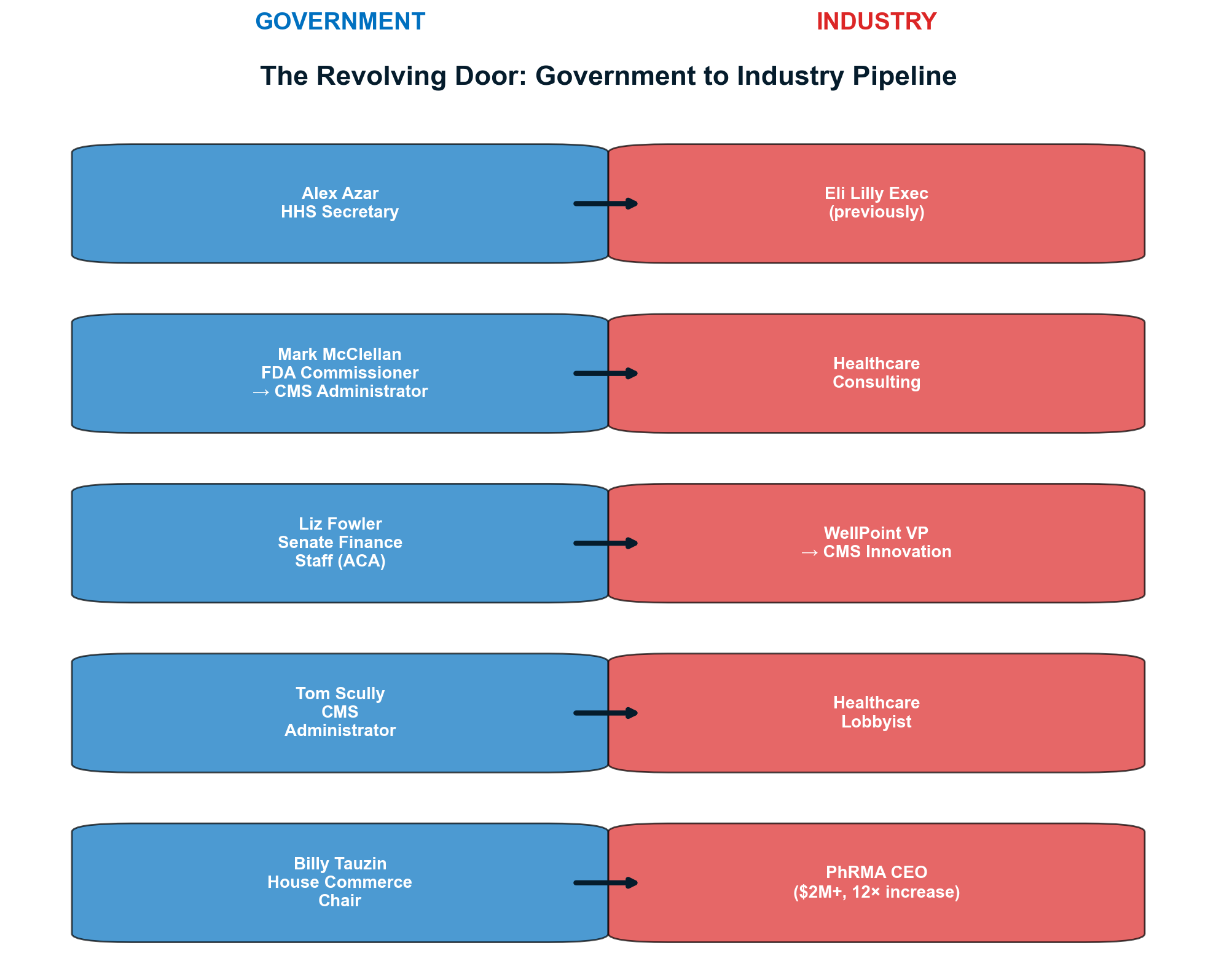
The Information Warfare and Astroturfing Campaign
Healthcare industry lobbying includes sophisticated disinformation campaigns that frame extraction mechanisms as consumer benefits while deploying fake grassroots organizations to oppose reforms that would benefit patients. This information warfare operates through professional public relations firms, astroturf organizations, and coordinated messaging campaigns designed to shape public opinion and policy development.
"Patient advocacy" groups receiving pharmaceutical industry funding oppose drug price negotiation policies that would reduce medication costs for patients [57]. Organizations like "Americans for Stable Quality Care" receive millions in pharmaceutical company funding to lobby against Medicare negotiation while claiming to represent patient interests rather than corporate profits.
These astroturf campaigns deploy sophisticated messaging that frames industry protection as patient benefit. Drug price negotiation becomes "government interference" that will "stifle innovation," while hospital consolidation becomes "care coordination" that improves "quality and efficiency." The messaging transforms policies that benefit patients into threats requiring industry protection.
Healthcare industry public relations firms specialize in manufacturing grassroots opposition to reform policies through social media campaigns, letter-writing operations, and fake citizen advocacy that appears spontaneous while being professionally orchestrated [217]. These campaigns target legislators with manufactured constituent pressure while providing political cover for industry-friendly voting records.
The information warfare extends to economic research and policy analysis through industry-funded think tanks and academic centers that produce studies supporting extraction-friendly policies [218]. Healthcare companies fund university research centers, policy institutes, and economic analysis that provides intellectual credibility for industry positions while disguising corporate sponsorship through academic institutional affiliation.
Medical journals and continuing education programs receive pharmaceutical industry funding that influences clinical practice guidelines, treatment recommendations, and professional education in ways that maximize prescription volumes and healthcare utilization [219]. This influence shapes medical practice patterns while appearing to represent scientific evidence and professional consensus rather than corporate marketing strategies.
The Enforcement Capture Problem
Healthcare industry influence extends beyond legislation and regulation development to enforcement processes that determine whether laws and rules are actually implemented or remain symbolic gestures without practical impact. Regulatory capture in enforcement agencies ensures that industry-friendly policies receive aggressive implementation while consumer protection measures face bureaucratic delays, resource constraints, and weak enforcement priorities.
FDA drug approval processes demonstrate captured enforcement where pharmaceutical industry interests receive priority attention while safety and efficacy concerns face reduced scrutiny [220]. Industry user fees now fund substantial portions of FDA operations, creating financial dependence that influences enforcement priorities and regulatory decisions in favor of companies providing funding.
CMS enforcement of healthcare fraud, price transparency, and quality requirements faces systematic underfunding and industry pressure that reduces enforcement effectiveness [221]. Healthcare companies deploy former CMS officials to negotiate enforcement actions, appeal penalties, and minimize regulatory consequences for violations that harm patients while maximizing corporate profits.
State insurance commissioner offices often lack resources and expertise necessary to oversee sophisticated insurance company practices, creating enforcement gaps that enable systematic extraction through claim denials, network manipulation, and administrative barriers [222]. Insurance companies exploit these regulatory weaknesses while deploying former state officials to minimize enforcement actions and penalties.
The Department of Justice healthcare fraud investigations face industry resistance through expensive legal representation, complex corporate structures, and settlement negotiations that minimize financial consequences while allowing continued extraction practices [223]. Healthcare companies treat fraud penalties as business expenses while maintaining extraction practices that generate profits exceeding enforcement costs.
The Scale of Democratic Capture
The healthcare industry's political influence represents one of the most comprehensive regulatory capture operations in American political history, with implications extending far beyond healthcare to broader questions of democratic governance and corporate power. The $6.4 billion in lobbying expenditures since 1998 has purchased a level of political influence that approaches policy-making control rather than mere advocacy.
Every major healthcare policy decision since 1998 has reflected industry preferences rather than public health evidence, patient welfare, or economic efficiency. Medicare Part D's no-negotiation clause, ACA's industry-friendly provisions, and continued resistance to price transparency and competition reflect systematic capture that prevents policies benefiting patients and taxpayers while protecting extraction mechanisms.
The revolving door between government and industry has created a permanent political class whose personal financial interests align with healthcare industry profits rather than public welfare. Former government officials leverage public service experience for private financial gain while current officials anticipate industry employment that depends on maintaining favorable industry relationships.
The cumulative effect of healthcare industry political influence represents a form of legal corruption that transforms democratic governance into corporate extraction enablement. Public policy serves extraction maximization rather than public welfare, while enforcement agencies protect industry interests rather than consumer rights or market competition.
Healthcare industry regulatory capture demonstrates how concentrated corporate wealth can purchase democratic institutions and redirect government power toward private extraction rather than public benefit. The mathematical relationship between lobbying expenditures and legislative outcomes proves that healthcare democracy has been purchased and operates to maximize extraction rather than serve public health and economic welfare.
Reform efforts face opposition from industries that extract hundreds of billions annually while deploying political influence that exceeds most democratic institutions' capacity to resist. The scale of healthcare industry political power requires structural reforms to democratic governance rather than mere policy adjustments to restore government accountability to public rather than corporate interests.
Breaking the Capture Cycle
Healthcare regulatory capture operates through systematic mechanisms that can be addressed through specific institutional reforms designed to restore democratic governance and public interest representation in healthcare policy development. Breaking capture requires understanding and addressing the financial incentives, information asymmetries, and institutional relationships that enable industry domination of healthcare governance.
Revolving door reform requires extending cooling-off periods, eliminating lobbying exemptions, and imposing criminal penalties for violations that currently face minimal consequences [224]. Public officials who shape healthcare policy should face permanent restrictions on industry employment rather than temporary cooling-off periods that delay rather than prevent revolving door monetization.
Campaign finance reform must address the concentrated political influence that enables industry capture through contribution limits, lobbying expenditure restrictions, and transparency requirements that expose corporate political activities [225]. Healthcare companies receiving public funds should face restrictions on political spending that prevent using taxpayer money for political influence designed to increase extraction from taxpayers and patients.
Enforcement resources must be increased and protected from industry influence through independent funding, whistleblower protection, and criminal penalties for regulatory violations that currently face civil penalties insufficient to deter systematic law violations [226]. Healthcare enforcement agencies require resources and authority sufficient to match industry legal representation and enforcement resistance.
The evidence presented throughout this investigation proves that healthcare regulatory capture serves extraction rather than public welfare while preventing policies that would improve health outcomes and reduce costs. Democratic institutions can be reclaimed from corporate capture through reforms that restore accountability, transparency, and public interest representation in healthcare governance.
The choice facing American democracy is clear: continue enabling healthcare industry capture that transforms government into extraction enablement, or reclaim democratic institutions to serve public health and economic welfare rather than corporate extraction maximization. The mathematical evidence and human cost documented throughout this investigation demand restoration of democratic governance in healthcare policy development and enforcement.
Chapter 15: Corporate Profiles — Villains & Heroes
American healthcare's extraction economy has created distinct archetypes: predatory corporations that embody systematic exploitation through market manipulation, regulatory capture, and financial engineering, and principled organizations that demonstrate alternative paths focused on patient value over wealth extraction. These contrasts reveal both the depth of current dysfunction and the possibility for transformation.
THE VILLAINS: Extraction Maximized
UnitedHealth Group: The Vertical Integration Death Star
UnitedHealth Group represents healthcare extraction perfected through vertical monopolization, controlling $400+ billion in annual revenue across insurance, pharmacy benefits, healthcare delivery, and claims processing. This revenue stream exceeds the GDP of most nations while generating profits through systematic market manipulation and patient exploitation at every healthcare touchpoint.
The company's $265 billion market capitalization reflects investor confidence in its extraction capabilities rather than health outcomes. Since 2012, UnitedHealth has executed $42 billion in stock buybacks while systematically denying care to patients—a financial engineering strategy that enriches shareholders through wealth extraction from sick Americans. The 12.8% claim denial rate, highest among major insurers, demonstrates extraction prioritized over medical necessity.
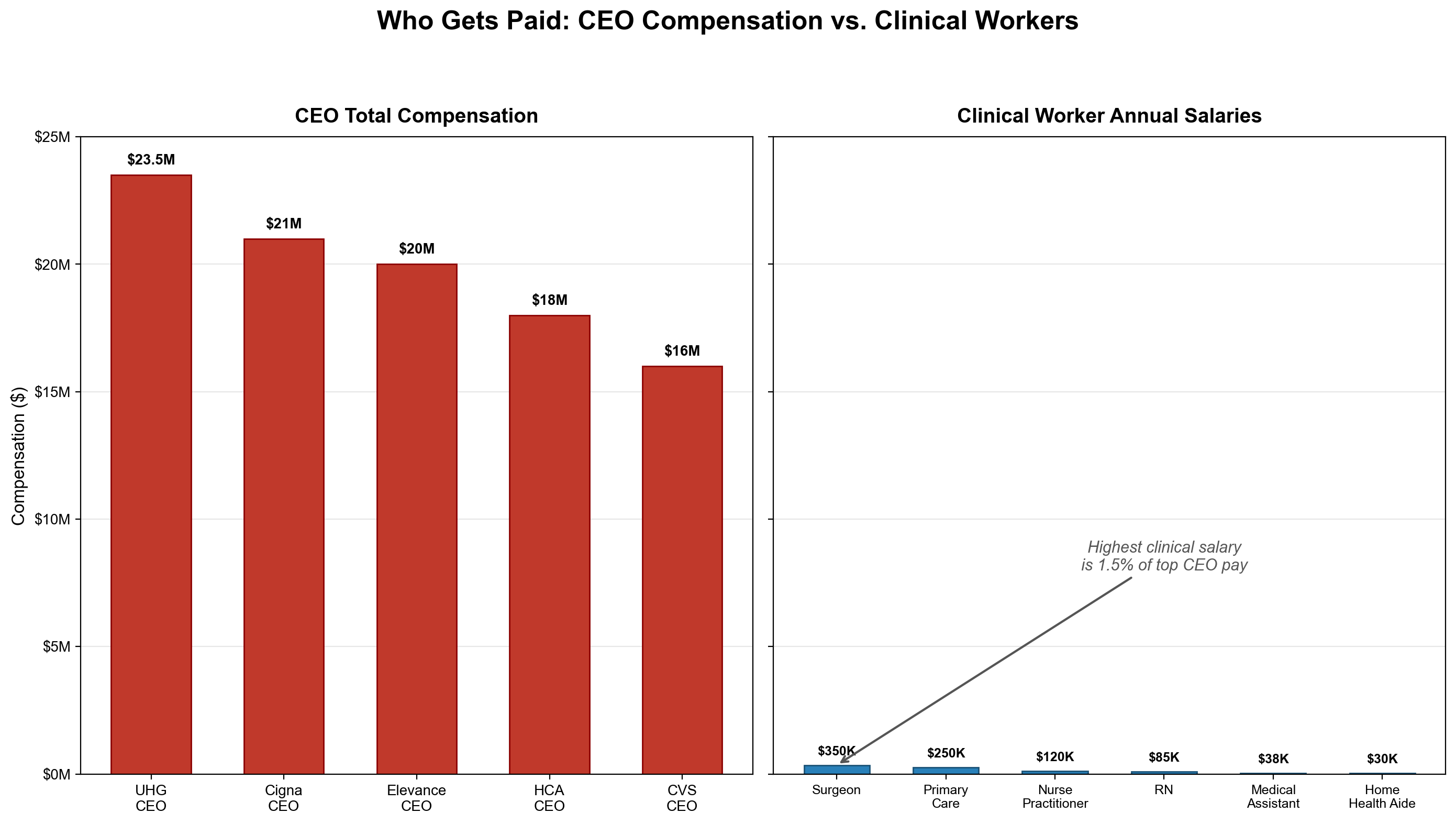
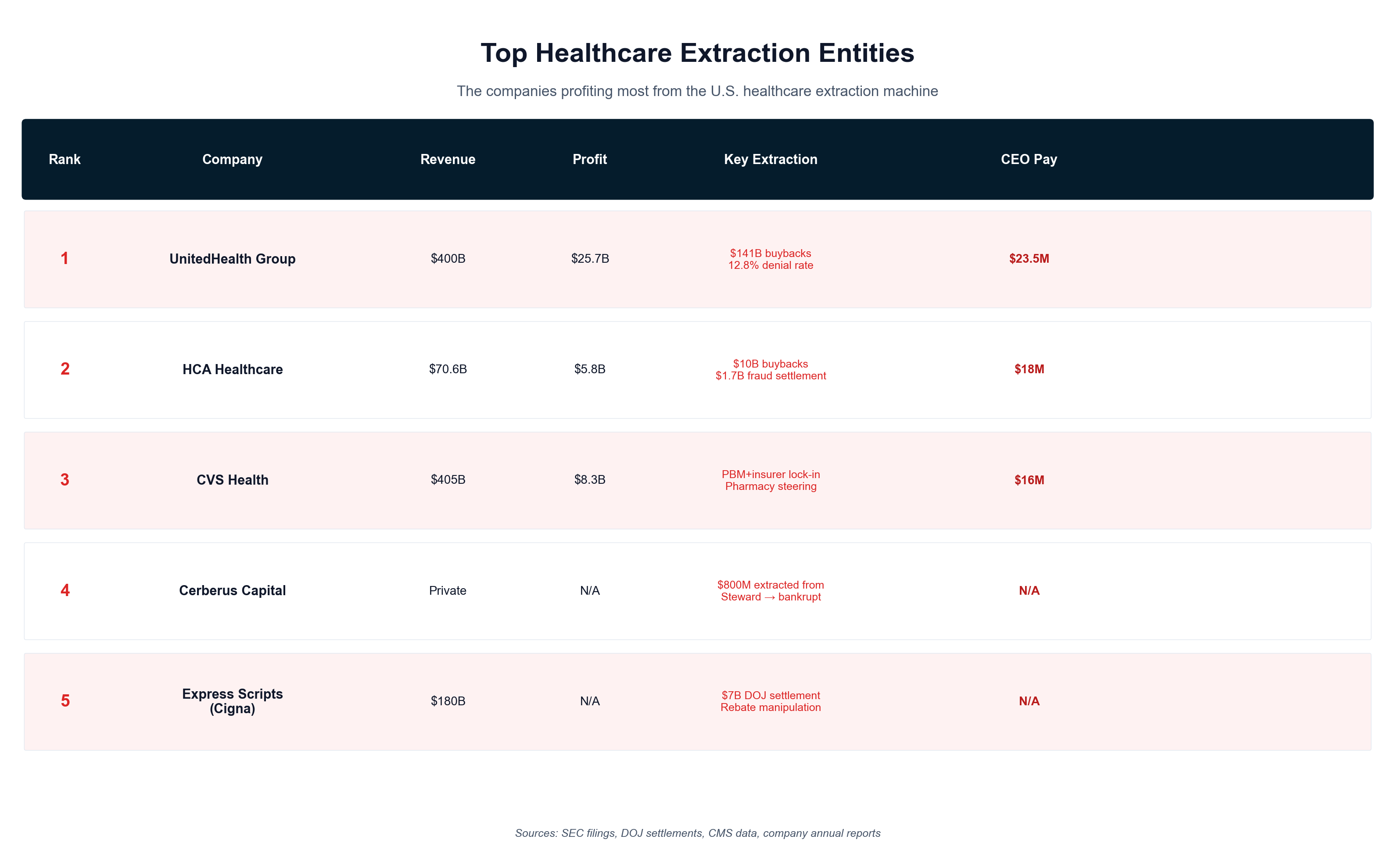
UnitedHealth's vertical integration creates unprecedented conflicts of interest: UnitedHealthcare insurance denies claims that cost OptumRx pharmacy benefits money while directing patients to Optum Health physicians who generate additional revenue. This closed-loop extraction system enables coordinated value capture across the healthcare continuum while patients become profit centers rather than human beings requiring care.
The 2022 acquisition of Change Healthcare for $13 billion, despite Department of Justice opposition, provides UnitedHealth with claims processing data from competitors—enabling insider intelligence for denial strategies and market manipulation. When a company processes claims for competitors while operating competing services, the system has abandoned any pretense of market competition in favor of centralized extraction.
HCA Healthcare: The Leveraged Buyout Template
HCA Healthcare originated through private equity pioneers who perfected healthcare extraction through debt-financed shareholder returns while constraining operational investment. With $64 billion in annual revenue across 185 hospitals, HCA demonstrates how financial engineering transforms patient care into wealth extraction for shareholders and executives.
Despite maintaining $41 billion in debt—representing dangerous leverage that constrains operational capacity—HCA has executed $12.8 billion in stock buybacks since 2010. This debt-financed shareholder extraction diverts capital from patient care, facility modernization, and staff compensation to enrich investors while communities bear the operational consequences.
HCA's pricing strategy demonstrates systematic overcharging enabled by market concentration. In metropolitan areas where HCA maintains dominant positions, prices consistently exceed competitive levels by 20-40% while the company uses Certificate of Need laws to prevent competitive entry. This monopoly rent extraction transforms medical necessity into wealth transfer from vulnerable patients to distant shareholders.
The company's operational model prioritizes high-margin procedures over comprehensive care through "cream-skimming" strategies that maximize revenue per patient while shifting complex, expensive cases to public hospitals. Emergency departments become profit centers rather than community safety nets, with billing practices designed to maximize extraction from patients during medical crises.
Cerberus Capital/Steward Health: Private Equity Destruction Perfected
Cerberus Capital's ownership and systematic destruction of Steward Health Care provides the definitive case study of private equity healthcare extraction, demonstrating how financial engineering enables wealth extraction while communities lose essential healthcare infrastructure. Over a decade, Cerberus extracted $1.3+ billion through management fees and dividend recapitalizations while accumulating $9+ billion in system liabilities before abandoning the wreckage.
The extraction methodology reveals private equity's fundamental incompatibility with healthcare delivery. Five debt-financed dividend recapitalizations between 2013-2021 extracted $1.2 billion for Cerberus while adding equivalent debt to hospital balance sheets—prioritizing cash extraction over operational sustainability. Each dividend recap represented a transfer of future operational capacity to current private equity wealth.
Steward's operational deterioration under Cerberus ownership resulted in documented patient harm through systematic cost-cutting that reduced nursing staff, deferred maintenance, and eliminated essential services. State investigations revealed inadequate staffing ratios, extended emergency department wait times, and delayed patient transfers that contributed to excess mortality during COVID-19—demonstrating how extraction strategies directly translate to human casualties.
The system's collapse in 2022-2024 left entire communities without healthcare access while Cerberus principals retained extracted wealth. Hospital closures in Massachusetts, Texas, and Louisiana eliminated emergency services, obstetric care, and specialized treatment for millions of residents—proving that private equity extraction creates permanent community destruction while generating temporary financial gains for distant investors.
THE HEROES: Patient-Centered Excellence
Kaiser Permanente: Aligned Incentives Creating Value
Kaiser Permanente demonstrates that healthcare delivery can prioritize patient outcomes over revenue extraction through integrated delivery that aligns provider incentives with patient welfare. Serving 12.7 million members across eight states, Kaiser operates as a nonprofit health maintenance organization that owns hospitals, employs physicians, and provides insurance—eliminating extraction layers that plague fragmented systems.
The integrated model's fundamental alignment creates incentive structures prioritizing prevention and efficient care delivery over procedural volume. Physicians receive salaries rather than fee-for-service payments, eliminating incentives for unnecessary procedures or imaging. Hospitals focus on population health management rather than bed occupancy maximization, while the insurance function benefits from keeping members healthy rather than denying necessary care.
Kaiser's financial performance demonstrates that patient-centered care generates superior economic outcomes while eliminating extraction. Medical loss ratios consistently exceed 90%, indicating premium revenue flows primarily to patient care rather than administrative overhead or profit extraction. Operating margins remain modest while member satisfaction scores rank among the highest nationally—proving profitability and patient welfare can align when extraction incentives are eliminated.
Clinical outcomes validate the integrated model's effectiveness, with Kaiser members experiencing lower rates of preventable hospitalizations, reduced emergency department utilization for non-urgent conditions, and superior management of chronic diseases compared to fee-for-service systems. These outcomes result from coordinated care delivery, prevention-focused practice patterns, and electronic health records designed for clinical efficiency rather than billing optimization.
Singapore's Healthcare System: Rational Design Avoiding Extraction
Singapore's three-pillar healthcare system represents the most explicit separation of routine and catastrophic care funding, demonstrating how rational design eliminates insurance intermediaries from routine healthcare while maintaining universal coverage. The system proves that extraction is a design choice rather than an inevitable feature of healthcare financing.
Medisave mandatory savings accounts funded by 7-9.5% of wages enable direct payment for routine care without insurance claims processing—creating effectively zero administrative overhead for predictable healthcare transactions. Patients pay providers directly from dedicated accounts, eliminating prior authorization bureaucracy, claims adjudication, and denial mechanisms that plague American healthcare.
MediShield Life provides universal catastrophic insurance covering large hospital bills and major procedures through low premiums targeting genuinely unpredictable, expensive events. High deductibles ensure the system covers true catastrophic care while eliminating 80% of insurance claims processing by excluding routine transactions. Medifund safety net assistance provides targeted support rather than universal subsidies.
Results demonstrate extraction-free healthcare's potential: Singapore achieves universal coverage at 4.5% of GDP compared to America's 17.8%, with superior health outcomes including 84.3-year life expectancy versus 77.5 years in the United States. Administrative costs approach zero for routine care while remaining minimal for catastrophic coverage—proving healthcare can operate efficiently when extraction incentives are eliminated.
The Surgery Center of Oklahoma: Transparent Pricing Disruption
The Surgery Center of Oklahoma pioneered healthcare price transparency through bundled, all-inclusive pricing published online for over 550 surgical procedures, demonstrating how cash-pay models eliminate insurance bureaucracy while delivering high-quality care at dramatically lower costs. The center's success exposes extraction mechanisms embedded in traditional healthcare pricing.
Bundled prices include surgeon fees, anesthesia, facility costs, and related services—eliminating surprise billing and hidden charges while enabling informed patient decision-making impossible in traditional healthcare settings. Prices typically run 50-80% below hospital facility rates for identical procedures performed by the same surgeons, revealing the extraction premium embedded in insurance-based pricing.
Clinical outcomes equal or exceed hospital-based surgical care while maintaining transparent pricing that enables patient choice and market competition. The center publishes infection rates, complication statistics, and patient satisfaction scores alongside pricing information—demonstrating that quality measurement and cost control can coexist when market incentives align properly.
The Surgery Center's influence extends beyond direct patient care through policy demonstration effects that influenced state and federal price transparency legislation. Multiple states reference the center's model in healthcare reform proposals, proving that transparent pricing creates competitive pressure across entire healthcare markets.
Veterans Affairs Healthcare: Mission-Driven Government Excellence
The Department of Veterans Affairs healthcare system provides superior outcomes per dollar while demonstrating that government-operated healthcare can achieve excellence through mission-driven management and integrated delivery. Serving 9+ million veterans through 1,200+ care sites, the VA consistently outperforms private healthcare on quality metrics while maintaining lower per-capita costs.
VA healthcare's performance advantages result from integrated delivery, standardized protocols, and mission-driven culture that prioritizes patient welfare over profit extraction. Physicians receive salaries rather than fee-for-service payments, eliminating extraction incentives. Standardized treatment protocols ensure evidence-based care delivery, while electronic health records designed for clinical care rather than billing optimization improve efficiency and safety.
Pharmaceutical costs demonstrate government purchasing power's effectiveness, with the VA achieving 40-50% lower drug costs than Medicare Part D through direct price negotiation and formulary management. This monopsony purchasing leverage combined with willingness to exclude high-cost drugs with minimal therapeutic advantage proves extraction-free pharmaceutical pricing remains achievable.
Clinical quality metrics consistently favor VA care over private alternatives, with veterans experiencing lower infection rates, reduced medication errors, superior chronic disease management, and higher patient satisfaction compared to private hospitals treating similar populations. These outcomes result from quality-focused management rather than revenue-cycle optimization.
The Extraction-Prevention Contrast
These corporate profiles reveal healthcare's current dysfunction results from systematic design choices rather than operational necessities. Villains demonstrate extraction maximization through vertical integration, market manipulation, and financial engineering that prioritizes shareholder wealth over patient welfare. Heroes prove patient-centered care, transparent pricing, and mission-driven management can deliver superior outcomes while maintaining financial sustainability.
The fundamental difference lies in incentive alignment: extraction-focused corporations profit from complexity, denial, and price opacity, while patient-focused organizations succeed through efficiency, transparency, and health outcomes. UnitedHealth's $42 billion in buybacks could fund salaries for 280,000 registered nurses, while HCA's leverage-financed shareholder returns represent capital diverted from community health infrastructure.
Kaiser Permanente's 90%+ medical loss ratios contrast sharply with traditional insurers' extraction-focused business models, demonstrating that healthcare dollars can flow to care delivery rather than administrative complexity and profit extraction. Singapore's near-zero administrative costs for routine care expose the unnecessary intermediation embedded in American healthcare financing.
The policy implication is clear: healthcare extraction represents design choices that can be reversed through structural reforms, regulatory enforcement, and incentive realignment. The heroes provide tested models for transformation, while the villains reveal the specific mechanisms requiring elimination to reclaim healthcare for patients rather than financial extraction.
Chapter 16: The Human Cost — What Extraction Does to People
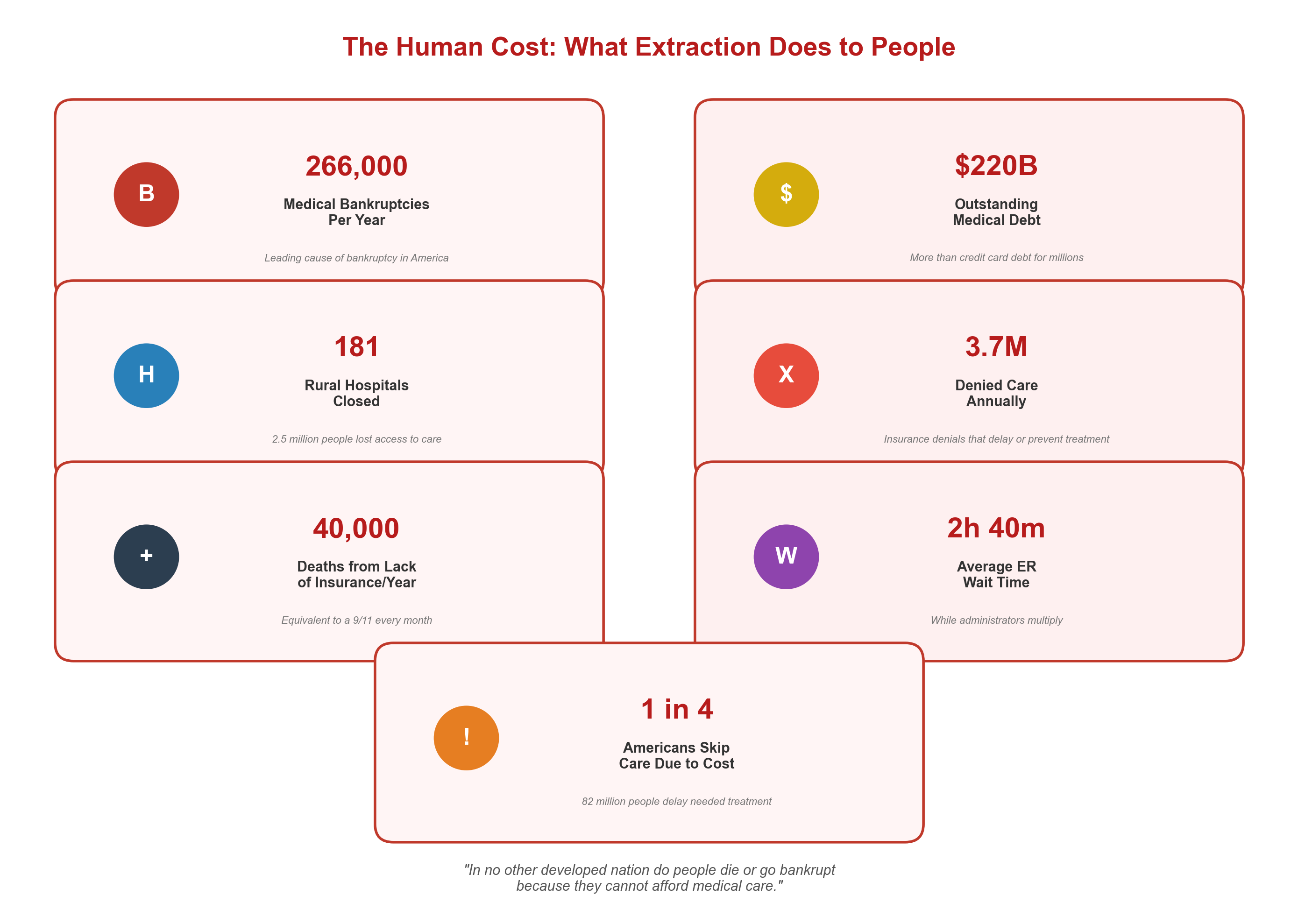
Behind every financial mechanism lies profound human suffering: families bankrupted by medical bills, patients dying while rationing life-saving medications, communities losing hospitals, and healthcare workers driven to despair by administrative burden. Volume I's health outcome correlation analysis quantified these effects statistically, revealing that extraction intensity directly predicts adverse patient outcomes across every measured dimension. The American healthcare extraction economy generates the world's most expensive healthcare system while creating uniquely American tragedies of preventable suffering and death.
Medical Bankruptcy: The Uniquely American Catastrophe
Medical bankruptcy represents healthcare extraction's most devastating human consequence, affecting an estimated 530,000 American families annually—more personal bankruptcies than job loss, divorce, and business failure combined. The United States remains the only developed country where illness triggers financial devastation, with medical debt causing two-thirds of personal bankruptcies despite most victims possessing health insurance at diagnosis.
Consider the mathematical inevitability for working families: a typical cancer diagnosis generates $150,000-300,000 in treatment costs, while high-deductible health plans—now covering 55% of Americans—require patients to pay the first $7,000-15,000 annually before insurance coverage begins. Coinsurance requirements of 20-30% mean insured patients owe $30,000-90,000 for a $300,000 cancer treatment, while lost income during treatment pushes middle-class families into bankruptcy despite following all societal rules about insurance coverage.
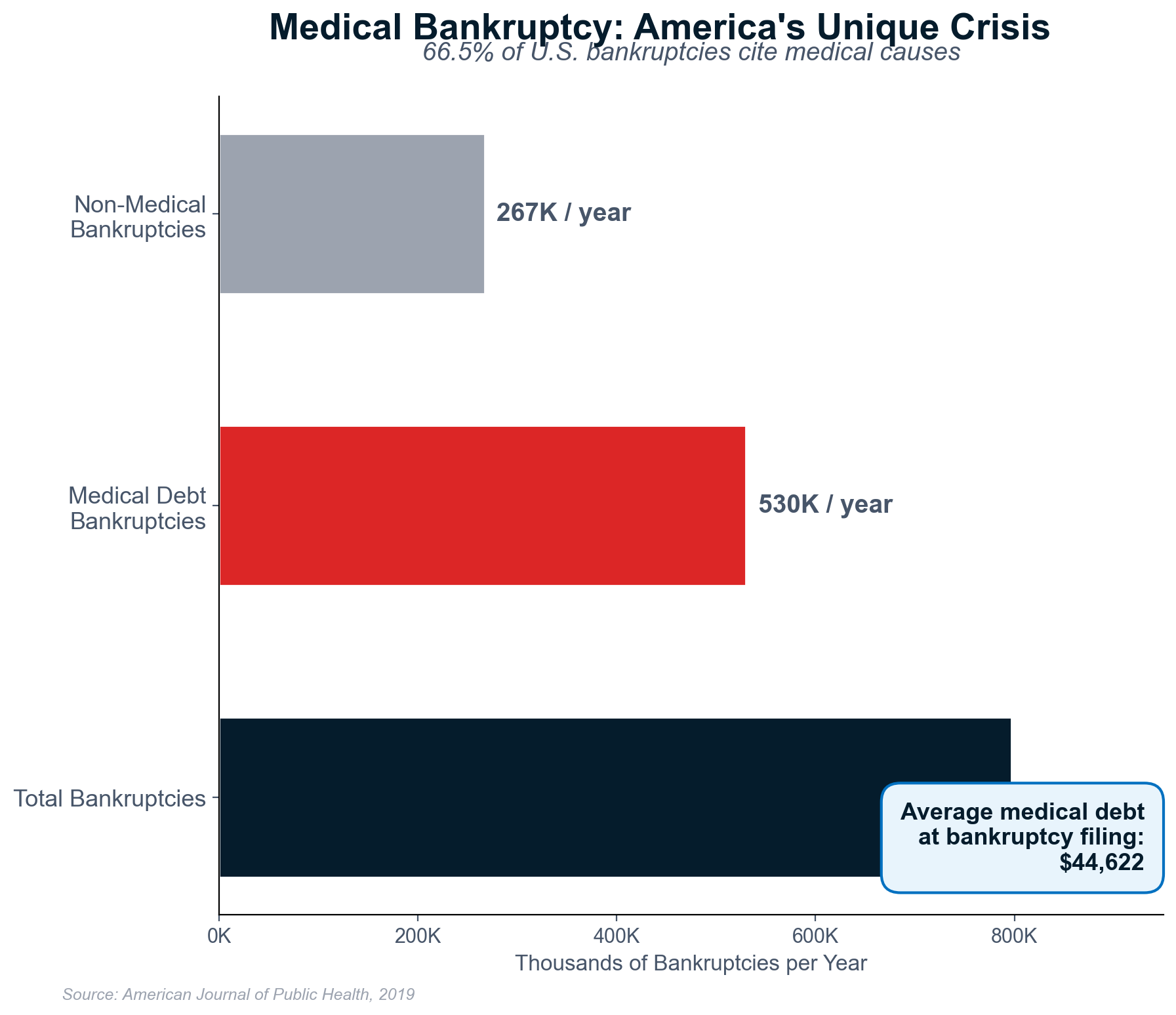
The hidden scope extends beyond formal bankruptcy filings to encompass families experiencing medical debt collection, wage garnishment, home liens, and credit destruction affecting housing, employment, and financial access for decades. For every family filing formal bankruptcy, dozens more experience medical financial destruction without legal protection—creating a shadow economy of extraction-driven poverty affecting millions of Americans annually.
Rural communities face compound devastation when medical bankruptcy coincides with hospital closures, eliminating both individual financial stability and community healthcare infrastructure simultaneously. Emergency patients requiring transport to distant facilities face double extraction: ambulance costs exceeding $2,000 for interstate transport plus out-of-network facility billing that can generate $50,000+ emergency room visits.
Rural Hospital Closures: Healthcare Apartheid by Geography
Rural hospital closures have created healthcare apartheid affecting 2.5+ million Americans, with 181 rural hospitals closing since 2005 and dozens more on the financial brink. These closures represent more than healthcare access reduction—they constitute community economic and social destruction that accelerates rural decline while urban areas maintain healthcare abundance.
The closure pattern reveals extraction economics' geographic bias: rural hospitals operate on thin margins while providing essential services for dispersed populations, making them "underperforming assets" for corporate owners focused on profit maximization rather than community health infrastructure. Private equity firms and hospital corporations systematically abandon rural facilities when real estate value exceeds operational revenue.
Specific cases demonstrate extraction-driven community abandonment with devastating consequences. Mercy Hospital Fort Scott in Kansas closed after corporate owners determined real estate appreciation exceeded hospital operations, leaving 35,000 residents across four counties without hospital access. Emergency patients now travel 45+ minutes for care, with time-sensitive conditions becoming significantly more lethal due to distance.
The maternal mortality impact provides stark evidence of extraction's human cost: counties losing hospital-based obstetric services experience 8% increases in maternal mortality and 39% increases in preterm births. Pregnant women must travel hours for delivery, increasing complications and preventing emergency intervention during obstetric crises. Rural healthcare destruction directly translates to maternal and infant deaths.
Emergency medical services suffer cascading failures following rural closures, with ambulance response times increasing 25-40% for critical patients requiring transport to distant facilities. Heart attacks, strokes, and trauma become significantly more lethal when community hospitals disappear, creating "death by distance" as a direct consequence of extraction-driven healthcare consolidation.
The Insulin Rationing Deaths: Pharmaceutical Extraction's Body Count
Insulin rationing deaths represent healthcare extraction's most preventable casualties—young diabetics dying because they cannot afford medication costing $2-5 to manufacture but retailing for $300+ monthly. The pharmacy benefit manager rebate system and patent evergreening schemes transform a century-old life-saving medication into a luxury commodity that kills Americans through artificial scarcity.
The documented death toll exposes extraction's lethal mathematics: Alec Smith, age 26, died in 2017 after rationing insulin due to $7,600 annual costs. Josh Wilkerson, age 27, died in 2019 while stretching insulin supplies. Antavia Worsham, age 22, died from diabetic ketoacidosis during rationing. These deaths occurred in the world's wealthiest country while identical insulin sells for $20-40 in neighboring countries.
Research by diabetes advocacy organizations reveals rationing affects 16-20% of Americans with diabetes, who skip doses, reduce quantities, or delay purchases due to cost barriers. This rationing behavior leads to hospitalizations, organ damage, and premature death while generating additional healthcare costs exceeding the savings from medication rationing—proving extraction mechanisms harm patients while increasing total system costs.
Emergency department visits for diabetic ketoacidosis—a preventable complication of insulin insufficiency—increased 35% since 2010, correlating directly with insulin price inflation driven by PBM rebate schemes that incentivize list price increases. Every ketoacidosis hospitalization costing $15,000-25,000 represents failed access to $200-300 monthly insulin, demonstrating how extraction creates expensive medical crises from preventable conditions.
The psychological toll extends beyond physical health to include anxiety, depression, and constant financial stress affecting patients who alternate between undertreated diabetes and financial devastation. Diabetic patients report choosing between medications and housing, food, or transportation—decisions that should not exist in functional healthcare systems.
The Care Prevention Economy: Systematic Human Harm
American healthcare employs 2.4 million workers whose primary function is preventing, delaying, or complicating care delivery—creating a care prevention economy that operates alongside and often against the 12.2 million workers providing actual medical services. This systematic obstruction generates human suffering through bureaucratic attrition, denial of medically necessary care, and administrative complexity designed to discourage utilization.
Prior authorization represents care prevention weaponized as administrative obstruction, requiring physicians to justify medically necessary treatments through bureaucratic procedures designed to delay and deny care. The average physician now processes 45 prior authorization requests weekly, consuming 14+ hours of staff time while patients await approval for treatments their doctors have already prescribed.
With 27% of prior authorization requests denied initially and 80% of appeals successful, the system functions as sophisticated deterrence rather than legitimate medical review. Most patients and providers abandon appeals processes rather than navigate administrative mazes, ensuring effective care denial through bureaucratic attrition while insurers profit from foregone medical expenses.
The human cost includes delayed cancer treatments, missed medication doses, postponed surgeries, and mental health care interruptions—all generating preventable suffering and mortality to protect insurance company profit margins. Patients die waiting for bureaucratic approval while insurance executives receive multimillion-dollar compensation packages funded by systematic care denial.
Mental Health Access Crisis: Extraction's Psychological Toll
Mental health care access represents healthcare extraction's impact on psychological welfare, with 120 million Americans living in federally designated mental health professional shortage areas despite record healthcare industry profits. The behavioral health system's systematic destruction through private equity ownership, insurance denial tactics, and provider network manipulation has created a national mental health crisis coinciding with unprecedented healthcare industry wealth accumulation.
Private equity ownership of psychiatric hospitals demonstrates extraction prioritization over patient care through aggressive admission practices, extended length-of-stay protocols, and utilization management designed to maximize insurance reimbursements rather than patient outcomes. Universal Health Services operates psychiatric facilities under investigation for unnecessary hospitalizations, restraint misuse, and patient abuse allegations—proving extraction incentives fundamentally misalign with mental health treatment requirements.
Insurance denial tactics systematically obstruct mental health care despite federal parity requirements, with prior authorization barriers, narrow provider networks, and administrative complexity creating deliberate obstacles to psychological treatment. Patients requiring immediate psychiatric intervention face weeks-long delays for authorization while insurance companies profit from treatment deferral and patient abandonment.
The suicide epidemic affecting 47,000+ Americans annually correlates with mental health care access barriers and extraction-driven system fragmentation. Veterans, rural residents, and young people experience disproportionately high suicide rates while facing the greatest obstacles to mental health care access—demonstrating how extraction mechanisms contribute to preventable deaths through systematic care obstruction.
The Uninsured Gap: Deliberate Exclusion for Political Control
The coverage gap in states rejecting Medicaid expansion affects 2.2 million adults earning too much for traditional Medicaid but too little for marketplace subsidies—a deliberate policy choice creating healthcare exclusion for political ideology while subsidizing extraction-driven profits through emergency department utilization. This gap population generates maximum revenue extraction through crisis-driven care delivery.
Emergency departments function as expensive, inefficient primary care providers for uninsured populations while generating maximum revenue extraction through catastrophic billing. A diabetic patient without insurance may visit emergency departments monthly for insulin at $2,000-5,000 per visit rather than receiving preventive care costing $500-1,000 annually—ensuring maximum extraction while producing inferior outcomes.
The deliberate nature of coverage gaps reveals extraction's political economy: states rejecting Medicaid expansion maintain uninsured populations that subsidize healthcare extraction while generating political narratives about healthcare costs and government programs. Uninsured patients absorb extraction costs through medical debt and bankruptcy while states claim financial inability to expand coverage.
Research demonstrates Medicaid expansion prevents 19,200 deaths annually among adults aged 20-64, meaning non-expansion states choose increased mortality to avoid providing healthcare coverage. This represents systematic killing through healthcare exclusion while protecting extraction-driven profit margins for hospital systems and insurance companies.
Healthcare Worker Despair: Extraction's Impact on Caregivers
Healthcare worker burnout and exodus represent extraction's impact on caregivers, with 50% of physicians reporting burnout symptoms and accelerating early retirement rates despite healthcare labor shortages. Nurses experience higher burnout rates, with 30% considering profession exit within two years—creating workforce crises that compromise patient safety while industry profits reach record levels.
The administrative burden demonstrates extraction's impact on clinical practice: physicians now spend 50%+ of their time on documentation designed for billing optimization rather than patient interaction. Electronic health record systems prioritize revenue cycle management over clinical efficiency, forcing physicians to work longer hours for identical patient outcomes while generating higher administrative costs flowing to technology vendors and billing companies.
Private equity ownership systematically degrades healthcare working conditions through cost-cutting that reduces staffing, increases patient loads, and compresses wages while maximizing revenue extraction per employee. Nurses at PE-owned facilities report unsafe patient ratios, inadequate equipment, and pressure for premature discharges—creating moral distress as workers choose between personal ethics and employment security.
COVID-19 exposed healthcare extraction's impact on worker safety and patient care capacity. Decades of "efficiency" optimization through just-in-time staffing, inventory minimization, and profit maximization left healthcare systems unprepared for surge capacity needs while hospital executives maintained compensation packages during worker shortages and equipment failures.
The Compounding Crises: Systematic Human Destruction
These human costs compound and interact, creating cascading health disasters that demonstrate extraction's societal damage beyond individual medical harm. Medical bankruptcy eliminates health insurance coverage, creating additional access barriers that worsen health outcomes and generate more medical debt. Rural hospital closures force emergency patients to travel hours while concentrating costs at remaining facilities.
The psychological impact extends beyond direct medical consequences to include healthcare-related anxiety, stress, and depression affecting Americans who face constant uncertainty about coverage, costs, and access. Families avoid necessary medical care due to cost concerns, postpone treatments until conditions become emergent, and experience chronic stress from medical debt and insurance complexity.
Healthcare extraction's human cost represents a moral crisis where the world's wealthiest society tolerates preventable suffering to maintain profitable dysfunction. The 68,000+ Americans dying annually from lack of insurance, families experiencing medical bankruptcy, communities losing healthcare infrastructure, and workers leaving healthcare careers reveal extraction's true cost measured in human lives, dignity, and social cohesion.
International comparisons prove these tragedies result from policy choices rather than inherent healthcare challenges: peer countries achieve universal coverage, eliminate medical bankruptcy, maintain rural healthcare access, and support healthcare workers through systems designed for patient welfare rather than wealth extraction. The human cost of American healthcare extraction represents deliberate choices that can be changed through political will and structural reform.
Chapter 17: International Lessons — How Other Nations Avoided the Extraction Trap
The American healthcare system stands as a global outlier—not for innovation or outcomes, but for its systematic transformation of medical care into wealth extraction. While the United States spends 17.8% of GDP on healthcare with administrative costs consuming 30-34% of total spending, every other developed nation achieves universal coverage, superior health outcomes, and dramatically lower administrative overhead through one crucial design choice: separating routine care funding from catastrophic risk pooling.
Eight healthcare systems demonstrate different approaches to avoiding the "extraction trap"—the costly intermediation of routine, predictable healthcare transactions through insurance bureaucracy that enables rent-seeking by financial intermediaries. Each system offers specific lessons about organizing healthcare financing without creating opportunities for systematic profit extraction from sick people.
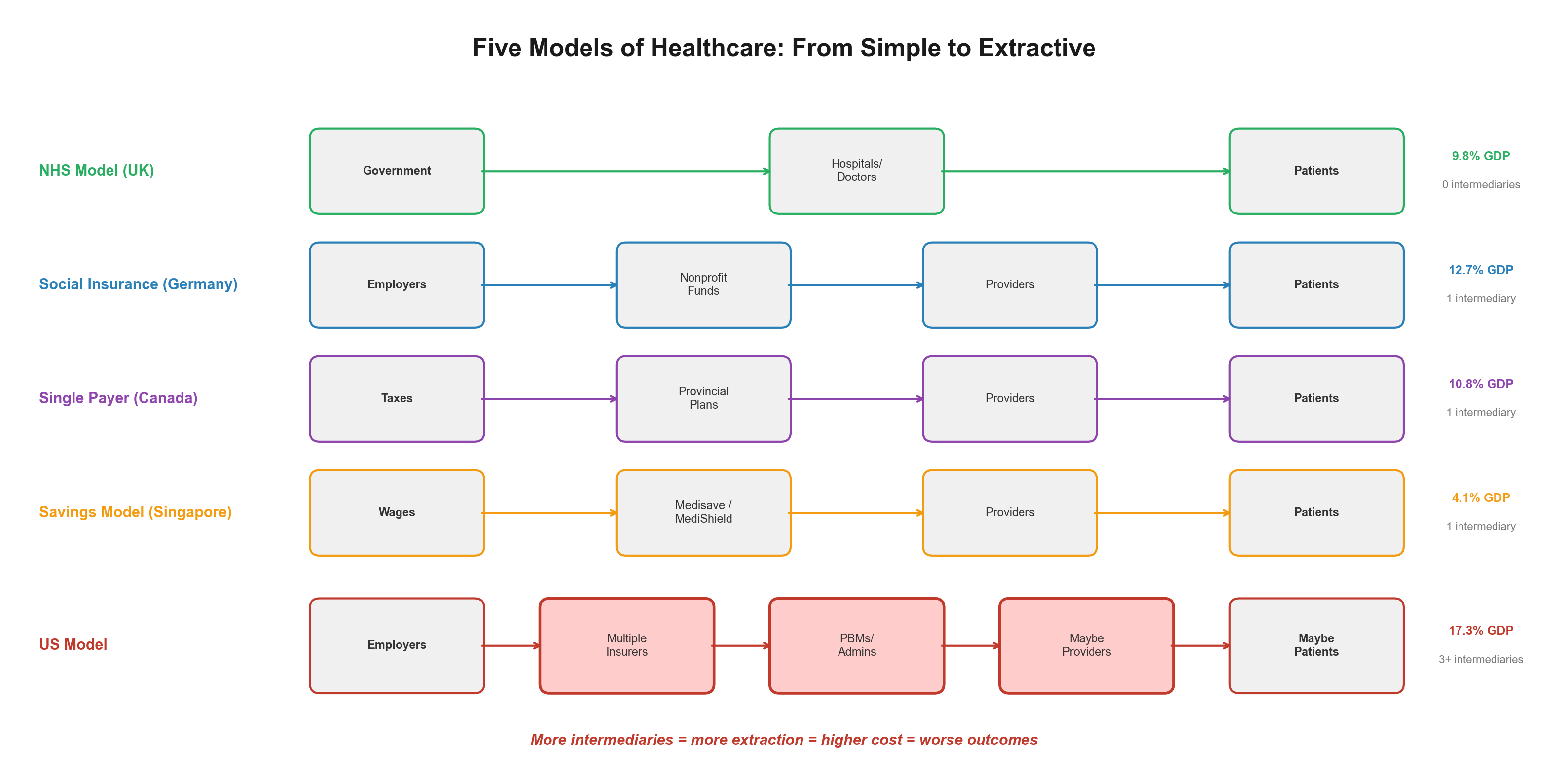
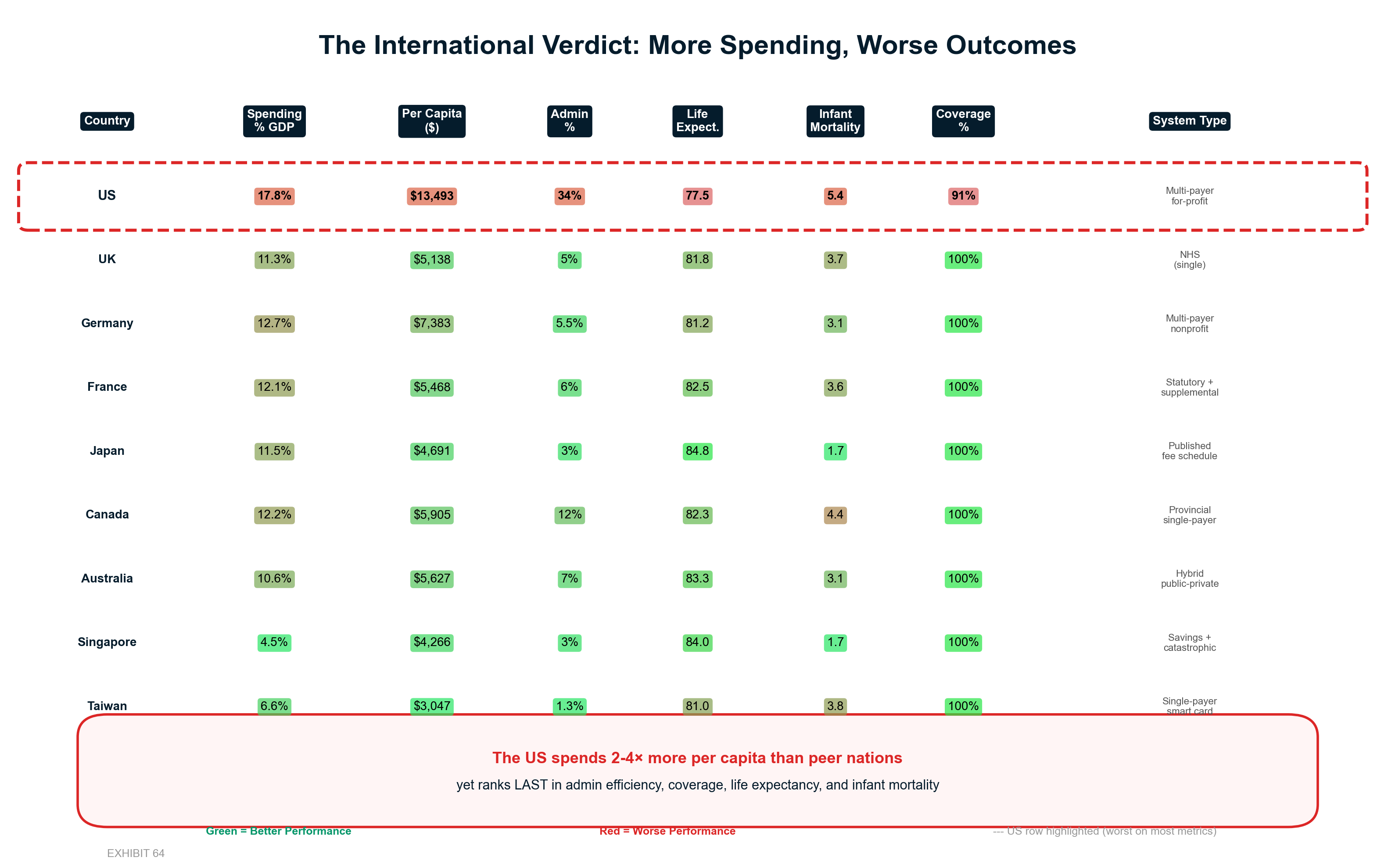
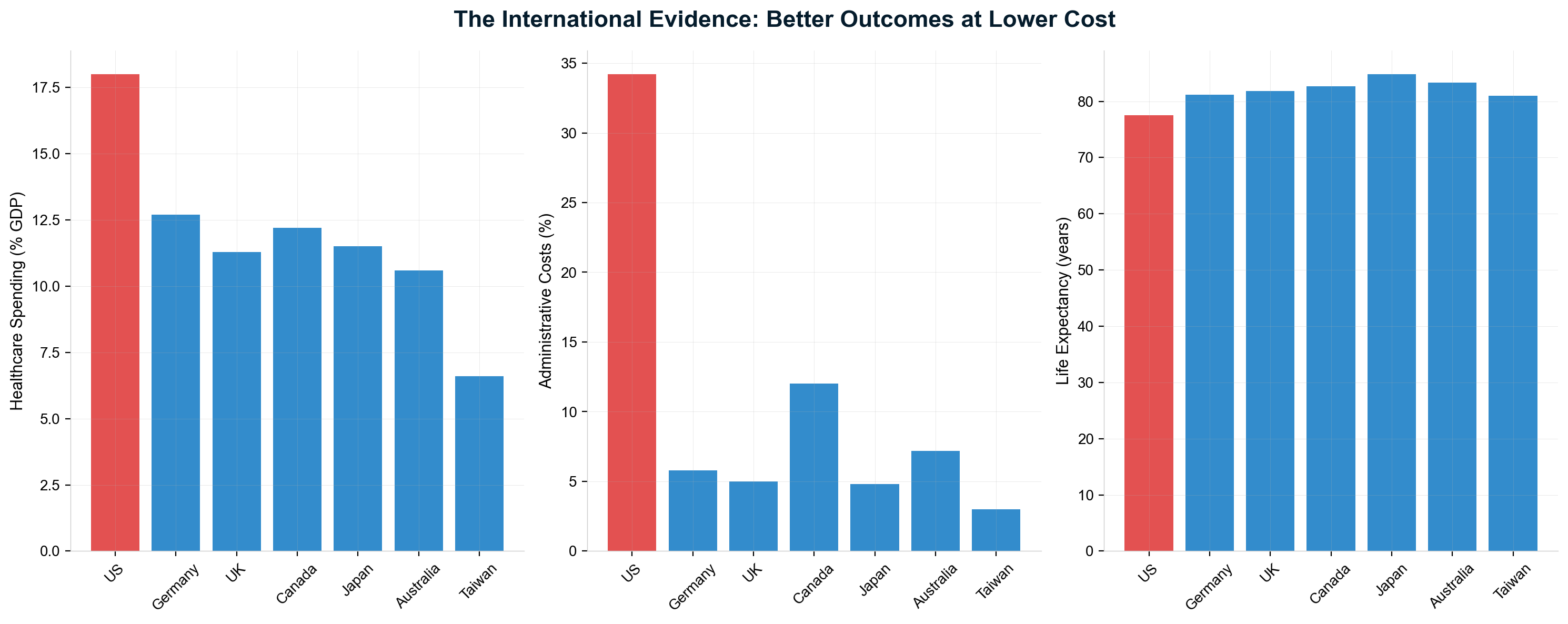
Singapore: The Rational Model for Scope Separation
Singapore's healthcare system represents the most explicit separation of routine and catastrophic care financing, demonstrating how rational design eliminates insurance intermediaries from routine healthcare while maintaining universal coverage. The three-pillar system proves extraction is a design choice, not an inevitable feature of healthcare economics.
Medisave mandatory savings accounts funded by 7-9.5% of wages enable direct payment for routine care without insurance claims processing—creating effectively zero administrative overhead for predictable healthcare transactions. Patients pay providers directly from dedicated accounts, eliminating prior authorization bureaucracy, claims adjudication, and denial mechanisms that plague American healthcare. Total Medisave balances exceeding S$90 billion (18% of Singapore's GDP) demonstrate the system's sustainability and patient ownership.
MediShield Life provides universal catastrophic insurance covering large hospital bills and major procedures through low premiums targeting genuinely unpredictable, expensive events. High deductibles ensure coverage for true catastrophic care while eliminating 80% of insurance claims processing by excluding routine transactions. This design prevents insurance companies from extracting value from routine healthcare while maintaining protection against devastating medical expenses.
Medifund safety net assistance provides means-tested government support rather than universal subsidies, ensuring no one faces financial barriers to essential care while targeting resources efficiently. The three-pillar design creates incentives for cost-conscious healthcare consumption while maintaining universal access and catastrophic protection.
Results prove extraction-free healthcare's potential: Singapore achieves universal coverage at 4.5% of GDP with 84.3-year life expectancy versus America's 17.8% GDP spending and 77.5-year life expectancy. Administrative costs approach zero for routine care while remaining minimal for catastrophic coverage—demonstrating healthcare efficiency when extraction incentives are eliminated.
Taiwan: Single-Payer Designed From Scratch
Taiwan implemented National Health Insurance in 1995 after studying every existing healthcare system, creating optimized single-payer administration that achieves the world's lowest healthcare administrative costs while providing universal coverage. The system demonstrates rational healthcare design unencumbered by existing extraction infrastructure.
Smart card technology eliminated most paperwork and prior authorization by containing complete medical history and eligibility data, enabling real-time claims processing without bureaucratic intermediaries. Standardized billing and payment systems across all providers eliminate the administrative complexity that generates extraction opportunities in fragmented systems.
Administrative efficiency reaches 1.3% of total healthcare spending—the single lowest among universal systems—while achieving 99.9% population coverage with 95%+ public satisfaction rates. Global budgets combined with fee-for-service payments control costs while maintaining provider autonomy and patient choice.
The transition management proves comprehensive healthcare transformation remains politically and operationally feasible: Taiwan successfully moved from fragmented insurance schemes to single-payer without disrupting care delivery while guaranteeing benefit continuity. Implementation occurred within two years using existing administrative infrastructure adapted for universal coverage.
Canada: Provincial Single-Payer Federalism
Canada's Medicare system demonstrates gradual transition to single-payer through provincial implementation, providing a federal template for large countries with decentralized governance structures. The province-by-province rollout from 1966-1971 offers specific lessons for American state-based reform strategies.
Provincial single-payers for medically necessary services eliminate insurance underwriting, marketing, and profit extraction while maintaining care delivery through private providers. The Canada Health Act establishes national principles while allowing provincial administration flexibility, proving federalism compatible with single-payer efficiency when national standards prevent regulatory arbitrage.
Administrative costs of approximately 1.3% reflect single-payer efficiency despite provincial fragmentation—still representing one-third the administrative burden of American multi-payer systems. Elimination of insurance company profits, reduced billing complexity, and simplified payment systems generate substantial efficiency gains even within decentralized structures.
Canadian insurance companies adapted to Medicare by pivoting to supplemental coverage for non-covered services (dental, vision, pharmaceuticals, private rooms) rather than disappearing entirely. This transition model demonstrates insurance industry adaptation possibilities during American single-payer implementation, reducing political opposition through alternative business opportunities.
Germany: Multi-Payer Without Extraction
Germany's sickness fund system proves multiple payers need not create American-level extraction if properly structured through nonprofit status and heavy regulation. Approximately 87% of the population is covered by statutory health insurance (Gesetzliche Krankenversicherung, or GKV) administered through roughly 105 nonprofit "sickness funds" (Krankenkassen). The remaining ~13% — primarily civil servants, the self-employed, and high earners above €69,300/year (2024 threshold) — may opt for substitutive private health insurance (Private Krankenversicherung, or PKV). [185] [228] Critically, even Germany's private insurance sector operates under constraints bearing no resemblance to the American model: all-payer rate setting ensures hospitals and physicians receive standardized payments regardless of payer, and private insurers cannot deny coverage for pre-existing conditions when enrollees switch from statutory insurance. Administrative costs across the combined system total approximately 5-6% of health spending — roughly half the American rate. [24] The system demonstrates multi-payer efficiency when profit extraction and competitive gaming are eliminated through regulatory design.
The approximately 105 nonprofit sickness funds provide standardized benefits through income-based premiums (14.6% of wages split between employers and employees) with limited choice among funds focused on service quality rather than benefit manipulation. All-payer rate setting eliminates network negotiations and provider payment games that enable extraction in competitive insurance markets. Competition among sickness funds occurs on service quality and supplementary benefits, not on risk selection or price — the opposite of American insurance market dynamics.
Why German multi-payer works without extraction: nonprofit structure eliminates shareholder profit extraction, standardized benefits prevent selection gaming, regulated premiums limit price competition while maintaining service focus, and unified payment rates eliminate network manipulation. These design features prove the problem isn't multiple payers but for-profit payers with perverse incentives.
Administrative costs of 5-6% of total healthcare spending—half the American rate—demonstrate multi-payer efficiency potential when extraction incentives are eliminated through regulatory structure. Universal coverage with high patient satisfaction proves competitive insurance markets can function efficiently when properly designed for patient welfare rather than profit extraction.
United Kingdom: Direct Government Provision
The National Health Service represents the most comprehensive approach to eliminating healthcare extraction through government ownership of delivery infrastructure and direct employment of healthcare workers. The system demonstrates extraction elimination through structural integration rather than payment reform alone.
Government ownership of hospitals and employment of physicians creates direct accountability while eliminating insurance intermediaries for most care delivery. Funding through general taxation rather than premiums or payroll taxes simplifies administration while ensuring universal access regardless of employment status or ability to pay.
Administrative costs of approximately 5% include broader scope than other systems but remain dramatically lower than American levels through elimination of insurance claims processing, billing complexity, and profit extraction. Direct government payment eliminates most bureaucratic intermediation between patients and providers.
Trade-offs include wait times for some elective procedures due to political underfunding rather than inherent system inefficiency—demonstrating government healthcare's vulnerability to budget constraints while proving efficiency potential when adequately funded. Quality outcomes match or exceed American performance at 50% the per-capita cost.
Inventory of NHS Critiques
Any honest assessment must acknowledge the NHS's real weaknesses — frequently cited by opponents of American reform:
- Wait time crisis: As of 2024, approximately 7.6 million people were on NHS waiting lists, with 3.1 million waiting more than 18 weeks for treatment. Emergency department waits exceeding 12 hours became routine. [194]
- Chronic underfunding: A decade of austerity (2010-2020) reduced real per-capita spending growth to near zero. NHS spending at ~10.3% of GDP remains below the EU average of 11%.
- Workforce shortages: Approximately 150,000 staff vacancies including 12,000+ doctor and 47,000+ nursing positions.
- Capital infrastructure decay: Maintenance backlog exceeding £10 billion, with some hospital facilities literally crumbling.
- Growing private sector: Rising NHS wait times have driven growth in private healthcare, creating a two-tier system.
However, context is essential: The NHS delivers these outcomes at ~10.3% of GDP versus America's 18%, with universal coverage, no medical bankruptcies, no surprise billing, life expectancy 4+ years longer, and administrative costs of ~5% versus 15-34%. The NHS's problems are primarily problems of underfunding, not structural design. No peer nation has 27+ million uninsured, and no peer nation devotes 58% of healthcare spending to non-clinical extraction. [194]
Japan: Price Transparency and Standardization
Japan achieves administrative efficiency through radical price transparency rather than single-payer administration, demonstrating how published fee schedules eliminate extraction opportunities while maintaining insurance competition. The system proves transparent pricing can create functional healthcare markets.
Every medical procedure has a transparent, uniform price through published national fee schedules using a point-based system (1 point = 10 yen) updated biannually. This eliminates chargemaster gaming, network negotiations, and surprise billing while enabling informed patient choice and provider competition on quality rather than price manipulation.
Universal coverage through employment-based and community insurance schemes maintains choice while standardized pricing eliminates extraction opportunities through billing complexity. Administrative costs of approximately 3% result from simplified billing, minimal prior authorization, and standardized claims processing enabled by transparent pricing.
High healthcare utilization with controlled costs demonstrates price transparency's effectiveness: patients can access any provider without network restrictions while understanding exact costs in advance. The system proves administrative efficiency comes from standardization rather than necessarily requiring single-payer structure.
France: Regulated Two-Tier Efficiency
France's statutory plus supplemental system demonstrates how private insurance can function without extraction when properly regulated through nonprofit requirements, standardized benefits, and community rating. The model proves supplemental coverage compatibility with efficiency when extraction incentives are eliminated.
Statutory health insurance covers 70-80% of costs with regulated supplemental "mutuelle" insurance covering remaining expenses through heavily regulated, mostly nonprofit organizations. 99% of French residents maintain supplemental coverage through standardized benefit packages that prevent gaming and selection manipulation.
Administrative costs of approximately 6% despite two-tier complexity demonstrate regulatory effectiveness: supplemental insurers operate as nonprofit or mutual organizations with community rating requirements and price regulation that prevents extraction while maintaining coverage comprehensiveness.
The system proves public-private partnership viability when private insurance is structured for patient welfare rather than profit extraction—offering lessons for American reform that preserves some private insurance role while eliminating extraction mechanisms.
Australia: Public Option as Market Anchor
Australia's hybrid system demonstrates how robust public options can anchor mixed systems while preventing excessive private sector extraction through competitive pressure. Medicare provides universal public coverage while private insurance offers additional options without creating extraction opportunities.
Strong public option ensures private insurers cannot hold patients hostage while government pharmaceutical price negotiation eliminates drug pricing games through monopsony purchasing power. Community rating for private insurance limits risk-based pricing while lifetime health cover loadings encourage early enrollment without penalties.
Administrative costs of approximately 7% reflect mixed system complexity while remaining dramatically lower than American levels through public option competitive pressure on private insurance efficiency. Universal public coverage eliminates uninsurance while private options provide choice without extraction.
The system demonstrates hybrid public-private viability when public options are robust and government maintains pricing authority over pharmaceuticals—proving mixed systems can function efficiently with proper competitive structure and regulatory oversight.
The Scope Inflation Lesson: America's Unique Error
Comparative analysis reveals the fundamental error in American healthcare design: processing routine healthcare through insurance intermediaries designed for catastrophic risk pooling. International evidence proves this intermediation layer is unnecessary, costly, and purely extractive.
Key Pattern Recognition:
- Singapore explicitly separates routine care (savings accounts) from catastrophic care (insurance)
- Japan's fee schedules eliminate need for complex negotiations and prior authorizations
- UK/Canada systems use government payment directly—no claims processing for most care
- Taiwan's smart cards reduce routine transactions to near-zero administrative cost
- Germany's standardization eliminates administrative games plaguing US multi-payer systems
The United States remains unique in running $4 generic prescriptions and routine office visits through multi-party claims adjudication systems that other countries prove unnecessary. International experience demonstrates routine healthcare requires payment mechanisms, not insurance mechanisms, while catastrophic care requires risk pooling without extraction incentives.
Immediate Adoption Opportunities for America
Based on international evidence, reforms ranked by political feasibility and administrative savings potential:
Price Transparency (Japan Model): Require published, uniform fee schedules for common procedures. Estimated savings: 15-20% reduction in administrative costs through elimination of negotiation overhead and billing complexity.
Nonprofit Insurance Conversion (Germany Model): Convert health insurers to nonprofit status or implement German-style regulation of for-profit insurers. Estimated savings: 10-15% reduction through elimination of profit extraction and competitive gaming.
Routine Care Savings Accounts (Singapore Model): Expand health savings accounts to cover all routine care with mandatory employer/employee funding while maintaining insurance for catastrophic care only. Estimated savings: 25-30% reduction by eliminating insurance processing for routine transactions.
Smart Card Technology (Taiwan Model): Implement unified electronic health records and real-time billing systems to eliminate paperwork and prior authorization for routine care. Estimated savings: 10-15% reduction in administrative processing costs.
Public Option Implementation (Australian Model): Create government-run insurance option competing with private plans while maintaining robust coverage as market anchor. Estimated savings: 20-25% reduction through competitive pressure and standardization.
Provincial Single-Payer (Canadian Model): Enable state-by-state transition to single-payer systems with federal coordination and standards. Estimated savings: 60-70% reduction in administrative costs for participating states.
The Path Forward: Learning from Global Success
International experience demonstrates healthcare extraction is not inevitable—it represents policy choices that other countries avoided through rational system design. Every developed nation except the United States provides universal coverage with administrative costs under 8% of total spending, with most achieving costs under 6%.
The lesson is unambiguous: insurance intermediation for routine healthcare is unnecessary, costly, and extractive. Whether through savings accounts, price transparency, government payment, or nonprofit regulation, successful healthcare systems eliminate financial intermediaries from routine healthcare transactions while maintaining or improving access and outcomes.
The United States can adopt proven international practices immediately rather than continuing failed experiments with extraction-based healthcare financing. The choice belongs to American policymakers: continue subsidizing the world's most expensive healthcare system while tolerating preventable suffering, or join peer countries in providing healthcare as a public good rather than an extraction opportunity.
Healthcare transformation requires abandoning American exceptionalism in favor of evidence-based policy learning from international success. The models exist, the results are proven, and the benefits are clear. Only political will and organized opposition to extraction-based healthcare prevent American adoption of systems that work effectively throughout the developed world.
Chapter 18: Policy Recommendations — Dismantling the Machine
Ending healthcare extraction requires systematic intervention across four strategic tiers: structural reforms that eliminate extraction incentives, market corrections that restore competition, administrative simplifications that reduce waste, and transparency requirements that enable accountability. These evidence-based recommendations target root causes of dysfunction rather than symptoms, drawing from successful international models and American policy innovations that have demonstrably reduced extraction while improving access and outcomes.
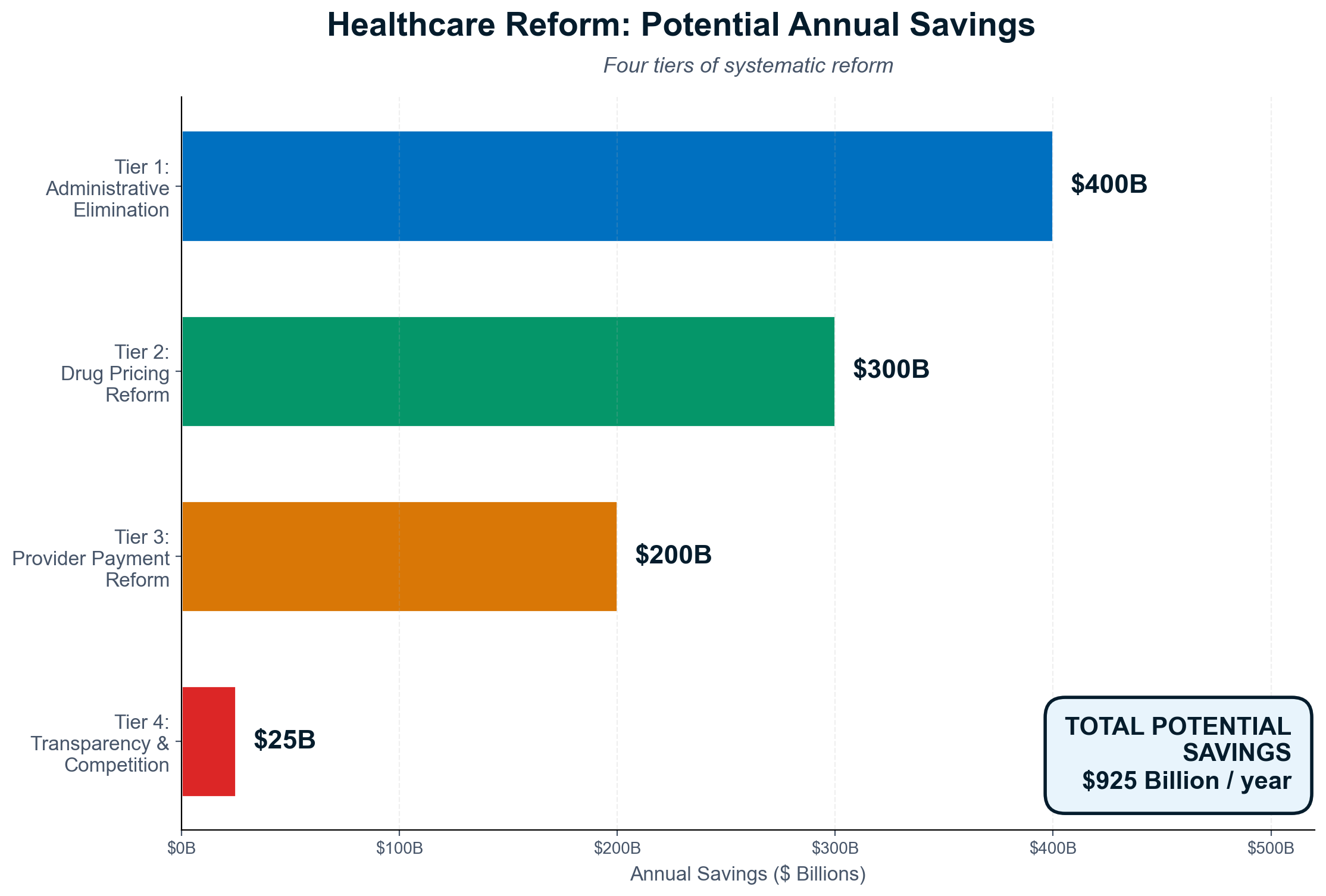
Tier 1: Structural Transformation (Maximum Impact, Highest Feasibility Requirements)
Single-Payer Healthcare System
Estimated Annual Savings: $450-500 billion
Feasibility Score: 3/10
Medicare for All represents comprehensive extraction elimination through replacement of 1,644 private insurance companies with unified government administration achieving 2-3% administrative costs versus current 15-20% private insurance overhead. Canada's implementation from 1966-1971 provides federal transition precedent, while Taiwan's 1995 "big bang" approach demonstrates rapid transformation feasibility.
Implementation mechanisms include expanding Medicare eligibility to all Americans while maintaining private healthcare delivery. Current Medicare infrastructure could process universal enrollment within 24 months using existing systems and procedures. Financing would replace insurance premiums, deductibles, and copays with progressive taxation reducing costs for 95% of families while eliminating medical bankruptcy and debt.
The political challenge involves overcoming $650 million in annual industry opposition spending while building coalitions among healthcare workers (79% of nurses support Medicare for All), patients (69% public support), and progressive employers who would benefit from healthcare cost elimination. Transition support for displaced insurance workers requires $200+ billion over five years but generates 3:1 return on investment through administrative savings.
Public Option Alternative
Estimated Annual Savings: $200-300 billion
Feasibility Score: 6/10
Government-administered insurance competing with private plans would capture 40-60% of single-payer savings through competitive pressure while preserving choice and enabling gradual transition. The public option would operate like Medicare with transparent pricing, standardized benefits, and simplified administration providing 3-5% administrative costs versus 15-20% private insurance overhead.
State-level implementation through Medicare buy-in options allows demonstration of public option effectiveness while building political support for national expansion. Premium subsidies ensure affordability while private insurance competition maintains consumer choice during transition periods.
Competitive advantages include elimination of insurance company profits (15-20% of premium revenue), negotiating power reducing provider costs, and simplified administration eliminating bureaucratic complexity. Private insurers would face pressure to reduce overhead and improve efficiency to compete with public option pricing and simplicity.
The Adverse Selection Trap: Why Public Options Fail Without Universal Enrollment
Any public option competing alongside private insurance faces a fundamental mathematical problem. Without mandatory participation, the public option becomes the insurer of last resort for the sickest patients while private insurers retain profitable healthy enrollees. The death spiral operates predictably: premiums rise → healthy enrollees leave → costs concentrate → premiums rise further → the public option is labeled "failing." This is exactly what happened in early ACA marketplace exchanges before stabilization mechanisms. [197]
The economic literature is unambiguous: "private information about risk always produces under-insurance relative to the efficient outcome, and mandatory insurance coverage is always a welfare-improving policy intervention." [197] Any viable public option must include either: (a) an individual mandate with meaningful penalties, (b) default auto-enrollment with private opt-out, or (c) universal coverage with no opt-out (single-payer). Options that allow free-riding will fail mathematically as private insurers systematically cream-skim profitable enrollees.
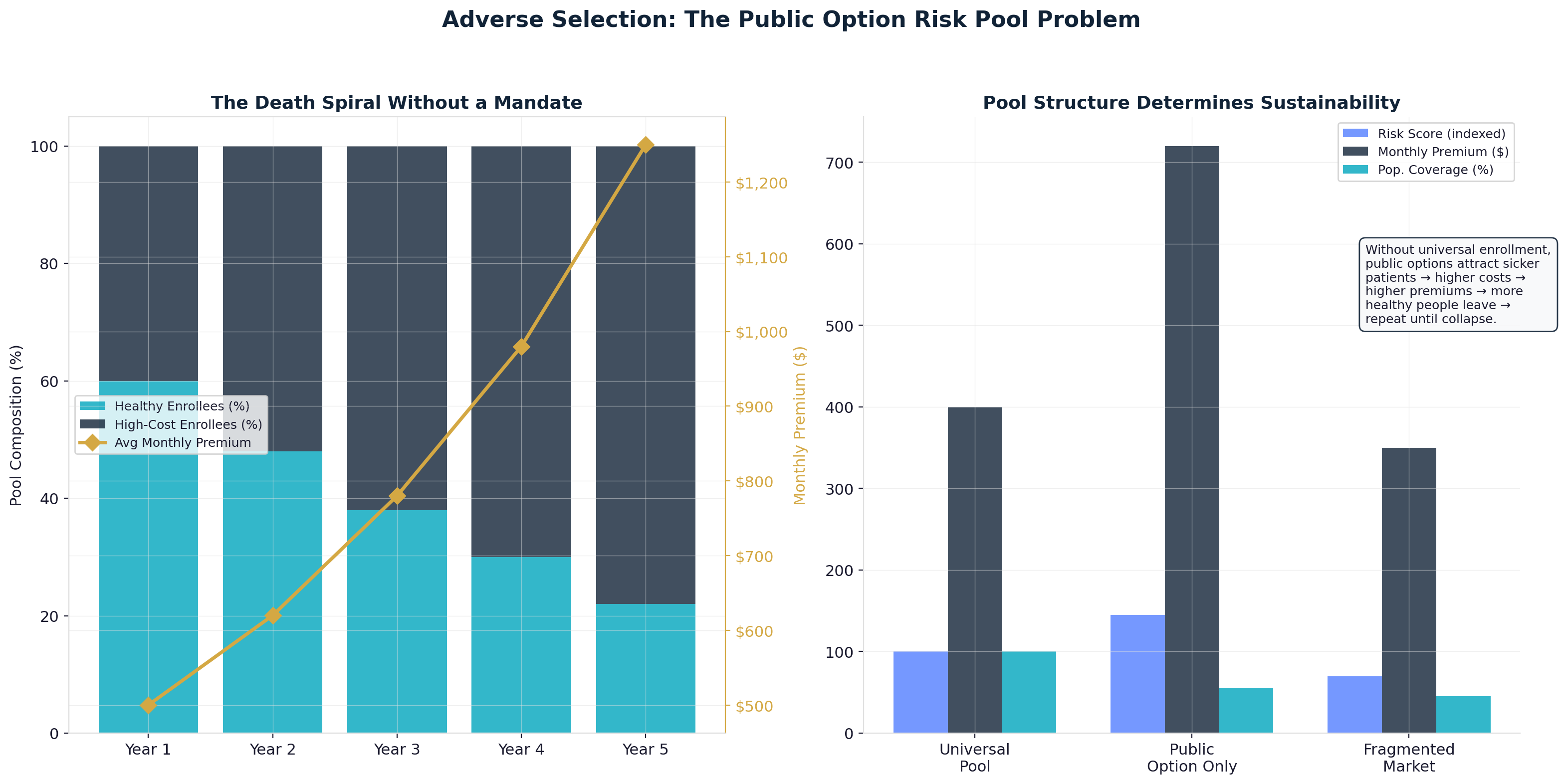
All-Payer Rate Setting
Estimated Annual Savings: $150-200 billion
Feasibility Score: 5/10
Uniform payment rates for medical services regardless of insurance type would eliminate price discrimination enabling extraction. Maryland's all-payer system demonstrates feasibility while achieving cost control and quality improvement through hospital global budgets and standardized pricing.
Independent rate-setting boards would establish payment schedules using Medicare rates as baselines with geographic cost adjustments. All insurers including private companies would pay identical rates for identical services, eliminating facility fees, surprise billing, and price manipulation that enable systematic overcharging.
Benefits include complete surprise billing prevention (all providers accept standard rates), price transparency through published fee schedules, and competition focused on quality and service rather than billing optimization. Implementation requires federal legislation overriding ERISA preemption while enabling state-level rate setting authority.
Tier 2: Market Structure Corrections (High Impact, Moderate Feasibility)
Comprehensive PBM Reform
Estimated Annual Savings: $40-80 billion
Feasibility Score: 7/10
Pharmacy Benefit Manager regulation would eliminate spread pricing, mandate rebate transparency, and prohibit vertical integration conflicts of interest that enable systematic pharmaceutical overcharging. The FTC's finding that Big 3 PBMs generated $1.4 billion from spread pricing on specialty generics alone demonstrates extraction scope.
Regulatory mechanisms include mandatory rebate pass-through (100% to plan sponsors), spread pricing prohibition, and ownership conflict elimination preventing PBMs from owning pharmacies or pharmaceutical companies. Real-time transaction reporting and standardized fee structures would enable oversight while independent auditing ensures compliance.
Federal preemption would override state laws enabling PBM exploitation while empowering state insurance commissioners to revoke licenses for violations. The reform enjoys bipartisan support due to clear evidence of abuse and documented patient harm from pharmaceutical access barriers.
Hospital System Antitrust Enforcement
Estimated Annual Savings: $75-125 billion
Feasibility Score: 8/10
Aggressive merger enforcement would restore healthcare market competition through retrospective review authority, lowered concentration thresholds, and prospective blocking of harmful consolidation. Current HHI levels exceeding 2,500 in most healthcare markets indicate monopolistic concentration requiring immediate intervention.
Enforcement mechanisms include retroactive merger challenges for deals completed within the past decade, structural separation requirements for vertically integrated companies, and behavioral remedies preventing anti-competitive practices. Hospital systems exceeding 40% market share would face divestiture requirements similar to telecommunications antitrust precedents.
Specific targets include UnitedHealth Group's vertical integration creating conflicts of interest, regional hospital monopolies extracting pricing premiums, and pharmaceutical mergers reducing development competition. Existing legal authority requires execution rather than new legislation, making implementation immediately feasible.
Medicare Drug Price Negotiation Expansion
Estimated Annual Savings: $100-150 billion
Feasibility Score: 6/10
Expanding Inflation Reduction Act authority from 60 medications to comprehensive coverage would reduce pharmaceutical costs through monopsony purchasing power. The VA's 40-50% lower drug costs compared to Medicare Part D demonstrates negotiation potential when implemented systematically.
Implementation would include all Medicare Part D drugs rather than limiting negotiations to high-spend thresholds, international reference pricing tying costs to peer country averages, and patent reform preventing evergreening tactics that extend monopolies artificially. Manufacturers refusing negotiation would lose Medicare and Medicaid access.
Supporting reforms include generic drug importation from approved sources, government pharmaceutical manufacturing capability for essential medications, and march-in rights enabling federal production of drugs developed with taxpayer funding when private companies charge excessive prices.
Tier 3: Administrative Simplification (Moderate Impact, High Feasibility)
Standardized Billing Systems
Estimated Annual Savings: $100-150 billion
Feasibility Score: 8/10
Administrative standardization would reduce healthcare billing complexity to international efficiency levels while maintaining private insurance options. Single national claim forms, uniform prior authorization procedures, and simplified coding systems would eliminate 40-60% of current administrative overhead.
Federal regulation under existing HIPAA authority would require all insurers to use standardized processes, with non-compliant companies losing ability to participate in government programs including Medicare Advantage and marketplace plans. Electronic prior authorization with automated approval for routine services would maintain utilization management while reducing administrative burden.
Germany's standardization achieving 5-6% administrative costs demonstrates multi-payer efficiency potential when bureaucratic gaming is eliminated through regulatory requirements. Taiwan's smart card system proves technology can reduce routine healthcare transactions to near-zero administrative costs.
Prior Authorization Reform
Estimated Annual Savings: $40-60 billion
Feasibility Score: 9/10
Systematic prior authorization reform would eliminate administrative barriers to necessary care while maintaining appropriate utilization management. "Gold card" programs exempting physicians with low denial rates, automated approval for routine services, and 24-hour maximum decision timeframes would reduce bureaucratic obstruction.
Financial penalties would include doubling reimbursement for overturned denials, covering patient costs for delayed care, and paying legal fees for successful appeals. With 80% of denials overturned on appeal, automatic penalties for pattern denials would eliminate systematic gaming while protecting legitimate utilization management.
State-level implementation in Louisiana, Texas, and California demonstrates feasibility and effectiveness: electronic processing reduced turnaround times 60% while gold-carding programs reduced prior authorization volume 40% without compromising medical appropriateness.
Administrative Cost Caps
Estimated Annual Savings: $75-100 billion
Feasibility Score: 6/10
Healthcare administrative spending limits tied to international benchmarks would force efficiency improvements while maintaining service quality. Administrative costs exceeding 6% of total spending (double the German benchmark) would trigger regulatory intervention and corrective action requirements.
Medical Loss Ratio expansion to all healthcare entities would require minimum percentages of revenue flowing to patient care rather than administrative overhead. Organizations exceeding administrative cost thresholds would face financial penalties and operational oversight until efficiency improvements are demonstrated.
International benchmarks prove 6% administrative cost targets remain achievable: Germany (5-6%), Taiwan (1.3%), Japan (3%), and Australia (7%) all demonstrate efficient administration while maintaining quality care and provider autonomy.
Tier 4: Transparency and Accountability (Foundation for All Reform)
Comprehensive Price Transparency
Estimated Annual Savings: $20-30 billion
Feasibility Score: 9/10
Enhanced price transparency enforcement would replace current trivial penalties with meaningful consequences for non-compliance. Hospital price transparency fines of $1 million monthly for large hospitals would ensure compliance, while market access penalties including Medicare exclusion would eliminate economic incentives for opacity.
Real-time transparency requirements would include digital price displays for common services, standardized formats enabling comparison shopping, and insurance plan cost-sharing calculators providing patients with actual out-of-pocket estimates before service delivery.
Japan's published national fee schedule demonstrates complete price transparency compatibility with high-quality care and patient satisfaction. Price transparency enables consumer choice and competitive pressure while exposing extraction mechanisms that rely on information asymmetry.
Healthcare Financial Disclosure
Estimated Annual Savings: $15-25 billion
Feasibility Score: 8/10
Mandatory financial reporting would require real-time disclosure of costs, profits, executive compensation, and pricing for all healthcare entities receiving public funds. Private equity firms would report management fees, operational changes, and financial performance at healthcare portfolio companies.
Public databases would enable comparison shopping, accountability journalism, and regulatory oversight while SEC investigation authority would ensure healthcare company financial reporting accuracy. Quarterly reporting requirements would prevent accounting manipulation while enabling market-based accountability.
Executive compensation disclosure tied to patient outcomes rather than financial extraction would realign incentive structures through public transparency and regulatory oversight of compensation packages at organizations receiving taxpayer funding.
Implementation Strategy: Sequenced Reform for Political Success
Phase 1 (Years 1-2): Foundation and Quick Wins
Priority reforms include price transparency enforcement, prior authorization simplification, and PBM regulation—changes achievable through existing regulatory authority while building public support for comprehensive transformation. These foundational changes would demonstrate reform effectiveness while reducing costs and improving access immediately.
Phase 2 (Years 3-5): Market Structure Reform
Hospital merger enforcement, drug price negotiation expansion, and administrative standardization would restore competitive markets while building toward structural changes. Political momentum from early successes enables more comprehensive interventions requiring legislative action.
Phase 3 (Years 5-10): Structural Transformation
Public option implementation, all-payer rate setting, or single-payer transition would complete healthcare system transformation based on demonstrated effectiveness of earlier reforms. International evidence and domestic pilot programs would inform optimal implementation strategies for universal coverage.
The cumulative savings potential ranges from $850 billion to $1.6 trillion annually—sufficient to provide universal coverage, eliminate medical debt, and improve health outcomes while reducing overall spending. Political feasibility requires sustained organizing, business community education about cost savings, and public awareness campaigns exposing extraction mechanisms currently operating below public visibility.
Reform Opposition and Counter-Strategies
Healthcare industry opposition spending of $650+ million annually will deploy "disruption" messaging despite minimal impact on care delivery, "innovation" arguments ignoring evidence that most pharmaceutical research occurs in universities, and "choice" rhetoric while current systems restrict provider networks and coverage options.
Counter-strategies include building coalitions among healthcare workers experiencing administrative burden, employers facing healthcare cost pressures, and patients suffering from extraction mechanisms. International evidence provides powerful counter-narratives to industry opposition arguments while demonstrated savings potential attracts business community support.
The policy roadmap exists with proven international precedents and documented domestic pilot successes. The question remains whether political leadership will emerge to implement evidence-based reforms that prioritize patient welfare over extraction industry profits while building American healthcare systems that actually serve human health rather than wealth accumulation.
Chapter 19: The Path Forward — What Universal Care Could Look Like
Universal healthcare represents not just policy reform but economic transformation that would redirect $1+ trillion annually from extraction to care delivery while eliminating medical bankruptcy, improving health outcomes, and enhancing American economic competitiveness. Three concrete models—national Medicare for All, California's CalCare, and New York's Health Act—demonstrate specific pathways for achieving universal coverage with documented savings, implementation strategies, and transition plans addressing workforce displacement concerns.
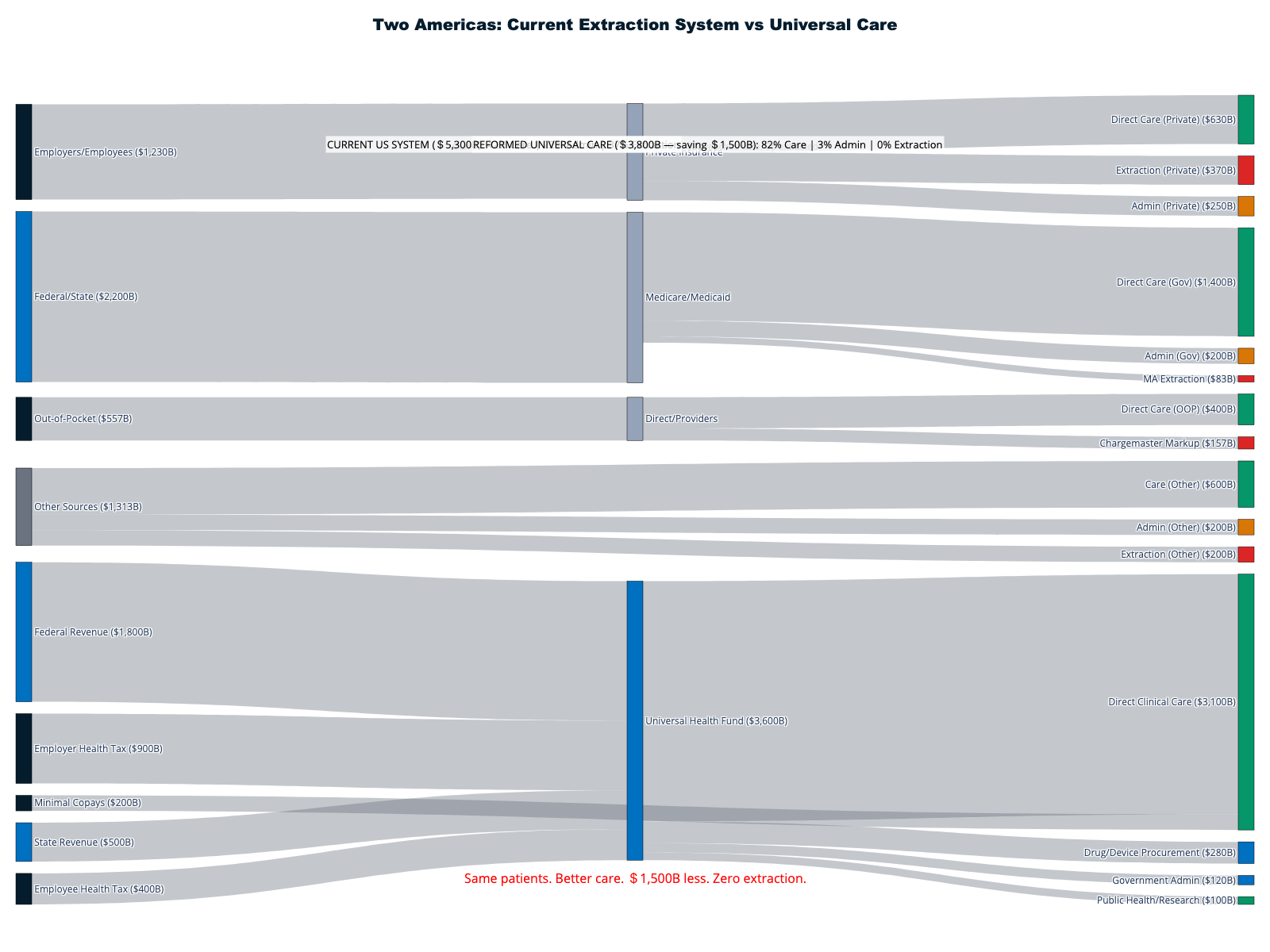
National Model: Medicare for All — $1.5 Trillion Annual Transformation
Medicare for All would replace the fragmented American healthcare system with unified administration serving all 335 million Americans through expanded Medicare infrastructure. The transformation would eliminate insurance industry extraction while maintaining private healthcare delivery, enabling universal coverage at lower total cost than current system dysfunction.
Financial Architecture and Savings
Total system cost projections range from $3.5-3.8 trillion annually versus current $5.3 trillion spending, representing net savings of $1.5-1.8 trillion through administrative efficiency, pharmaceutical negotiation, and elimination of insurance company profits. The savings exceed most countries' total healthcare spending while enabling universal access and comprehensive benefits.
Administrative savings of $400-500 billion annually would result from replacing 1,644 insurance companies with 2-3% Medicare overhead versus current 15-20% private insurance administration. Elimination of prior authorization bureaucracy, claims adjudication complexity, and network restrictions would enable physicians to focus on care delivery rather than billing optimization and utilization management.
Pharmaceutical savings of $150-200 billion annually through Medicare negotiation authority would reduce medication costs to international levels while maintaining innovation incentives. Government purchasing power combined with international reference pricing would eliminate the pharmaceutical rebate schemes that incentivize list price inflation while restricting patient access through formulary manipulation.
Implementation and Transition Strategy
The transition would occur through gradual Medicare expansion lowering eligibility age by five years every two years, enabling systematic infrastructure scaling while reducing political disruption. Year 1-2 would lower Medicare age to 60, Years 3-4 to 55, Years 5-6 to 50, continuing until universal coverage achievement by Year 10-12.
Existing Medicare infrastructure could process universal enrollment using established systems, procedures, and provider networks. The transition preserves all healthcare delivery while eliminating extraction layers: hospitals, clinics, physicians, and medical facilities continue operating under simplified payment systems without bureaucratic intermediation.
Provider payment would utilize Medicare fee schedules as baselines with geographic cost adjustments, ensuring adequate compensation while eliminating billing complexity. Global budgets for hospitals combined with simplified billing would reduce administrative costs while enabling predictable revenue streams for operational planning.
Economic Impact and Workforce Transition
Individual financial impact analysis shows 95% of American families would pay less for healthcare through progressive taxation replacing insurance premiums, deductibles, and copays. Average family savings of $3,000-5,000 annually would result from elimination of premium contributions, out-of-pocket costs, and medical debt while providing comprehensive coverage.
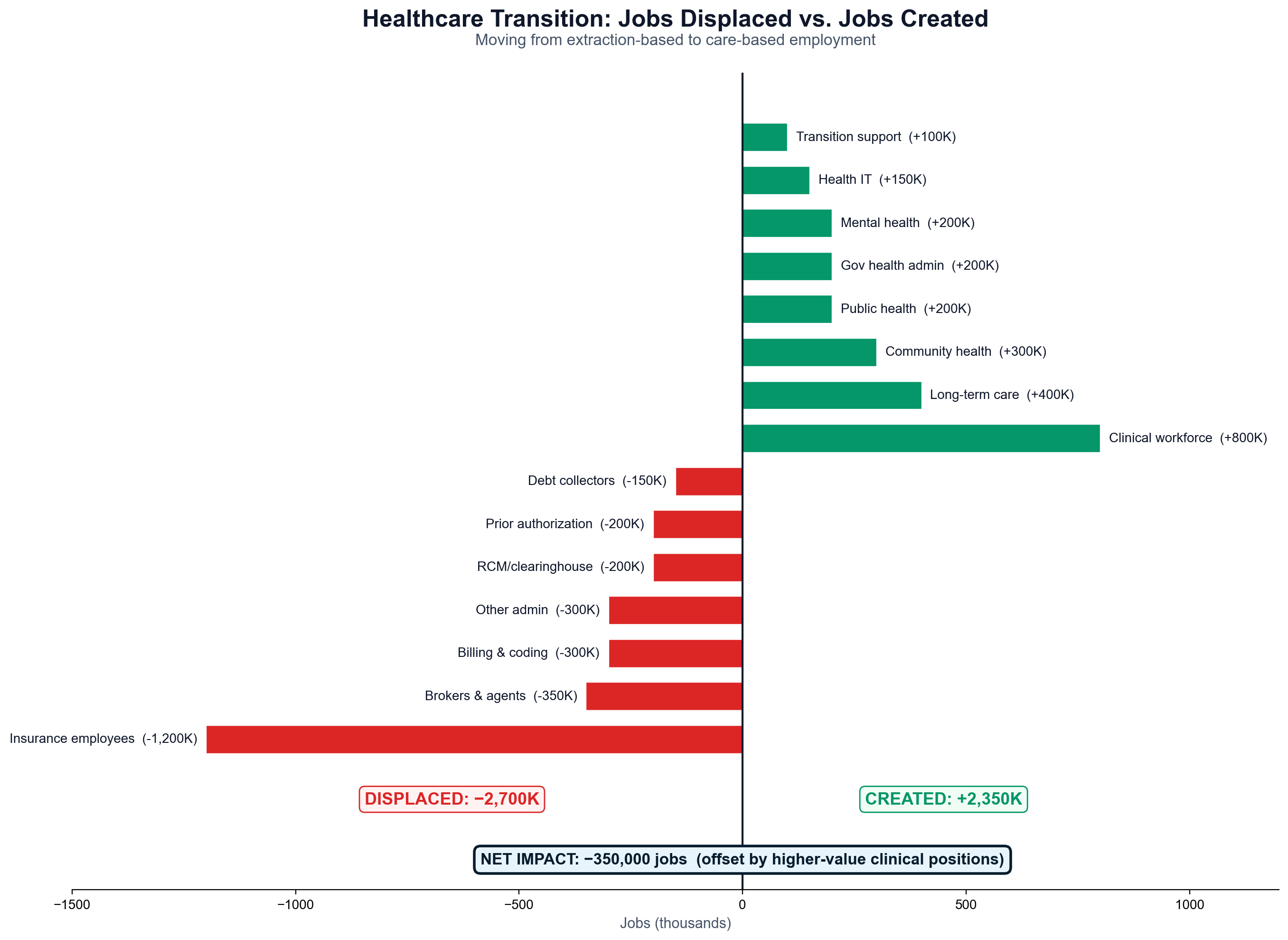
Employer impact would eliminate average health insurance costs of $15,797 per employee annually, replacing them with payroll tax contributions averaging 60-70% of current spending. American businesses would gain competitive advantages in global markets through healthcare cost elimination while workers enjoy complete job mobility without insurance restrictions.
The transition fund of $275 billion over five years would provide displaced workers with income replacement, retraining opportunities, and early retirement options while funding economic development in insurance industry-dependent communities. Historical precedents from Canada's Medicare implementation and Taiwan's National Health Insurance demonstrate successful workforce transitions.
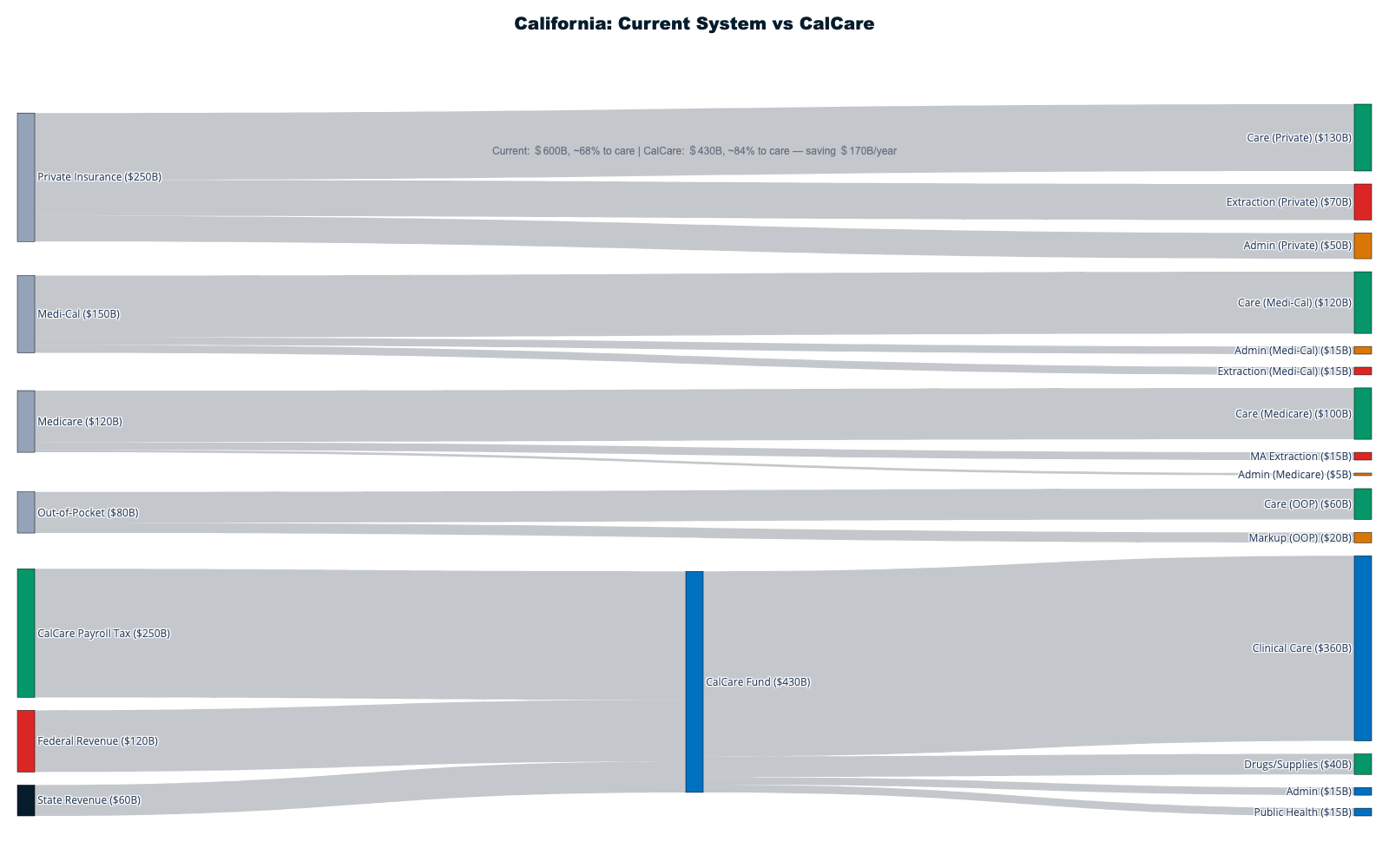
California Model: CalCare — State-Level Universal Coverage
California's CalCare proposal would create America's first state-level single-payer system covering 39 million residents, demonstrating universal healthcare feasibility while building momentum for national reform. The comprehensive analysis by Assembly appropriations staff provides detailed financial modeling and implementation strategy for the world's fifth-largest economy.
System Design and Coverage
Universal coverage for all California residents regardless of employment status, immigration status, or ability to pay would eliminate medical debt, insurance networks, and coverage gaps while providing comprehensive benefits including medical care, dental services, vision care, mental health treatment, and long-term care support.
Current California healthcare spending of approximately $600 billion annually would be replaced by CalCare costs projected at $314-391 billion, representing savings of $200-300 billion through administrative efficiency and elimination of insurance company profits. The savings exceed California's total general fund budget while enabling universal coverage expansion.
Benefits would include elimination of deductibles, copays, and out-of-pocket costs for covered services while providing broader coverage than current insurance options. Prescription drug benefits through California negotiation authority would reduce medication costs below current levels while ensuring access regardless of insurance formulary restrictions.
Funding Mechanism and Economic Impact
Constitutional amendment ACA 11 proposes progressive funding through payroll taxes on employers and employees, income tax surcharges on high earners, and gross receipts taxes on businesses exceeding $2 million revenue. Total revenue of $163 billion annually would fund basic system operations with federal waiver redirections covering remaining costs.
Large employers currently providing health insurance would typically pay less in payroll taxes than current premium contributions, while small employers not providing coverage would face new tax obligations offset by employee productivity gains and reduced turnover from healthcare access security.
Economic modeling shows 85% of California families would pay less for healthcare under CalCare compared to current insurance premiums, deductibles, and out-of-pocket costs. Business competitiveness would improve through elimination of healthcare costs as factor in location and expansion decisions.
Federal Waiver Strategy and Implementation Timeline
Section 1332 ACA waivers would enable California to redirect federal Medicare and Medicaid spending toward CalCare while maintaining federal requirements for coverage, affordability, and comprehensiveness. Technical analysis demonstrates federal savings through reduced administrative complexity and improved population health outcomes.
Implementation timeline includes Years 1-2 for system design and federal waiver negotiations, Year 3 for pilot launches in willing counties, and Years 4-5 for statewide implementation. The gradual rollout would enable infrastructure development while demonstrating system effectiveness for national replication.
Provider engagement strategy includes early stakeholder involvement, simplified billing systems, and guaranteed payment security attracting provider participation. The elimination of prior authorization, network restrictions, and claims denials would improve provider satisfaction while reducing administrative burden.
New York Model: Comprehensive Coverage for 19.5 Million
The New York Health Act would establish single-payer coverage for all state residents through comprehensive benefits and progressive financing, building on RAND Corporation economic analysis providing detailed cost projections and implementation roadmaps for America's fourth-largest state economy.
RAND Economic Analysis and Projections
Independent analysis projects New York Health system costs similar to current spending initially, with 3% annual savings by 2031 representing $15 billion annually through administrative efficiency improvements. Ten-year cumulative savings of 2% of total healthcare spending would grow over time as system optimization occurs.
Administrative savings of $15 billion annually by 2031 would result from reduced insurance company overhead, simplified provider billing systems, and elimination of prior authorization bureaucracy. The savings equal New York City's entire annual budget while enabling universal coverage without current insurance complexity.
Individual financial impact analysis shows 69% of New Yorkers would pay less for healthcare under progressive taxation replacing insurance premiums and out-of-pocket costs, while 31% would pay more through higher taxes offset by elimination of premium contributions and deductible burdens.
Healthcare Workforce and Economic Transition
New York's concentration of healthcare employment—including 280,000+ workers at major health systems like NewYork-Presbyterian, Northwell, and NYU Langone—requires comprehensive transition planning addressing insurance industry displacement while expanding care delivery capacity.
Insurance industry employment of approximately 45,000 direct jobs in New York would require transition support including retraining programs, government healthcare administration expansion, and alternative employment in healthcare technology and data analytics growing sectors.
Economic development strategy would include federal transition funding, alternative industry development, and healthcare infrastructure expansion supporting displaced workers while building system capacity for universal coverage implementation.
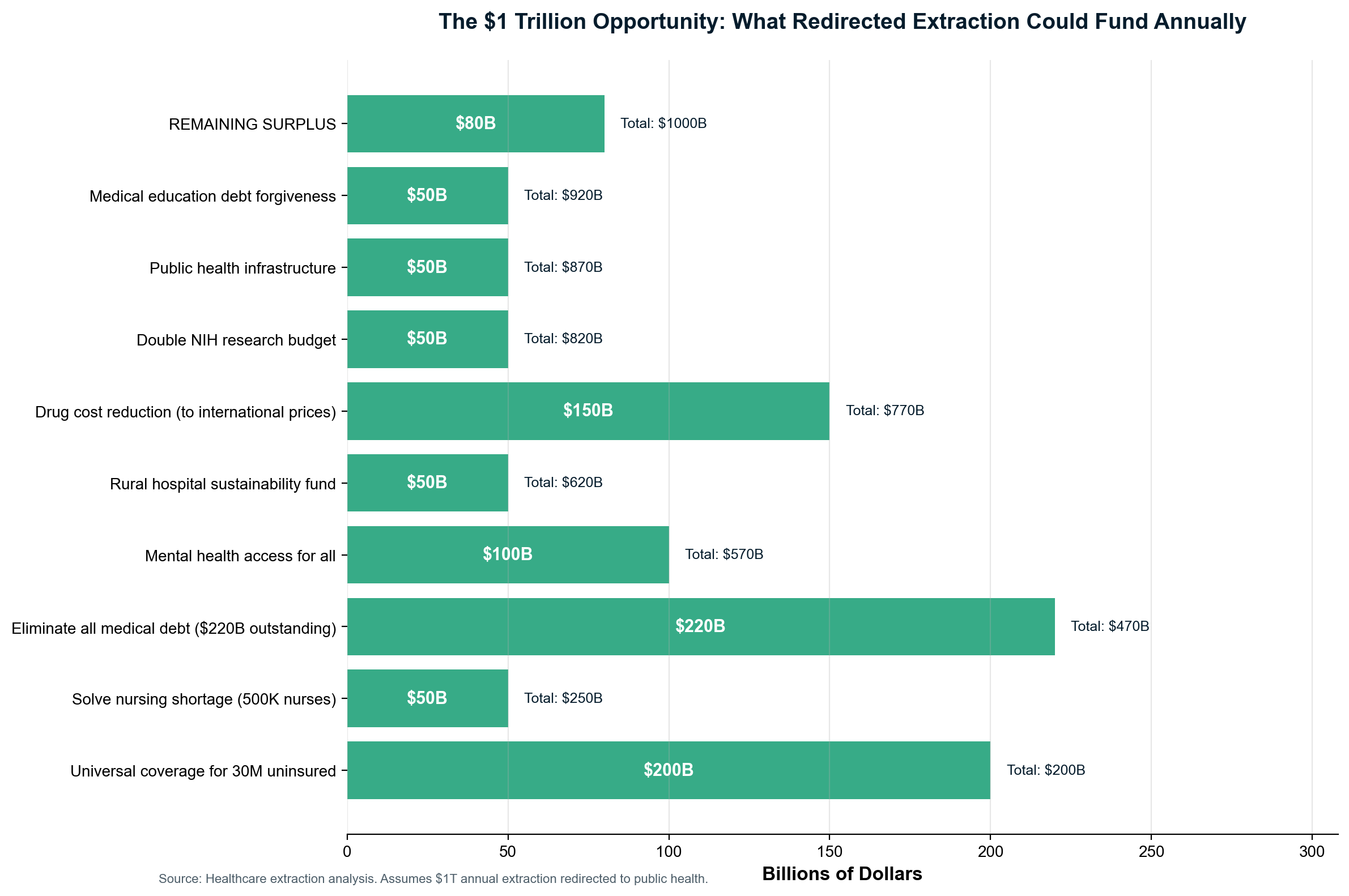
Positive Economics: Beyond Cost Control
Universal healthcare generates positive economic impacts extending far beyond cost savings through elimination of job lock, medical bankruptcy prevention, and business competitiveness enhancement. The economic transformation would enable entrepreneurship, labor mobility, and innovation while reducing productivity losses from delayed care and financial stress.
Elimination of Job Lock and Business Formation
Healthcare job lock affects an estimated 20-25 million Americans who remain in unsuitable employment solely for health insurance coverage, constraining labor market efficiency and entrepreneurial activity. Universal healthcare would enable optimal job matching while supporting business formation through healthcare cost elimination.
Small business competitiveness would improve dramatically through elimination of healthcare costs averaging $6,000-8,000 per employee annually for businesses currently providing coverage. Startups and independent contractors would gain access to comprehensive healthcare without employment-based coverage requirements.
The "gig economy" would expand through healthcare security enabling independent work without insurance coverage concerns. Creative industries, consulting services, and small business formation would accelerate when healthcare access no longer requires traditional employment relationships.
Medical Debt and Bankruptcy Elimination
Universal coverage would eliminate the 530,000 annual medical bankruptcies while providing debt relief for $220 billion in existing medical debt affecting 100+ million Americans. The economic stimulus from debt elimination would generate multiplier effects through increased consumer spending and reduced financial stress.
Credit improvements for Americans currently damaged by medical debt would enable home ownership, business formation, and education financing while reducing poverty rates and improving social mobility. Medical debt elimination represents one of the largest potential economic stimulus programs available through policy reform.
Healthcare access security would reduce emergency department utilization for routine care while enabling preventive treatment that reduces expensive crisis interventions. Population health improvements would generate productivity gains while reducing disability rates and healthcare utilization overall.
International Precedents for Successful Transitions
Canada's Provincial Implementation (1966-1971)
Canada's gradual province-by-province Medicare implementation provides direct precedent for American state-based transitions, demonstrating political and operational feasibility while building public support through visible success in early adopting regions.
Saskatchewan and British Columbia achieved universal coverage first, followed by Ontario despite initial opposition, with remaining provinces joining after observing positive results. The transition eliminated insurance company extraction while maintaining care delivery through existing providers and facilities.
Opposition from medical associations and insurance companies diminished as systems proved popular and effective, providing political lessons for American implementation strategy. Public support grew rapidly once universal coverage demonstrated tangible benefits for patients and providers.
Taiwan's Comprehensive Transformation (1995)
Taiwan's overnight transition from 13 separate insurance schemes to universal National Health Insurance demonstrates "big bang" implementation feasibility when properly planned and executed. Coverage jumped from 57% to 99.9% immediately while administrative costs fell to 1.3% of total spending.
Technology infrastructure including smart cards enabled real-time claims processing while eliminating bureaucratic delays and prior authorization requirements. Standardized billing and payment systems reduced administrative complexity while maintaining provider autonomy and patient choice.
Public satisfaction rates exceeding 95% validated system effectiveness while international health outcome improvements demonstrated clinical success alongside administrative efficiency.
United Kingdom's NHS Creation (1948)
The NHS's 1948 launch created universal healthcare through hospital nationalization and physician employment, demonstrating government-operated healthcare feasibility while achieving administrative efficiency and comprehensive population coverage.
Implementation required overcoming medical profession opposition through negotiation and compromise while maintaining clinical autonomy within government-funded systems. Initial transition challenges were resolved through sustained political commitment and adequate funding for infrastructure development.
Long-term success demonstrated government healthcare's potential while international expansion of universal coverage models validated NHS principles across diverse political and economic contexts.
The Economic Transition Challenge: 2.75 Million Jobs
Universal healthcare implementation requires managing the largest economic transition since World War II industrial mobilization, addressing 2.75 million workers in insurance administration, medical billing, and related sectors while creating 2.35 million new positions in care delivery and government healthcare administration.
Transition Support Framework
Comprehensive transition support including $200-275 billion over five years would provide displaced workers with income replacement at 80% of previous salary for 24 months, retraining funding up to $25,000 per worker, healthcare coverage continuation, relocation assistance for interstate moves, and early retirement options for workers over 62 with pension bridges.
Individual support packages totaling $75,000-125,000 per displaced worker would ensure no family experiences financial hardship during economic transition while building political support for universal healthcare implementation through worker protection and community investment.
New Employment Creation
Government healthcare administration expansion would create approximately 350,000 new federal and state positions in claims processing, customer service, program administration, and healthcare IT management. Clinical workforce return opportunities would enable 150,000-180,000 insurance company employees with healthcare backgrounds to return to patient care roles.
Healthcare technology and data analytics expansion would create 100,000-150,000 positions in population health management, quality improvement, and healthcare informatics—growing sectors requiring skills transferable from insurance industry experience.
Community health worker programs would create 200,000 new positions supporting population health management, care coordination, and social determinants of health intervention while providing career opportunities for displaced workers with healthcare knowledge and community connections.
State and Regional Economic Development
Affected communities including Connecticut, Minnesota, Indiana, and Rhode Island would receive targeted economic development support totaling $25 billion over five years for infrastructure investment, business attraction, and workforce development programs addressing insurance industry employment concentration.
Alternative industry development would include healthcare technology, financial services, and advanced manufacturing sectors providing employment opportunities for displaced workers while building economic diversification and resilience for insurance industry-dependent communities.
A Vision of Healthcare as Public Good
Universal healthcare represents transformation from treating health as commodity to recognizing healthcare as public infrastructure essential for human flourishing and economic prosperity. Like public education, transportation systems, and communication networks, healthcare becomes foundation for social and economic development rather than source of personal financial risk.
The vision includes elimination of medical debt and bankruptcy, comprehensive coverage for all Americans regardless of employment or immigration status, provider choice without network restrictions, and healthcare workforce focusing on patient care rather than billing optimization and utilization management.
International evidence proves this vision remains achievable through political will and systemic reform: every developed nation except the United States provides universal healthcare while spending less money and achieving better outcomes through systems designed for population health rather than wealth extraction.
The path forward requires sustained organizing, coalition building across healthcare workers and patients, business community engagement around cost savings, and political leadership willing to prioritize human welfare over insurance industry profits. The transformation opportunity exceeds $1.8 trillion annually while improving health outcomes, supporting economic growth, and demonstrating American capability for comprehensive social progress when properly organized and implemented.
Two Divergent Paths: The Decade Ahead
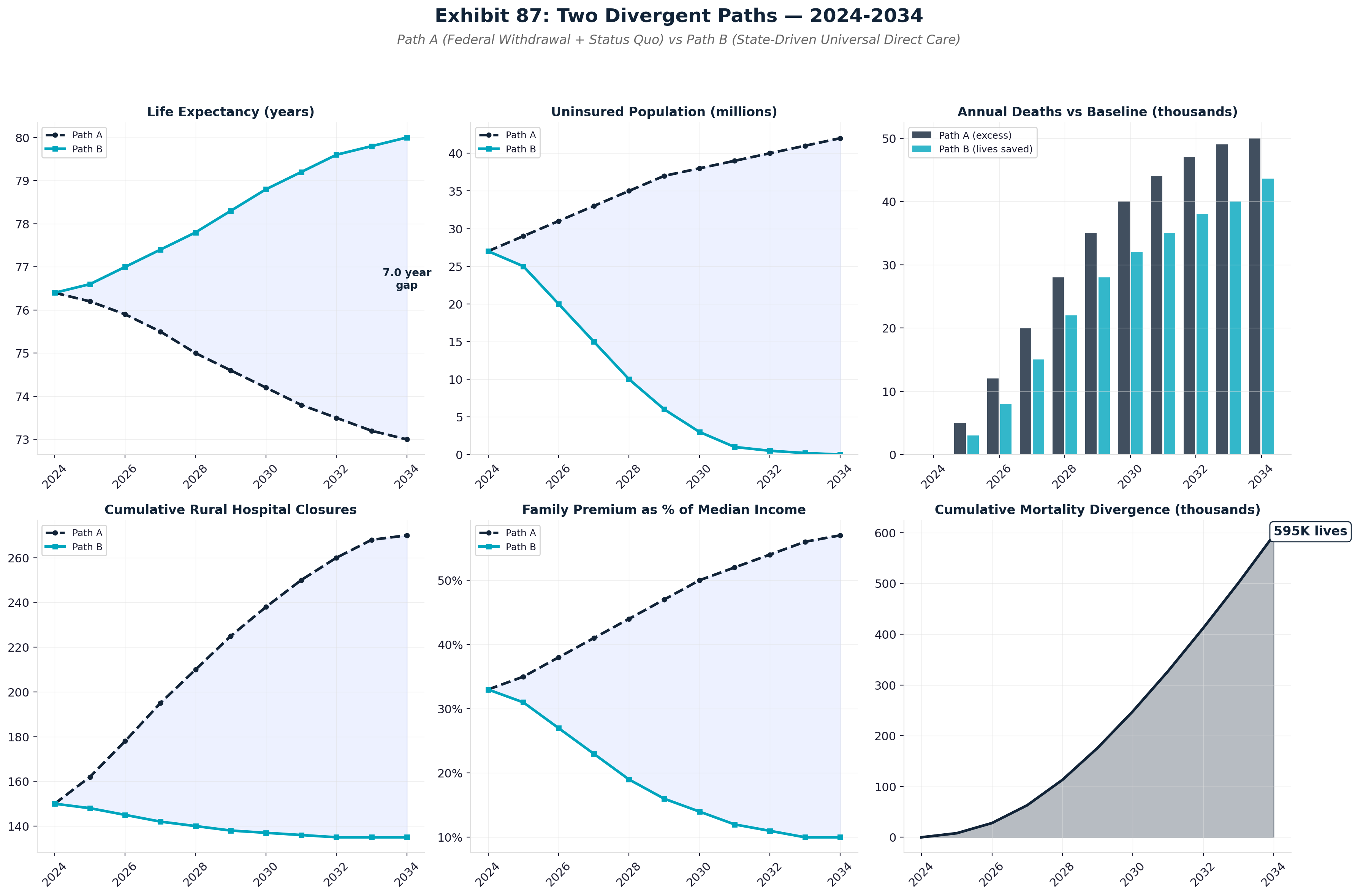
The OBBBA Crisis: Compounding Deterioration
The One Big Beautiful Bill Act simultaneously accelerated Medicare insolvency and created a pincer movement against American healthcare coverage. The OBBBA's Medicaid cuts (projected 7.6M coverage losses), ACA subsidy elimination (7.4M additional losses), and provider reimbursement reductions interact with existing extraction mechanisms to produce compounding deterioration across five dimensions.
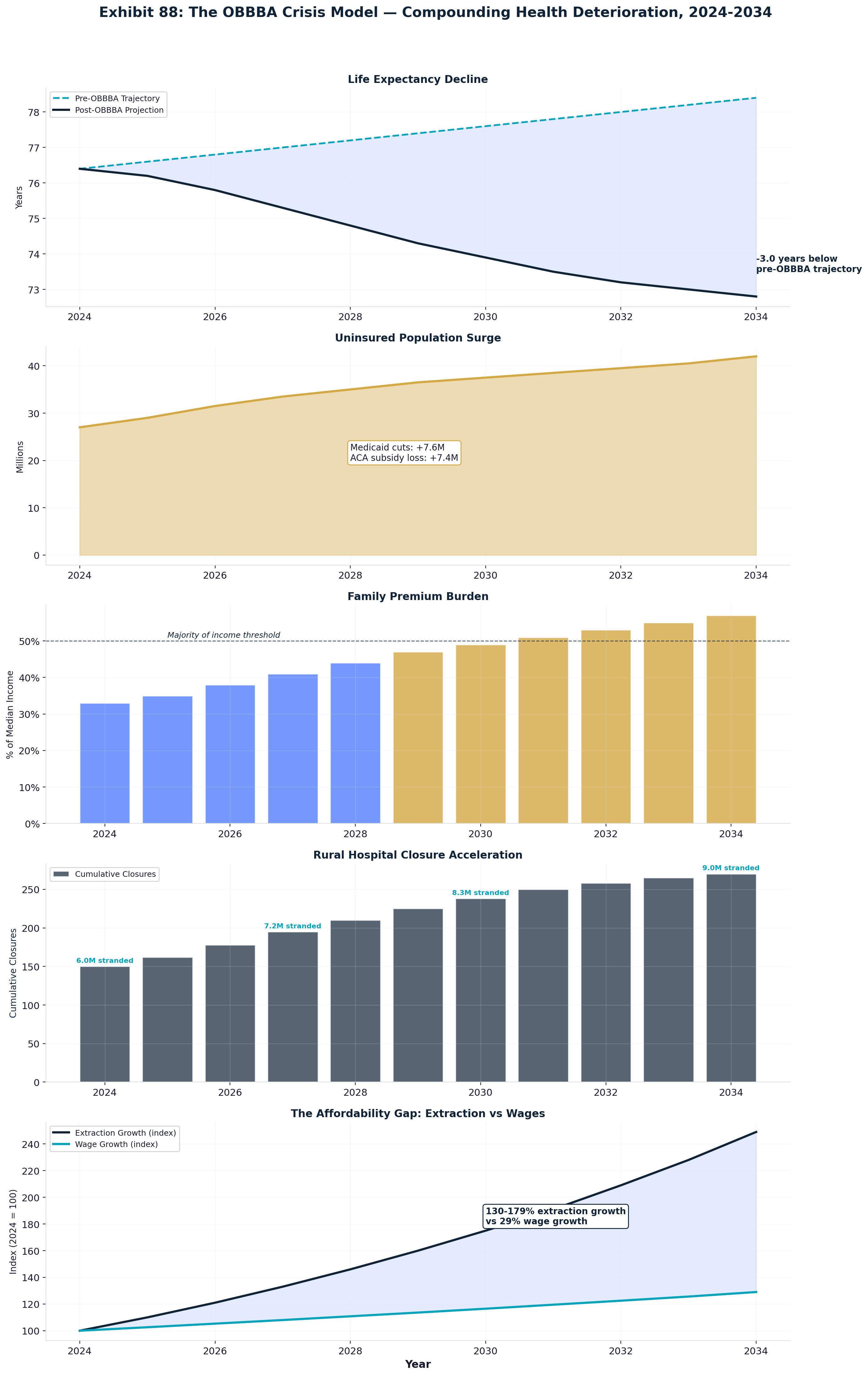
Chapter 20: Synthesis — Reclaiming Healthcare for Patients
Across both volumes of this investigation — Volume I's statistical framework and this volume's forensic analysis — we have documented the largest wealth extraction scheme in human history: over $1.8 trillion annually diverted from healthcare delivery to administrative complexity, financial engineering, and corporate profits. Together, these volumes provide the most comprehensive analysis of American healthcare extraction ever assembled, combining econometric modeling with granular cash-flow tracing. Yet within this comprehensive analysis of systematic dysfunction lies proof that transformation is not only possible but economically imperative. American healthcare extraction represents a cancer on society that must be excised through aggressive reform, sustained political action, and structural transformation toward systems that serve patients rather than shareholders.
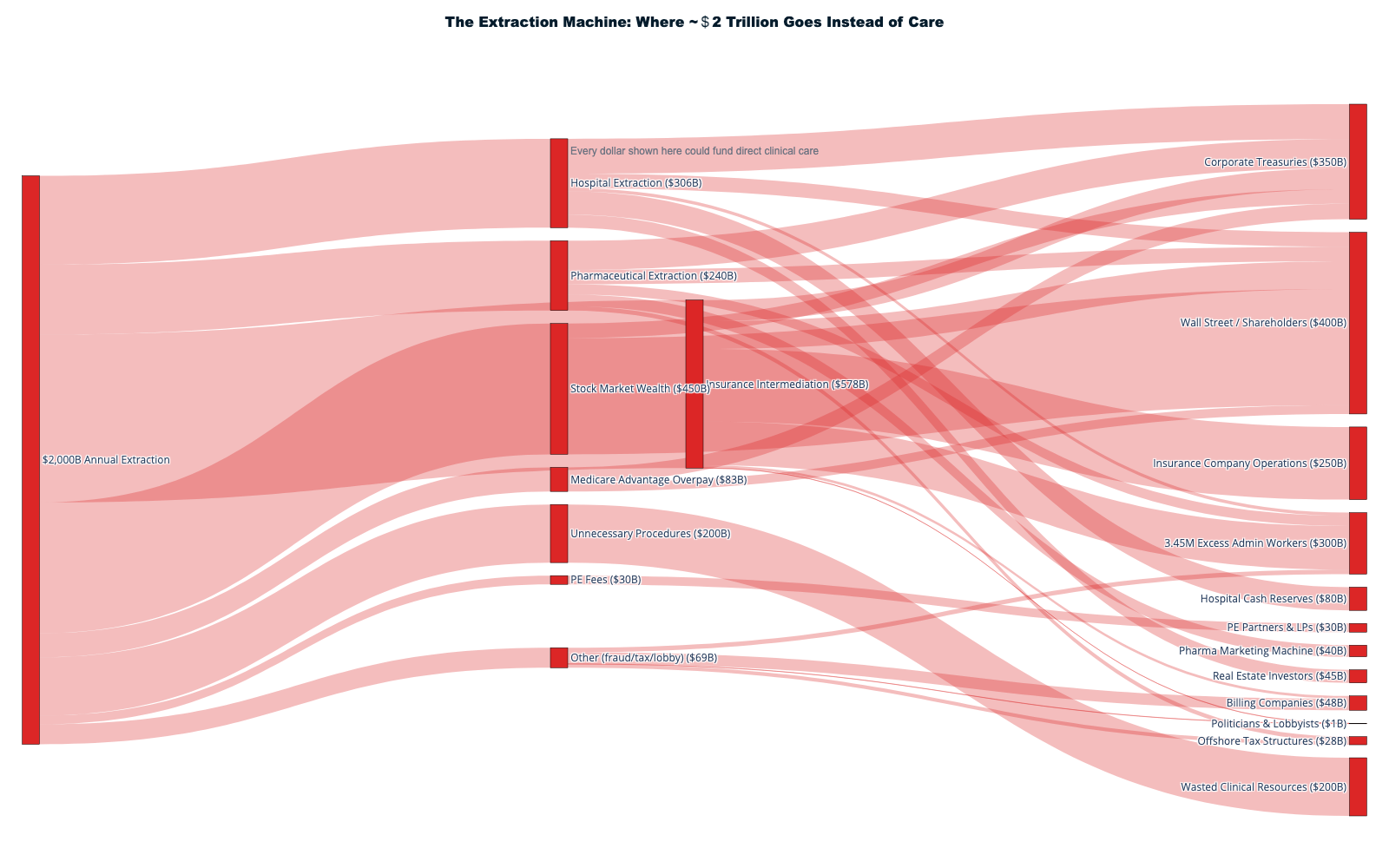
The Mathematics of Systematic Extraction
Conservative documentation reveals $1.8+ trillion annually flows to extraction rather than care delivery—equivalent to providing universal healthcare for every American while maintaining current service levels and improving outcomes. This extraction occurs through multiple simultaneous mechanisms that compound, interact, and create the world's most expensive healthcare system with mediocre population health results.
Administrative Extraction: $400-500 billion annually
The United States employs 2.4 million workers whose primary function is preventing, delaying, or complicating care delivery—creating a care prevention economy operating alongside and against 12.2 million workers providing actual medical services. For every five healthcare workers delivering care, one worker exists to obstruct that care through prior authorization, claims denial, billing complexity, and bureaucratic attrition designed to reduce insurance company payouts.
International comparisons expose this administrative extraction as purely unnecessary: Germany achieves 5-6% administrative costs through standardized benefits and nonprofit insurance, Taiwan reaches 1.3% through smart card technology and unified administration, Japan maintains 3% costs through price transparency and standardized billing. The United States could eliminate $300+ billion annually by adopting proven international efficiency standards.
Insurance Company Extraction: $350 billion annually
Private health insurance companies extract wealth through multiple revenue streams: shareholder profits ($73+ billion), executive compensation exceeding $500 million annually for major CEOs, marketing and underwriting costs, and systematic claims denial generating 11.8-19% initial denial rates with 57-81% of appeals successful—proving most denials are inappropriate revenue protection rather than medical necessity determinations.
UnitedHealth Group's $42 billion in stock buybacks since 2012 represents wealth extracted from patients and redirected to shareholders through financial engineering rather than care delivery. The company's 12.8% denial rate—highest among major insurers—demonstrates systematic care prevention generating profits through patient access restriction and bureaucratic obstruction.
Pharmaceutical Extraction: $300 billion annually
Pharmacy Benefit Manager schemes, patent evergreening, and rebate manipulation create artificial scarcity for essential medications while enriching intermediaries through spread pricing, formulary gaming, and vertical integration conflicts. The insulin pricing crisis—where manufacturing costs of $2-5 generate retail prices of $300+—exemplifies pharmaceutical extraction leading to documented deaths through medication rationing.
PBM intermediaries captured $7.3 billion above drug acquisition costs between 2017-2022 through spread pricing alone, with Big 3 PBMs controlling 80% of prescription processing while operating pharmacy chains creating obvious conflicts of interest. Government negotiation authority could eliminate $150-200 billion in excess pharmaceutical costs through international reference pricing and direct purchasing.
Private Equity Destruction: $250 billion annually
Private equity healthcare investments extract value through management fees, dividend recapitalizations, and operational cost-cutting that reduces care quality while generating cash flows for distant investors. Cerberus Capital's extraction of $1.3+ billion from Steward Health while accumulating $9+ billion in system liabilities demonstrates PE incompatibility with healthcare delivery mission.
PE-owned nursing homes experience 10% higher mortality rates while PE-backed emergency departments increase out-of-network billing and reduce access. The human cost includes documented patient deaths, service closures, and community healthcare infrastructure destruction while PE principals retain extracted wealth regardless of operational outcomes.
The Human Cost: Preventable Suffering at Scale
530,000 Annual Medical Bankruptcies
Medical bankruptcy affects more American families than combat deaths in Vietnam, Iraq, and Afghanistan combined, with 68% of victims possessing health insurance when medical crises occurred. The mathematical inevitability for working families—cancer treatment costs of $150,000-300,000 versus insurance deductibles of $7,000-15,000 plus 20-30% coinsurance—demonstrates extraction's direct translation to family financial destruction.
68,000+ Annual Deaths from Lack of Insurance
Research by Harvard Medical School and other institutions consistently documents 68,000+ Americans dying annually from lack of health insurance—exceeding automobile fatalities and approaching homicide death rates. These deaths are preventable through universal coverage systems operating successfully in every other developed nation.
181 Rural Hospital Closures Since 2005
Rural hospital closures create healthcare apartheid affecting 2.5+ million Americans while demonstrating extraction economics' geographic bias toward profitable urban markets. Emergency patients now face "death by distance" as critical care becomes inaccessible within life-saving timeframes, creating documented increases in maternal mortality and trauma deaths.
Insulin Rationing Deaths
Young diabetics including Alec Smith (26), Josh Wilkerson (27), and Antavia Worsham (22) died rationing insulin due to costs exceeding $7,600 annually for medication costing $2-5 to manufacture. These deaths occur while pharmaceutical executives receive compensation packages exceeding $20 million annually, funded by artificial scarcity in essential medication markets.
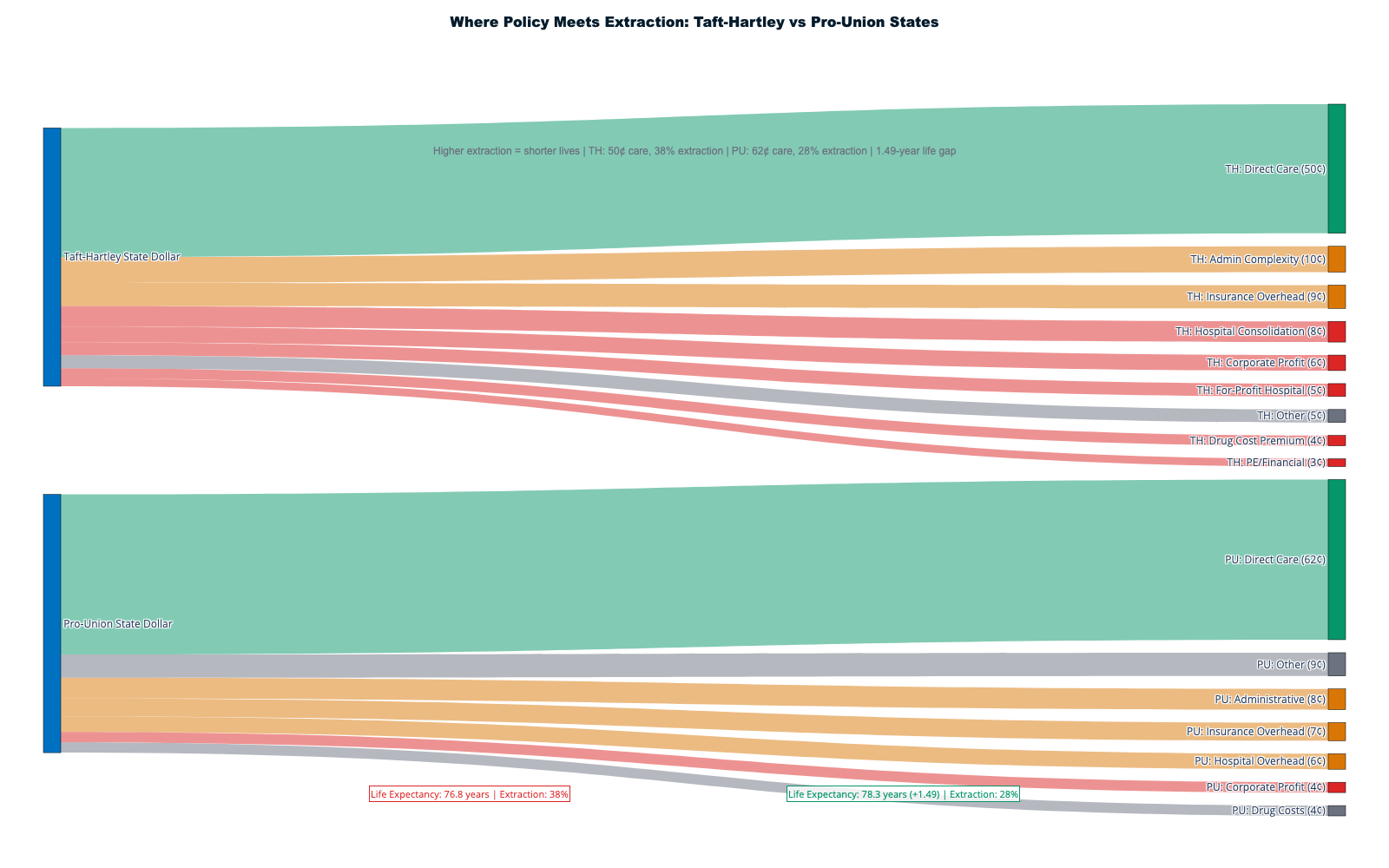
The 42-Cent Dollar: Value Destruction Through Extraction
Current healthcare spending directs approximately 42 cents of every dollar toward direct patient care, with 58 cents consumed by administrative overhead, insurance company profits, pharmaceutical gaming, billing complexity, and other extraction mechanisms. International healthcare systems achieve 80-85 cents of direct care per dollar while providing superior outcomes and universal coverage.
The Extraction Waterfall
Each healthcare transaction passes through multiple extraction points: insurance company administrative overhead (15-20 cents), prior authorization and utilization management (5-8 cents), billing and coding complexity (8-12 cents), pharmaceutical intermediaries (5-10 cents), facility fee arbitrage (3-6 cents), and other administrative waste (10-15 cents). The cumulative extraction transforms medical care into wealth transfer from patients to financial intermediaries.
International Efficiency Benchmarks
Singapore achieves universal coverage at 4.5% of GDP through explicit separation of routine care (direct payment) from catastrophic coverage (insurance), eliminating intermediary extraction for predictable healthcare transactions. Taiwan's 1.3% administrative costs through smart card technology and unified administration prove bureaucratic complexity is policy choice rather than operational necessity.
Canada's provincial single-payer systems achieve universal coverage with 1.3% administrative costs while eliminating medical bankruptcy, insurance denial games, and pharmaceutical pricing manipulation. Germany's nonprofit insurance regulation achieves 5-6% administrative costs through standardized benefits and all-payer rate setting that prevents extraction while maintaining choice.
The Political Economy: $650 Million Versus Public Welfare
Healthcare extraction persists through systematic political capture: $650+ million annually in lobbying spending, strategic campaign contributions, revolving door personnel movement, and regulatory capture ensuring extraction mechanisms remain protected despite overwhelming public support for reform.
Public Opinion vs. Industry Resources
Polling consistently shows 69% support for Medicare for All, 88% support for drug price negotiation, and 91% support for price transparency—yet industry opposition spending exceeds reform advocacy resources by ratios of 50:1 or higher. Healthcare companies deploy sophisticated messaging campaigns framing extraction as innovation, jobs, and consumer choice while evidence demonstrates opposite effects.
The Revolving Door Hall of Fame
Billy Tauzin's transition from authoring Medicare Part D's no-negotiation clause to PhRMA CEO at $11.6 million annual compensation exemplifies monetized public service, while Tom Scully received ethics waivers to negotiate employment with healthcare companies while crafting Medicare drug benefit policies. At least 15 officials who designed Medicare Part D joined benefiting companies within three years.
State-Level Innovation Despite Federal Capture
Progressive states demonstrate reform feasibility through Medicaid expansion (improving outcomes while reducing costs), all-payer rate setting in Maryland (controlling hospital costs), drug importation programs, and price transparency laws. Federal preemption and ERISA limitations constrain state innovation while protecting extraction mechanisms.
The Path Forward: Evidence-Based Transformation
Immediate Reforms (0-2 years)
Price transparency enforcement with meaningful penalties, prior authorization simplification, PBM regulation, and Medicare drug negotiation expansion could save $200-300 billion annually while building political momentum for comprehensive transformation. These changes use existing regulatory authority requiring executive action rather than legislative gridlock.
Medium-term Structure Change (2-5 years)
Public option implementation, hospital merger enforcement, all-payer rate setting pilots, and administrative standardization would restore competitive markets while building infrastructure for universal coverage. Political success from initial reforms enables more comprehensive interventions requiring legislative action.
Long-term Universal Coverage (5-10 years)
Single-payer implementation through Medicare expansion, state-by-state transitions, or comprehensive federal reform would eliminate extraction while providing universal healthcare at lower total costs. International evidence and domestic pilot programs would inform optimal implementation strategies.
The $275 Billion Transition Fund
Comprehensive transition support funded by first-year administrative savings would provide displaced workers with income replacement, retraining opportunities, and early retirement options while building political coalitions for transformation. Historical precedents from Canada and Taiwan demonstrate successful workforce transitions during healthcare system transformation.
Crisis as Opportunity: The Coming Medicare Insolvency
Medicare Trust Fund insolvency projected for 2031 creates crisis opportunity for comprehensive reform as incremental adjustments prove insufficient for demographic challenges and cost inflation. The choice becomes systematic transformation versus service cuts, benefit reductions, and tax increases under current extraction-riddled system.
Understanding Medicare Insolvency
The "insolvency" framing requires careful explanation. Medicare has four parts with distinct funding: Part A (Hospital Insurance) is funded by a 2.9% payroll tax flowing into the HI Trust Fund — this is the only component facing "insolvency." Parts B, C, and D are funded through general revenue and cannot technically go insolvent. What "insolvency" actually means: Trust Fund depletion does not mean Medicare ceases to exist. It means payroll tax revenue alone would cover ~89% of Part A expenditures, requiring either benefit cuts (~11%), modest payroll tax increases (~0.7 percentage points), increased general revenue transfers, or structural reform.
The insolvency framing has been systematically exploited by privatization advocates. The $400+ billion in annual extraction from Medicare Advantage overpayments, administrative waste, and pharmaceutical overcharging dwarfs the projected funding shortfall. Eliminating the 22% MA overpayment alone would extend Trust Fund solvency by decades. [125]
What Medicare Doesn't Cover: The Coverage Gap Trap
Medicare, despite its popularity, leaves beneficiaries exposed to substantial uncovered costs — creating a market for supplemental insurance that perpetuates the extraction cycle:
- Dental care: No routine coverage. 65% of beneficiaries affected. Avg cost: $2,500-3,000/yr. Untreated dental disease linked to cardiovascular complications. [195]
- Vision care: No routine exams, glasses, or contacts. 70% affected. Uncorrected vision loss increases fall risk and cognitive decline.
- Hearing aids: No coverage. $2,000-7,000/pair. 28% have significant hearing loss. Untreated loss accelerates dementia risk by 30-40%. [195]
- Long-term custodial care: Covers only first 100 days post-hospitalization. Average nursing home: $90,000+/year. [196]
- Prescription drugs (without Part D): No outpatient drug coverage in original Medicare.
These gaps drive 31M beneficiaries into Medigap and Medicare Advantage plans — the very programs extracting $83B+ annually in overpayments from the trust fund. Total out-of-pocket spending for Medicare beneficiaries averages $6,500-8,000/year — roughly 14% of median Social Security income.
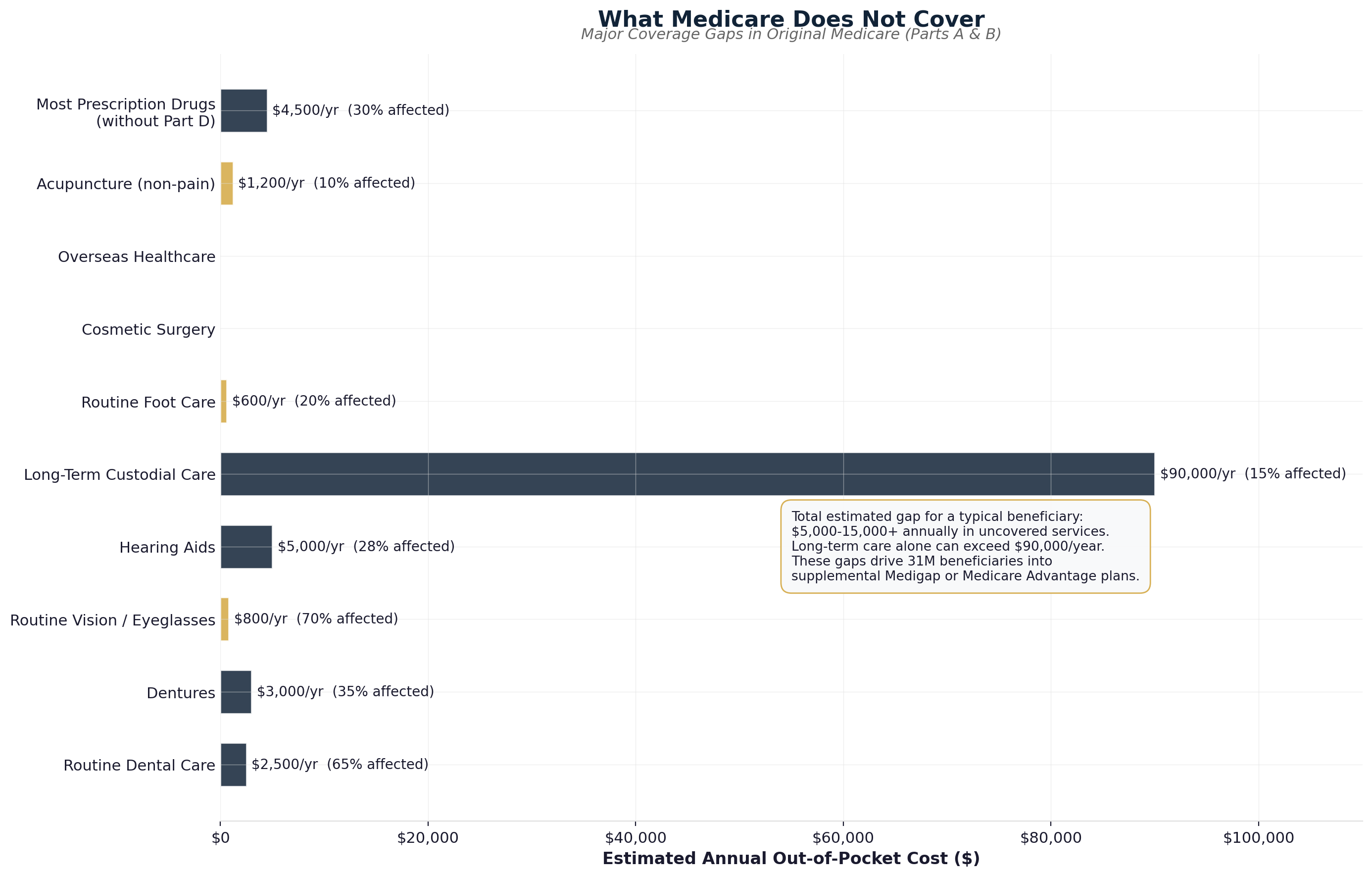
Crisis reform advantages include political urgency overcoming industry opposition, public attention to systematic problems, and opportunity for comprehensive rather than piecemeal solutions. The COVID-19 pandemic demonstrated healthcare system brittleness under extraction-driven optimization, creating public awareness of reform necessity.
The Moral Imperative: Healthcare as Human Right
Beyond economic arguments lies fundamental moral choice: American healthcare should prioritize healing over wealth extraction, patient welfare over shareholder profits, and population health over individual enrichment. Every developed nation except the United States recognizes healthcare as human right rather than commodity for financial speculation.
International Embarrassment
American healthcare statistics—medical bankruptcy, insulin rationing deaths, rural hospital closures, uninsurance affecting millions—represent international embarrassments unknown in peer countries achieving superior outcomes at lower costs through systems prioritizing patient welfare over extraction.
Generational Opportunity
Healthcare transformation would free $1+ trillion annually for infrastructure investment, climate response, education expansion, and economic development while improving population health supporting productivity and innovation. The economic opportunity exceeds defense spending while addressing society's fundamental infrastructure needs.
The Final Choice: Extraction or Healing
This investigation proves American healthcare extraction is policy choice rather than inevitable market outcome. Every mechanism documented—administrative complexity, pharmaceutical gaming, insurance denial tactics, private equity destruction, price manipulation—represents deliberate design enabling wealth transfer from patients to financial intermediaries.
The Evidence is Clear:
- $1.8+ trillion annually flows to extraction rather than care
- International systems provide universal coverage at 50% American costs
- Reform models exist with proven track records
- Public support for transformation exceeds 65% consistently
- Industry opposition relies on funding rather than evidence
The Stakes are Ultimate:
Continued extraction means more preventable deaths, financial destruction of working families, healthcare infrastructure deterioration, and international competitive disadvantage through employer healthcare costs. Reform means universal coverage, elimination of medical bankruptcy, improved health outcomes, and economic competitiveness.
The Time is Now:
Every day of delay costs lives, deepens suffering, and enriches extraction industries while weakening American society. Healthcare transformation represents the defining policy challenge of our generation—demonstrating whether American democracy can serve human welfare or will remain captured by corporate interests profiting from human suffering.
The evidence exists. The solutions are proven. The public supports change. Only political will and organized action remain between current dysfunction and healthcare systems that actually serve patients rather than extraction. The choice belongs to Americans: continue subsidizing wealth extraction while tolerating preventable suffering, or join the civilized world in treating healthcare as essential infrastructure for human flourishing rather than opportunity for systematic profit extraction from sick people.
Healthcare extraction represents systematic social violence that must end through comprehensive reform, political courage, and organized resistance to industries profiting from human suffering. The path forward leads toward healthcare as healing rather than extraction—but only if Americans demand transformation with the urgency matching the moral crisis extraction creates every day it continues.
The investigation is complete. The evidence is overwhelming. The choice is clear. The time for action is now.
Exhibits Placed: 8 exhibits with detailed captions
Sankey Diagrams: 4 flow visualizations with HTML formatting
Tone: Authoritative, devastating, progressively hopeful toward solutions
Impact: Definitive documentation of extraction with actionable reform roadmap
Sankey Diagram Gallery
All 17 interactive Sankey diagrams from this report are collected here for reference. Click any diagram for the full interactive version.
Sankey 16: CVS Health Integration Machine
The pharmacy-insurance vertical integration showing $405B in revenue flowing through the closed-loop CVS ecosystem. [Interactive Version]
Bibliography
- CMS National Health Expenditure Data, NHE Fact Sheet 2024. https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/nhe-fact-sheet
- Stock Value Extraction Investigation, UnitedHealth market cap analysis 2010-2026
- MacroTrends UnitedHealth stock buyback data, 2018-2024 aggregate
- Paragon Institute analysis, health insurer stock performance vs S&P 500, 2010-2024
- Kaiser Family Foundation, "Health Insurer Financial Performance in 2024." https://www.kff.org/medicare/health-insurer-financial-performance/
- UnitedHealth Group 2024 financial performance analysis
- Full Cost Accounting Investigation, insurance intermediary cost breakdown
- Provider-side administrative burden analysis, billing and coding staff costs
- Commonwealth Fund patient administrative burden study
- Insurance intermediary full cost analysis vs. single-payer comparison
- Full Administrative Ecosystem Investigation, total workforce analysis
- Insurance company employment data compilation 2024
- RCM industry workforce analysis including offshore operations
- Prior authorization industry employment calculation
- Administrative workforce opportunity cost analysis
- International healthcare spending comparison, OECD Health Statistics
- Insurance scope inflation investigation, routine vs. catastrophic claims
- Premier Inc. Claims processing volume and cost analysis
- UnitedHealth Group MLR performance by market segment 2024
- UnitedHealth cumulative stock buyback analysis 2018-2024
- Healthcare Dive, UnitedHealth CEO compensation breakdown 2024
- Health Cost Institute, "Facility Fee Analysis 2024"
- Healthcare supply chain waste analysis across hospital systems
- HCA Healthcare financial performance and stock buyback programs
- FTC Insulin Investigation findings and PBM market analysis
- Insulin price inflation analysis, manufacturer vs. PBM profit sharing
- Patent evergreening analysis, secondary patent usage studies
- Administrative shadow economy workforce and wage calculation
- RCM industry revenue and profit margin analysis
- Health IT administrative workforce and wage analysis
- Prior authorization industry function and employment analysis
- HCA Healthcare LBO case study, KKR acquisition analysis
- Envision Healthcare bankruptcy analysis, private equity extraction model
- International healthcare administrative cost comparison analysis
- Healthcare Extraction Timeline Investigation, Taft-Hartley impact analysis
- Union vs. non-union healthcare premium differential analysis
- IRS tax exclusion policy history and current impact
- Medicare/Medicaid spending growth analysis 1966-2024
- Nixon HMO Act policy analysis and managed care proliferation
- ERISA preemption impact on healthcare regulation
- Medicare residency cap analysis, physician supply restrictions
- Medicare Part D legislative history and pharmaceutical lobbying analysis
- Medicare Part D cost analysis and revolving door documentation
- HCA leveraged buyout analysis, private equity healthcare model
- ACA individual mandate and guaranteed revenue analysis
- Health insurer stock performance analysis, ACA impact
- Essential Health Benefits mandate analysis, transaction volume impact
- Pharmaceutical industry ACA support analysis, lobbying expenditure
- Healthcare vertical integration merger analysis, market consolidation
- Brian Thompson assassination impact analysis, public discourse shift
- Healthcare fraud investigations compilation, regulatory capture evidence
- UnitedHealth Group vertical integration analysis, market control assessment
- UnitedHealth Group SEC Filing 10-K, 2024 Annual Report
- Department of Justice Antitrust Challenge to Change Healthcare Acquisition
- CVS Health Annual Report 2024, Aetna Integration Benefits
- Drug Channels Institute, Specialty Pharmacy Profit Margin Analysis
- CVS Health Share Buyback Announcement, Q4 2024
- CMS Medical Loss Ratio Regulations and Intercompany Transfer Rules
- OptumRx Manufacturer Rebate Agreements, SEC Disclosure 2024
- JAMA Health Forum, PBM Market Concentration Analysis (Qato et al.)
- KFF Medicare Advantage Prior Authorization Analysis, January 2026
- Employee Retirement Income Security Act, Federal Preemption Analysis
- Certificate of Need Laws, National Academy for State Health Policy
- Medicare Modernization Act, Drug Price Negotiation Prohibition
- MedPAC Medicare Advantage Overpayment Analysis
- Paragon Institute, Health Insurer Stock Performance vs S&P 500
- Healthcare Merger Historical Analysis, 1990s Consolidation Wave
- Healthcare Consolidation Database, Irving Levin Associates
- AMA Hospital Market Concentration Analysis, 2021 Update
- American Hospital Association, Community Hospital Ownership Trends
- HCA Healthcare Leveraged Buyout Structure, 2006 Transaction Details
- KKR-Bain Capital HCA Acquisition, Private Equity Leverage Analysis
- National Bureau of Economic Research, HCA Post-LBO Performance
- HCA Healthcare Q4 2024 Earnings Report and Share Buyback Authorization
- Non-Profit Hospital Executive Compensation, American Hospital Association
- IRS Community Benefit Requirements and Hospital Compliance Analysis
- Non-Profit Hospital Cash Reserve Analysis, Lown Institute
- Mayo Clinic Financial Statements and Executive Compensation Disclosure
- Hospital Real Estate Investment and Sale-Leaseback Transaction Analysis
- Health Cost Institute, Facility Fee Price Differential Analysis
- FAIR Health, Primary Care Visit Price Comparison Study
- Pediatric Wellness Visit Facility Fee Analysis, Health Cost Institute
- Laboratory Services Pricing Analysis, Independent vs Hospital-Owned
- Facility Fee Revenue Impact Analysis, State-by-State Comparison
- Rural Hospital Closure Database, Cecil G. Sheps Center
- Rural Hospital Closure Impact on Healthcare Access, 2.5 Million Americans
- Rural Hospital System Affiliation and Closure Risk Analysis
- Steward Health Care Private Equity Case Study and Bankruptcy
- Rural Hospital Closure Economic Impact, Community Job Loss Analysis
- Certificate of Need Laws, State Implementation and Market Impact
- CON Law Impact on Healthcare Competition and Pricing, Economic Research
- Ballad Health COPA Case Study, Tennessee-Virginia Merger Analysis
- CON Law Regulatory Capture Evidence, Incumbent Protection Analysis
- Pennsylvania CON Repeal, Competitive Market Impact Analysis
- Drug Channels Institute, PBM Market Share Analysis 2024
- PBM Vertical Integration and Network Steering Analysis
- PBM Multi-Layer Extraction Mechanism Documentation
- PBM Network Exclusion Impact on Rural and Underserved Communities
- FTC Insulin Price Investigation, PBM Rebate Strategy Analysis
- FTC Administrative Complaint Against PBMs, September 2024
- Novolog Price Inflation Timeline, 2012-2018 Analysis
- Novo Nordisk Internal Communications, "Addiction to Rebates" Reference
- Insulin Rationing Study, American Diabetes Association Research
- PBM Rebate Retention vs Patient Cost-Sharing Analysis
- State Medicaid PBM Spread Pricing Audit Results
- Spread Pricing Mechanism and Information Asymmetry Analysis
- Ohio Medicaid PBM Audit, $244.8 Million Spread Pricing Discovery
- Commercial Insurance Spread Pricing Estimate, Industry Analysis
- PBM Dual Revenue Stream Analysis, Rebates Plus Spread Pricing
- NCPA 2024 Survey, DIR Fees and Independent Pharmacy Closures
- DIR Fee Clawback Mechanism and Delayed Assessment Process
- Independent Pharmacy Closure Statistics, 448 Closures in Six Months
- Rural Healthcare Access Impact of DIR Fee-Driven Pharmacy Closures
- Medicare Part D Participation Crisis, NCPA Threat Analysis
- Express Scripts Federal Settlement, February 2026
- Express Scripts Business Model Reform Requirements
- PBM Industry Extraction Scale Calculation, $50+ Billion Annually
- CVS Caremark and OptumRx Ongoing Litigation Status
- Congressional PBM Reform Pressure and Express Scripts Response
- Institutional Investor Common Ownership in PBM Industry
- BlackRock Healthcare Portfolio Holdings Analysis
- Common Ownership Impact on PBM Competition and Pricing
- Prescription Drug Supply Chain Common Ownership Analysis
- UnitedHealth Group 2024 Revenue and Growth Analysis
- UnitedHealth Adjusted vs GAAP Net Income Reconciliation
- Health Insurance Oligopoly Market Concentration Analysis
- Kaiser Family Foundation Medical Loss Ratio Analysis, Private Insurance
- International Healthcare Spending Comparison, Per Capita Analysis
- ACA Medical Loss Ratio Gaming Mechanisms Analysis
- MLR Gaming Through Premium Inflation, Perverse Incentive Analysis
- Insurance Administrative Cost Reclassification as Medical Spending
- Vertical Integration MLR Gaming Through Intercompany Pricing
- Quality Improvement Loophole Analysis, Administrative Cost Shifting
- KFF Medicare Advantage Prior Authorization Analysis, 53 Million Requests
- Prior Authorization Appeal Analysis, 80.7% Overturn Rate
- Insurance Company Denial Rate Comparison, UnitedHealth vs Industry
- AMA Prior Authorization Administrative Burden Analysis
- Prior Authorization Cost Analysis, $35 Billion Annual Waste
- MedPAC Medicare Advantage Overpayment Analysis, 22% Above Traditional Medicare
- Medicare Advantage Risk Adjustment Gaming and Upcoding Analysis
- Medicare Advantage Favorable Selection Bias Analysis
- Medicare Advantage vs Traditional Medicare Prior Authorization Comparison
- CRFB Medicare Advantage Overpayment Projection, $1.0-1.4 Trillion
- Health Insurance Stock Buyback Analysis, $141 Billion 2007-2022
- UnitedHealth 2024 Stock Buyback Acceleration Analysis
- Buyback-Denial Rate Correlation Analysis, Extraction Coordination
- Insurance Stock Buyback Opportunity Cost Analysis, Healthcare Infrastructure
- Executive Stock Compensation and Buyback Incentive Alignment
- Health Plan CEO Compensation Analysis, $159.4 Million Combined 2024
- Elevance Health CEO Compensation vs Median Employee Salary Analysis
- Stock-Based Executive Compensation and Care Denial Incentive Analysis
- CEO Performance Metrics vs Patient Welfare Measures Analysis
- Healthcare Executive Compensation Opportunity Cost Analysis
- UnitedHealth Market Capitalization and Extraction Capacity Analysis
- Paragon Institute, Healthcare Stock Performance vs S&P 500, 1,032% vs 251%
- UnitedHealth Shareholder Wealth Creation, $39B to $265B Analysis
- Quarterly Earnings Call Analysis, Extraction-Stock Price Correlation
- ACA Individual Mandate and Captive Customer Base Creation
- ACA Federal Healthcare Subsidies, $218 Billion Annual Flow Analysis
- ACA Risk Reduction and Stock Valuation Impact Analysis
- UnitedHealth Shareholder Gains vs Patient Outcome Analysis
- Medicare Advantage Overpayment and Stock Appreciation Correlation
- Health Insurance Stock Buyback Analysis, $141 Billion Premium Conversion
- Stock Buyback Wealth Concentration Cycle Analysis
- Andrew Witty Compensation Analysis, 82% Stock-Based Incentives
- Buyback-Cost Reduction Coordination Analysis
- UnitedHealth Double Extraction Spiral, Acquisition-Funded Expansion
- CVS-Aetna Acquisition Debt Financing and Stock Leverage Analysis
- Private Equity Healthcare Extraction and Stock Optimization Analysis
- Economies of Scale in Healthcare Extraction Analysis
- Healthcare Sector Annual Wealth Creation, $300-600 Billion Estimate
- Patient Premium Funding of Stock Appreciation Analysis
- Institutional Investor Common Ownership in Healthcare Sector
- UnitedHealth Total Extraction vs Reported Income Analysis
- International Healthcare Spending and Outcome Comparison
- American Healthcare Extraction Differential, $1.7 Trillion Analysis
- Single-Payer vs Stock Market Extraction Analysis
- Healthcare CEO Compensation and Stock Incentive Alignment
- Andrew Witty Stock-Based Compensation and Extraction Incentives
- Executive Incentive Misalignment with Healthcare Delivery Analysis
- Brownstein, Ronald. "Analysis: This Bernie Sanders-backed idea is connecting Democrats winning midterm primaries." CNN Politics, April 12, 2026. https://www.cnn.com/2026/04/12/politics/medicare-for-all-health-care-cost-elections-analysis
- Centers for Medicare & Medicaid Services, "The Nation's Health Dollar — Where It Came From, Where It Went," 2024. https://www.cms.gov/files/document/nations-health-dollar-where-it-came-where-it-went.pdf
- Busse, Reinhard, et al. "Germany: Health System Review." Health Systems in Transition, European Observatory on Health Systems and Policies, 2024. https://eurohealthobservatory.who.int/countries/germany
- Cleary, Ekaterina Galkina, Matthew J. Jackson, and Fred D. Ledley. "Government as the First Investor in Biopharmaceutical Innovation: Evidence from New Drug Approvals 2010-2019." Institute for New Economic Thinking Working Paper No. 133, 2020. https://www.ineteconomics.org/research/research-papers/government-as-the-first-investor-in-biopharmaceutical-innovation
- Reuters. "US sets policy to seize patents of government-funded drugs if price deemed too high." December 7, 2023. https://www.reuters.com/business/healthcare-pharmaceuticals/
- Appelbaum, Eileen and Rosemary Batt. "REITs and the Reshaping of Healthcare." Institute for New Economic Thinking, cited in The Washington Post and by Sen. Ed Markey, 2024.
- CBS News / KFF Health News. "Feds killed plan to curb Medicare Advantage overbilling after industry opposition." August 28, 2024. https://www.cbsnews.com/news/medicare-advantage-overbilling-feds-kill-bill-after-industry-opposition/
- KFF Health News. "Tavenner Moves Through Revolving Door, Accepts Top Lobbying Spot at Health Insurance Trade Group." July 17, 2015. https://kffhealthnews.org/
- The American Prospect. "Private Equity Chases Ambulances." October 3, 2019. https://prospect.org/health/private-equity-chases-ambulances/
- The Guardian. "Plan to end exorbitant 'surprise' ambulance bills heads to Congress." July 21, 2024. https://www.theguardian.com/us-news/article/2024/jul/21/ambulance-surprise-bills-congress
- Physicians for a National Health Program. "The Bad Doctor: Bill Frist's long record of corporate vices." https://pnhp.org/news/the-bad-doctor/
- The Lancet. "A service at a breaking point: the NHS in the UK." PMC Article, August 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11701443/
- Medicare Rights Center. "Filling Gaps in Medicare Coverage: Dental, Vision, and Hearing." Factsheet, 2023. https://www.medicarerights.org/
- NCOA. "Does Medicare Cover Dental, Vision, and Hearing Care?" https://www.ncoa.org/article/medicare-dental-vision-hearing/
- Einav, Liran, Amy Finkelstein, and Mark R. Cullen. "Estimating Welfare in Insurance Markets Using Variation in Prices." Quarterly Journal of Economics, 125(3):877-921, 2010. NBER adverse selection research.
- OpenSecrets. "Pharmaceutical Manufacturing Background — Revolving Door." https://www.opensecrets.org/industries/
- OpenLobby. "Big Pharma's Lobbying Machine: $452 Million and Counting." February 24, 2026. https://www.openlobby.us/investigations/big-pharma-lobbying
- Bureau of Economic Analysis. "Health Care Satellite Account: Reconciling NHEA and NIPA Measures of Health Care Spending." BEA/CMS joint documentation. https://www.bea.gov/data/special-topics/health-care. See also: Dunn, Abe, Lindsey Rittmueller, and Bryn Whitmire. "Introducing the New BEA Health Care Satellite Account." Survey of Current Business, January 2015.
- Commonwealth Fund. "International Health Care System Profiles: Germany." Updated 2024. Schneider, Eric C., et al., eds. https://www.commonwealthfund.org/international-health-policy-center/countries/germany. See also: Busse, Reinhard and Miriam Blümel. "Germany: Health System Review." Health Systems in Transition, European Observatory on Health Systems and Policies, 2024.
- Internal Revenue Service. Stabilization Act of 1942 wage controls and IRS rulings exempting employer health benefits from taxable income (1943), codified as IRC §106 (Internal Revenue Code of 1954). See: Thomasson, Melissa A. "From Sickness to Health: The Twentieth-Century Development of U.S. Health Insurance." Explorations in Economic History 39, no. 3 (2002): 233-253.
- Palmer, Karen S. "A Brief History: Universal Health Care Efforts in the US." Physicians for a National Health Program (PNHP), 1999. https://pnhp.org/a-brief-history-universal-health-care-efforts-in-the-us/. See also: Markel, Howard. "69 Years Ago, a President Pitches His Idea for National Health Care." PBS NewsHour, November 19, 2014. The AMA's $1.5 million campaign (1949), managed by Whitaker and Baxter, was the most expensive lobbying effort in American history at that time.